Transcription
PLEASE READ:THIS DOCUMENT CONTAINSINFORMATION ABOUT THEDRUGS WE COVER IN THIS PLANFHCP Medicare Rx Plus (HMO-POS)FHCP Medicare Rx (HMO)FHCP Medicare Rx Savings (HMO)FHCP Medicare Premier Plus (HMO)FHCP Medicare Flagler Advantage (HMO)FHCP Medicare Premier Advantage (HMO)2020PRESCRIPTION DRUGFORMULARY(LIST OF COVERED DRUGS)FHCP Medicare is an HMO plan with a Medicare contract. Enrollment in FHCP Medicare depends on contract renewal. Thisinformation is not a complete description of benefits.HMO coverage is offered by Florida Blue Medicare, Inc., DBA FHCP Medicare, an affiliate of Florida Blue and an IndependentLicensee of the Blue Cross and Blue Shield Association.This formulary was updated on 11/25/2020.For more recent information or other questions, please contact us at 1-833-866-6559 or, for TTY users, 1-800-955-8770.Hours are 8:00 a.m. - 8:00 p.m. local time, seven days a week from October 1 – March 31, except for Thanksgiving Day andChristmas Day. However, from April 1 - September 30, our hours are 8:00 a.m. -8:00 p.m. local time, five days a week. Youwill have to leave a message on Saturdays, Sundays and Federal holidays. We will return your call within one business day.Or visit www.fhcpmedicare.com.HPMS Approved Formulary File SubmissionID 00020556, Version Number 26Y0011 34655 C 0818 C: 08/2019
Note to existing members: This formulary has changed since last year. Pleasereview this document to make sure that it still contains the drugs you take.When this drug list (formulary) refers to “we,” “us”, or “our,” it means FHCP Medicare.When it refers to “plan” or “our plan,” it means FHCP Medicare Rx, FHCP Medicare RxPlus, FHCP Medicare Rx Savings, FHCP Medicare Premier Plus, FHCP Medicare FlaglerAdvantage, and FHCP Medicare Premier Advantage.This document includes a list of the drugs (formulary) for our plan which is current as of11/25/2020. For an updated formulary, please contact us. Our contact information,along with the date we last updated the formulary, appears on the front and back coverpages.You must generally use network pharmacies to use your prescription drug benefit.Benefits, formulary, pharmacy network, and/or copayments/coinsurance may change onJanuary 1, 2021, and from time to time during the year.What is the FHCP Medicare Rx, FHCP Medicare Rx Plus, FHCP Medicare RxSavings, FHCP Medicare Premier Plus, FHCP Medicare Flagler Advantage, andFHCP Medicare Premier Advantage Formulary?A formulary is a list of covered drugs selected by us in consultation with a team of healthcare providers, which represents the prescription therapies believed to be a necessarypart of a quality treatment program. We will generally cover the drugs listed in ourformulary as long as the drug is medically necessary, the prescription is filled at a plannetwork pharmacy, and other plan rules are followed. For more information on how tofill your prescriptions, please review your Evidence of Coverage.Can the Formulary (drug list) change?Most changes in drug coverage happen on January 1, but we may add or remove drugson the Drug List during the year, move them to different cost-sharing tiers, or addnew restrictions. We must follow Medicare rules in making these changes.Changes that can affect you this year: In the below cases, you will be affected bycoverage changes during the year: New generic drugs. We may immediately remove a brand name drug on ourDrug List if we are replacing it with a new generic drug that will appear on thesame or lower cost sharing tier and with the same or fewer restrictions. Also,when adding the new generic drug, we may decide to keep the brand name drugon our Drug List, but immediately move it to a different cost-sharing tier or addnew restrictions. If you are currently taking that brand name drug, we may not tellyou in advance before we make that change, but we will later provide you withinformation about the specific change(s) we have made.i
o If we make such a change, you or your prescriber can ask us to make anexception and continue to cover the brand name drug for you. The notice weprovide you will also include information on how to request an exception,and you can also find information in the section below entitled “How do Irequest an exception to the FHCP Medicare Rx, FHCP Medicare Rx Plus, FHCPMedicare Rx Savings, FHCP Medicare Premier Plus, FHCP Medicare FlaglerAdvantage, and FHCP Medicare Premier Advantage’s Formulary?” Drugs removed from the market. If the Food and Drug Administration deems adrug on our formulary to be unsafe or the drug’s manufacturer removes the drugfrom the market, we will immediately remove the drug from our formulary andprovide notice to members who take the drug. Other changes. We may make other changes that affect members currentlytaking a drug. For instance, we may add a generic drug that is not new to marketto replace a brand name drug currently on the formulary or add new restrictions tothe brand name drug or move it to a different cost-sharing tier. Or we may makechanges based on new clinical guidelines. If we remove drugs from our formulary,add prior authorization, quantity limits and/or step therapy restrictions on a drugor move a drug to a higher cost-sharing tier, we must notify affected members ofthe change at least 30 days before the change becomes effective, or at the timethe member requests a refill of the drug, at which time the member will receive a31-day supply of the drug.o If we make these other changes, you or your prescriber can ask us to makean exception and continue to cover the brand name drug for you. The noticewe provide you will also include information on how to request an exception,and you can also find information in the section on page iv entitled “How doI request an exception to the FHCP Medicare Rx, FHCP Medicare Rx Plus,FHCP Medicare Rx Savings, FHCP Medicare Premier Plus, FHCP MedicareFlagler Advantage, and FHCP Medicare Premier Advantage’s Formulary?”Changes that will not affect you if you are currently taking the drug. Generally, ifyou are taking a drug on our 2020 formulary that was covered at the beginning of theyear, we will not discontinue or reduce coverage of the drug during the 2020 coverageyear except as described above. This means these drugs will remain available at thesame cost-sharing and with no new restrictions for those members taking them for theremainder of the coverage year.The enclosed formulary is current as of 11/25/2020. To get updated information aboutthe drugs covered by our plan, please contact us. Our contact information appears onthe front and back cover pages. Our plan issues monthly formulary updates to ourwebsite (www.fhcpmedicare.com) and in print by request.ii
How do I use the Formulary?There are two ways to find your drug within the formulary:Medical ConditionThe formulary begins on page 3. The drugs in this formulary are grouped intocategories depending on the type of medical conditions that they are used to treat.For example, drugs used to treat a heart condition are listed under the category,“Cardiovascular Agents”. If you know what your drug is used for, look for thecategory name in the list that begins on page 1. Then look under the category namefor your drug.Alphabetical ListingIf you are not sure what category to look under, you should look for your drug in theIndex that begins on page 73. The Index provides an alphabetical list of all of thedrugs included in this document. Both brand name drugs and generic drugs arelisted in the Index. Look in the Index and find your drug. Next to your drug, you willsee the page number where you can find coverage information. Turn to the pagelisted in the Index and find the name of your drug in the first column of the list.What are generic drugs?Our plan covers both brand name drugs and generic drugs. A generic drug isapproved by the FDA as having the same active ingredient as the brand namedrug. Generally, generic drugs cost less than brand name drugs.Are there any restrictions on my coverage?Some covered drugs may have additional requirements or limits on coverage. Theserequirements and limits may include: Prior Authorization: Our plan requires you or your physician to get priorauthorization for certain drugs. This means that you will need to get approvalfrom us before you fill your prescriptions. If you don’t get approval, we may notcover the drug. Quantity Limits: For certain drugs, our plan limits the amount of the drug thatwe will cover. For example, our plan provides 31 tablets per prescription forJanuvia 50mg. This may be in addition to a standard one-month or three-monthsupply. Step Therapy: In some cases, our plan requires you to first try certain drugs totreat your medical condition before we will cover another drug for that condition.For example, if Drug A and Drug B both treat your medical condition, we may notcover Drug B unless you try Drug A first. If Drug A does not work for you, we willthen cover Drug B.iii
You can find out if your drug has any additional requirements or limits by looking in theformulary that begins on page 3. You can also get more information about therestrictions applied to specific covered drugs by visiting our Web site. We have postedon line documents that explain our prior authorization and step therapy restrictions. Youmay also ask us to send you a copy. Our contact information, along with the date welast updated the formulary, appears on the front and back cover pages.You can ask us to make an exception to these restrictions or limits or for a list of other,similar drugs that may treat your health condition. See the section, “How do I requestan exception to the FHCP Medicare Rx, FHCP Medicare Rx Plus, FHCP Medicare RxSavings, FHCP Medicare Premier Plus, FHCP Medicare Flagler Advantage, and FHCPMedicare Premier Advantage’s formulary?” below for information about how to requestan exception.What if my drug is not on the Formulary?If your drug is not included in this formulary (list of covered drugs), you should firstcontact Member Services and ask if your drug is covered.If you learn that we do not cover your drug, you have two options: You can ask Member Services for a list of similar drugs that are covered by us.When you receive the list, show it to your doctor and ask him or her to prescribe asimilar drug that is covered by us. You can ask us to make an exception and cover your drug. See below forinformation about how to request an exception.How do I request an exception to the FHCP Medicare Rx, FHCP Medicare RxPlus, FHCP Medicare Rx Savings, FHCP Medicare Premier Plus, FHCP MedicareFlagler Advantage, and FHCP Medicare Premier Advantage’s Formulary?You can ask our plan to make an exception to our coverage rules. There are severaltypes of exceptions that you can ask us to make. You can ask us to cover a drug even if it is not on our formulary. If approved, thisdrug will be covered at a pre-determined cost-sharing level, and you would not beable to ask us to provide the drug at a lower cost-sharing level. You can ask us to cover a formulary drug at a lower cost-sharing level if this drugis not on the specialty tier. If approved this would lower the amount you must payfor your drug. You can ask us to waive coverage restrictions or limits on your drug. For example,for certain drugs, we limit the amount of the drug that we will cover. If your drughas a quantity limit, you can ask us to waive the limit and cover a greater amount.iv
Generally, we will only approve your request for an exception if the alternative drugsincluded on the plan’s formulary, the lower cost-sharing drug or additional utilizationrestrictions would not be as effective in treating your condition and/or would cause youto have adverse medical effects.You should contact us to ask us for an initial coverage decision for a formulary, orutilization restriction exception. When you request a formulary or utilizationrestriction exception you should submit a statement from your prescriber orphysician supporting your request. Generally, we must make our decision within 72hours of getting your prescriber’s supporting statement. You can request an expedited(fast) exception if you or your doctor believes that your health could be seriouslyharmed by waiting up to 72 hours for a decision. If your request to expedite is granted,we must give you a decision no later than 24 hours after we get a supporting statementfrom your doctor or other prescriber.What do I do before I can talk to my doctor about changing my drugs orrequesting an exception?As a new or continuing member in our plan, you may be taking drugs that are not onour formulary. Or, you may be taking a drug that is on our formulary but your ability toget it is limited. For example, you may need a prior authorization from us before youcan fill your prescription. You should talk to your doctor to decide if you should switchto an appropriate drug that we cover or request a formulary exception so that we willcover the drug you take. While you talk to your doctor to determine the right course ofaction for you, we may cover your drug in certain cases during the first 90 days you area member of our plan.For each of your drugs that is not on our formulary or if your ability to get your drugs islimited, we will cover a temporary 31-day supply. If your prescription is written for fewerdays, we’ll allow refills to provide up to a maximum 31-day supply of medication. Afteryour first 31-day supply, we will not pay for these drugs, even if you have been amember of the plan less than 90 days.If you are a resident of a long-term care facility and you need a drug that is not on ourformulary or if your ability to get your drugs is limited, but you are past the first 90 daysof membership in our plan, we will cover a 31-day emergency supply of that drug whileyou pursue a formulary exception.Note: Circumstances exist in which unplanned transitions for current members couldarise and in which prescribed drug regimens may not be on the formulary. Thesecircumstances usually involve level of care changes in which a member is changing fromone treatment setting to another. For these unplanned transitions, you must use theexceptions and appeals processes. Coverage determinations and redeterminations willbe processed as expeditiously as your health condition requires.v
In order to prevent a temporary gap in care when a member is discharged to home,members are permitted to have a full outpatient supply available to continue therapyonce their limited supply provided at discharge is exhausted. This outpatient supply isavailable in advance of discharge from a Medicare Part A covered stay.When a member is admitted to or discharged from an LTC facility and does not haveaccess to the remainder of the previously dispensed prescription, a one-time override ofthe “refill too soon” edit will be provided for each medication. Early refill edits are notused to limit appropriate and necessary access to a member’s Part D benefit, and suchmembers are allowed to access a refill upon admission or discharge.For more informationFor more detailed information about your plan’s prescription drug coverage, pleasereview your Evidence of Coverage and other plan materials.If you have questions about our plan, please contact us. Our contact information, alongwith the date we last updated the formulary, appears on the front and back cover pages.If you have general questions about Medicare prescription drug coverage, please callMedicare at 1-800-MEDICARE (1-800-633-4227) 24 hours a day/7 days a week. TTYusers should call 1-877-486-2048. Or, visit http://www.medicare.gov.vi
Our Plan’s FormularyThe formulary that begins on page 3 provides coverage information about the drugscovered by us.If you have trouble finding your drug in the list, turn to the Index that begins on page73.The first column of the chart lists the drug name. Brand name drugs are capitalized(e.g., TOVIAZ) and generic drugs are listed in lower-case italics (e.g., tamsulosin).The information in the Requirements/Limits column tells you if our plan has anyspecial requirements for coverage of your drug.Usage Rules 75% Usage Rule: Prescription refills will not be covered unless at least 75% ofthe previous prescription has been used by the Member (based on the dosageschedule prescribed by the physician). 90% Usage Rule: Prescription refills for narcotics or controlled substances willnot be covered unless at least 90% of the previous prescription has been used bythe Member (based on the dosage schedule prescribed by the physician).vii
List of AbbreviationsTier 1: Preferred GenericTier 2: GenericTier 3: Preferred BrandTier 4: Non-Preferred BrandTier 5: Specialty(DL) Dispensing Limit: Cannot be dispensed for more than a 31-day supply.(LA) Limited Access: This prescription may be available only at certain pharmacies.For more information consult your Pharmacy Directory or call Member Services at 1833-866-6559, From October 1 through March 31, we are open 8 a.m. – 8 p.m. localtime, seven days a week. From April 1 through September 30, we are open 8 a.m. – 8p.m. local time, Monday – Friday. TTY users should call 1-800-955-8770.(B/D) Part B vs. Part D Prior Authorization Required: Part B vs. Part Dadministrative prior authorization required. This drug may be covered under MedicarePart B or Part D depending upon the circumstances. Part B medications must beobtained from FHCP Pharmacies.(PA) Prior Authorization: Our plan requires you or your physician to get priorauthorization for certain drugs. This means that you will need to get approval from ourplan before you fill your prescriptions. If you don’t get approval, our plan may not coverthe drug.(QL) Quantity Limits: For certain drugs, our plan limits the amount of the drug thatour plan will cover. For example, our plan provides 31 tablets per prescription forJanuvia 50mg. This appears on the formulary as “31 EA per 31 days” which meanscoverage is limited to 31 tablets every 31 days, or 1 tablet per day.(ST) Step Therapy: In some cases, our plan requires you to first try certain drugs totreat your medical condition before we will cover another drug for that condition. Forexample, if Drug A and Drug B both treat your medical condition, our plan may notcover Drug B unless you try Drug A first. If Drug A does not work for you, our plan willthen cover Drug B.Distribution Types (RO) Retail Only: Must be filled at a retail pharmacy. Mail order delivery notavailable.(RM) Retail and Mail: May be filled at a retail pharmacy or the FHCP mail orderpharmacy.(SP) Specialty Pharmacy Only: Certain drugs can only be filled via specialtypharmacies.viii
Deductible, Initial Coverage, and Coverage Gap StagesThe copayment/coinsurance amounts that you pay in each drug tier at a PreferredRetail (31-day supply), Standard Retail (31-day supply), or through FHCP’s Mail Orderpharmacy (93-day supply) are listed belowFHCP Medicare Rx Plus (HMO-POS)DeductibleNonePharmacyType/ DaySupplyInitial CoverageTier 1 Tier 2 Tier 3 Tier 4 Tier 5Preferred Retail1 Month Supply 0 3 42Standard Retail1 Month Supply 17 20 47 0 6 123Mail Order3 Month SupplyCoverage GapWe provideadditionalcoverage forprescription 10033% drugs on Tiers 1and 2 while inthe CoverageGap. Pleaserefer to ourEvidence ofNotCoverage for 273Coveredmoreinformationabout thiscoverage. 9233%FHCP Medicare Rx (HMO)DeductiblePharmacyType/ DaySupply 295 – OnlyPreferred Retailapplies to1 Month Supplydrugs inTiers 3, 4,Standard Retailand 51 Month SupplyMail Order3 Month SupplyInitial CoverageTier 1 Tier 2 Tier 3 Tier 4 Tier 5 0 7 44 9526% 17 20 47 10026% 0 18 129 282NotCoveredixCoverage GapStandardCoverage
Deductible, Initial Coverage, and Coverage Gap Stages (Continued)FHCP Medicare Premier Plus (HMO)DeductiblePharmacyType/ DaySupplyInitial CoverageTier 1 Tier 2 Tier 3 Tier 4 Tier 5NonePreferred Retail1 Month Supply 0 7 45Standard Retail1 Month Supply 17 20 47 0 18 132Mail Order3 Month SupplyCoverage GapWe provideadditional 9833% coverage forprescriptiondrugs on Tiers 1and 2 while inthe Coverage 10033% Gap. Pleaserefer to ourEvidence ofCoverage formoreNotinformation 291Coveredabout thiscoverage.FHCP Medicare Rx Savings (HMO)DeductiblePharmacyType/ DaySupply 395 – OnlyPreferred Retailapplies to1 Month Supplydrugs inTiers 3, 4,Standard Retailand 51 Month SupplyMail Order3 Month SupplyInitial CoverageTier 1 Tier 2 Tier 3 Tier 4 Tier 5 4 10 45 9825% 17 20 47 10025% 9 27 132 291NotCoveredxCoverage GapStandardCoverage
Deductible, Initial Coverage, and Coverage Gap Stages (Continued)FHCP Medicare Flagler Advantage (HMO)DeductiblePharmacyType/ DaySupplyInitial CoverageTier 1 Tier 2 Tier 3 Tier 4 Tier 5NonePreferred Retail1 Month Supply 0 5 44Standard Retail1 Month Supply 17 20 47 0 12 129Mail Order3 Month SupplyxiCoverage GapWe provideadditional 9533% coverage forprescriptiondrugs on Tiers 1and 2 while inthe Coverage 10033% Gap. Pleaserefer to ourEvidence ofCoverage formoreNotinformation 282Coveredabout thiscoverage.
Deductible, Initial Coverage, and Coverage Gap Stages (Continued)FHCP Medicare Premier Advantage (HMO)DeductiblePharmacyType/ DaySupplyInitial CoverageTier 1 Tier 2 Tier 3 Tier 4 Tier 5NonePreferred Retail1 Month Supply 0 5 44Standard Retail1 Month Supply 17 20 47 0 12 129Mail Order3 Month SupplyxiiCoverage GapWe provideadditional 9533% coverage forprescriptiondrugs on Tiers 1and 2 while inthe Coverage 10033% Gap. Pleaserefer to ourEvidence ofCoverage formoreNotinformation 282Coveredabout thiscoverage.
Table of ContentsAnalgesics.3Anesthetics. 4Anti-Addiction/ Substance Abuse Treatment Agents. 5Antibacterials. 5Anticonvulsants. 11Antidementia Agents. 14Antidepressants. 14Antiemetics. 16Antifungals. 17Antigout Agents. 19Anti-inflammatory Agents.19Antimigraine Agents. 19Antimyasthenic Agents.20Antimycobacterials. 20Antineoplastics. 20Antiparasitics.26Antiparkinson Agents. 27Antipsychotics. 28Antispasticity Agents. 31Antivirals. 31Anxiolytics. 34Bipolar Agents. 35Blood Glucose Regulators. 35Blood Products/ Modifiers/ Volume Expanders. 38Cardiovascular Agents. 40Central Nervous System Agents. 45Dental and Oral Agents. 47Dermatological Agents. 47Electrolytes/Minerals/Metals/Vitamins. 49Gastrointestinal Agents. 50Genetic or Enzyme Disorder: Replacement, Modifiers, Treatment. 51Genitourinary Agents. 51Hormonal Agents, Stimulant/ Replacement/ Modifying (Adrenal).52Hormonal Agents, Stimulant/ Replacement/ Modifying (Pituitary).54Hormonal Agents, Stimulant/ Replacement/ Modifying (Sex Hormones/ Modifiers). 55Hormonal Agents, Stimulant/ Replacement/ Modifying (Thyroid).57Hormonal Agents, Suppressant (Adrenal). 57Hormonal Agents, Suppressant (Pituitary). 57Hormonal Agents, Suppressant (Thyroid). 58Immunological Agents. 58Inflammatory Bowel Disease Agents. 62Metabolic Bone Disease Agents. 63Ophthalmic Agents. 63Otic Agents. 66Respiratory Tract/ Pulmonary Agents. 66Skeletal Muscle Relaxants. 70Sleep Disorder Agents.701
2
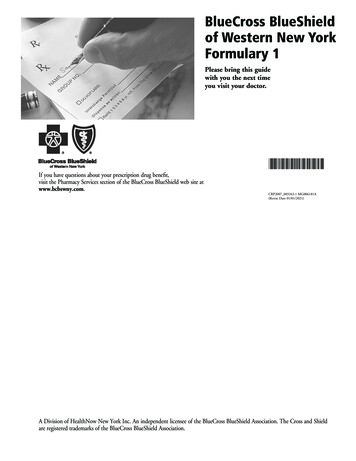
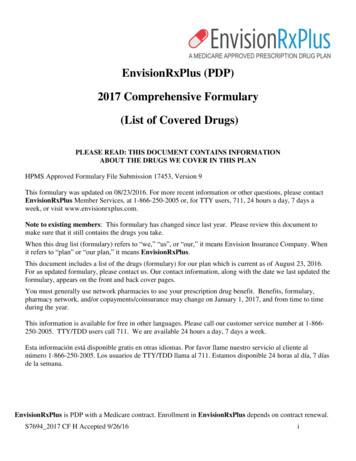
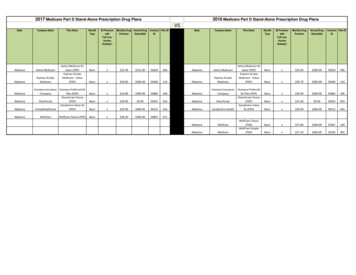
Drug -codeine #3 oral tablet300-30 mgTier 2RMacetaminophen-codeine oral solution120-12 mg/5mlTier 2RO; DLacetaminophen-codeine oral tablet300-15 mg, 300-60 mgTier 2RMbutalbital-apap-caffeine oral tablet 50325-40 mgTier 2RMbutalbital-aspirin-caffeine oral capsule50-325-40 mgTier 2RMcelecoxib oral capsule 100 mg, 200 mg,400 mg, 50 mgTier 2RMdiclofenac sodium oral tablet delayedrelease 25 mg, 50 mg, 75 mgTier 2RMetodolac er oral tablet extended release24 hour 400 mg, 500 mg, 600 mgTier 2RMetodolac oral capsule 200 mg, 300 mgTier 2RMetodolac oral tablet 400 mg, 500 mgTier 2RMfentanyl citrate buccal lozenge on ahandle 1200 mcg, 1600 mcg, 200 mcg,400 mcg, 600 mcg, 800 mcgTier 4PA; RO; QL (120 EA per 30days); DLfentanyl transdermal patch 72 hour 100mcg/hr, 12 mcg/hr, 25 mcg/hr, 50mcg/hr, 75 mcg/hrTier 2PA; RO; DLhydrocodone-acetaminophen oralsolution 7.5-325 mg/15mlTier 2RO; QL (2700 ML per 30days); DLhydrocodone-acetaminophen oral tablet10-325 mg, 5-325 mg, 7.5-325 mgTier 2RMhydromorphone hcl oral liquid 1 mg/mlTier 2RO; DLhydromorphone hcl oral tablet 2 mg, 4mg, 8 mgTier 2RMibuprofen oral tablet 400 mg, 600 mg,800 mgTier 1RMindomethacin er oral capsule extendedrelease 75 mgTier 2RMindomethacin oral capsule 25 mg, 50mgTier 2RMketorolac tromethamine oral tablet 10mgTier 2RM; QL (20 EA per 31days)3
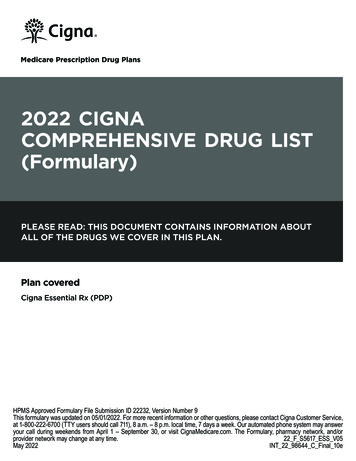
Drug NameTierRequirements/Limitsmeclofenamate sodium oral capsule100 mg, 50 mgTier 2RMmeloxicam oral tablet 15 mg, 7.5 mgTier 1RMmeperidine hcl oral tablet 100 mg, 50mgTier 2RMmethadone hcl oral solution 5 mg/5mlTier 2RO; DLmethadone hcl oral tablet 10 mg, 5 mgTier 2RMmorphine sulfate (concentrate) oralsolution 100 mg/5mlTier 2RO; DLmorphine sulfate er oral tabletextended release 100 mg, 15 mg, 200mg, 30 mg, 60 mgTier 2RMmorphine sulfate oral solution 10mg/5ml, 20 mg/5mlTier 2RO; DLmorphine sulfate oral tablet 15 mg, 30mgTier 2RMnabumetone oral tablet 500 mg, 750mgTier 2RMnaproxen oral suspension 125 mg/5mlTier 2RO; DLnaproxen oral tablet 250 mg, 375 mg,500 mgTier 1RMoxycodone hcl oral solution 5 mg/5mlTier 2RO; DLoxycodone hcl oral tablet 10 mg, 15mg, 20 mg, 30 mg, 5 mgTier 2RMoxycodone-acetaminophen oral tablet10-325 mg, 2.5-325 mg, 5-325 mg,7.5-325 mgTier 2RMpiroxicam oral capsule 10 mg, 20 mgTier 2RMsulindac oral tablet 150 mg, 200 mgTier 2RMtramadol hcl oral tablet 50 mgTier 2RMlidocaine external ointment 5 %Tier 2RO; QL (120 GM per 30days); DLlidocaine external patch 5 %Tier 2PA; RO; DLlidocaine viscous hcl mouth/throatsolution 2 %Tier 2RO; DLlidocaine-prilocaine external cream 2.52.5 %Tier 2RO; QL (30 GM per 30days); DLAnesthetics4
Drug NameTierRequirements/LimitsAnti-Addiction/ Substance AbuseTreatment Agentsacamprosate calcium oral tabletdelayed release 333 mgTier 2RMbuprenorphine hcl sublingual tabletsublingual 2 mg, 8 mgTier 2RO; DLbuprenorphine hcl-naloxone hclsublingual tablet sublingual 2-0.5 mg,8-2 mgTier 2RO; DLbupropion hcl er (smoking det) oraltablet extended release 12 hour 150mgTier 2RMCHANTIX CONTINUING MONTH PAKORAL TABLET 1 MGTier 4RO; DLCHANTIX ORAL TABLET 0.5 MG, 1 MGTier 4RMCHANTIX STARTING MONTH PAK ORALTABLET 0.5 MG X 11 & 1 MG X 42Tier 4RO
FORMULARY PRESCRIPTION DRUG (LIST OF COVERED DRUGS) PLEASE READ: THIS DOCUMENT CONTAINS INFORMATION ABOUT THE DRUGS WE COVER IN THIS PLAN HPMS Approved Formulary File Submission ID 00020556, Version Number 26 Y0011_34655_C 0818 C: 08/2019 FHCP