Transcription
20 most common dermatology diagnosesDermatology: What you need toknow in primary carePart IJessica Kaffenberger, MDAssistant Professor – ClinicalDivision of DermatologyThe Ohio State University Wexner Medical Center1.2.3.4.5.6.7.acne11. hemangiomas/port-winestainrosacea12. verruca/condylomapsoriasis13. molluscum contagiosumseborrheic dermatitis14. seborrheic keratosisatopic dermatitis15. actinic keratosiscontact dermatitis16. melanocytic nevistasis17. impetigo, folliculitis,dermatitis/ulcersabscess8. urticaria18. herpesvirus infections9. dermatophyte19. scabiesinfections20. pityriasis rosea10. tinea versicolor20 most common dermatology diagnoses1.2.3.4.5.6.7.acne11. hemangiomas/port-winestainrosacea12. verruca/condylomapsoriasis13. molluscum contagiosumseborrheic dermatitis14. seborrheic keratosisatopic dermatitis15. actinic keratosiscontact dermatitis16. melanocytic nevistasis17. impetigo, folliculitis,dermatitis/ulcersabscess8. urticaria18. herpesvirus infections9. dermatophyte19. scabiesinfections20. pityriasis rosea10. tinea versicolorHEADSHOULDERSKNEESTOES1
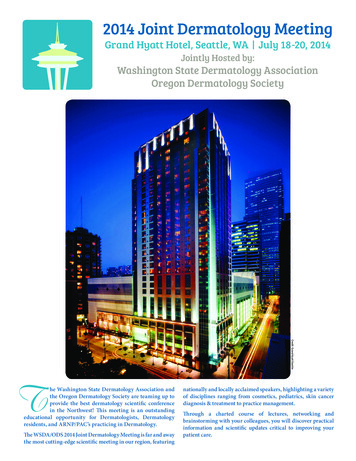
HEADSHOULDERSPSORIASISKNEESTOESPsoriasisPlaque Psoriasis Four Main types: Plaque Guttate Pustular Inverse Arthritis can be seen with any typeOSUDERM.org2
Plaque PsoriasisGuttate Psoriasis More common in children Most common type Scalp, Elbows, Knees, Sacrum Usually itches Related to strep infections Trunk most involved May resolve ular PsoriasisInverse Psoriasis Usually macerated –scale NOT visible Most acute type Can be life threatening May have fevers, highWBC Can be caused bywithdrawal of systemicsteroidsOSUDERM.orgPhoto from J.KaffenbergerPhoto from J.KaffenbergerOSUDERM.org3
TreatmentTopicalPsoriasis- Steroids: mid-strong potency- Triamcinolone 0.1%(only one that comes in atub)- Calcipotriene- Tacrolimus/Pimecrolimus:usually for inverse pso (offlabel)- Ultraviolet light: 2-3x weeklyPsoriasis Pearls:Other:- Pustular pso: call derm- AVOID systemicsteroids – can causesevere flare whenstopped PPso lifelonglif lconditionditi–choosehtherapiesthiaccordingly Make sure correct vehicle for all pso locations Scalp oil, solution, foam Body cream, ointmentSystemic- Acitretin, cyclosporine,biologics (call dermatologist) Give appropriate amount of topicalmedication(Whole body application approx 30g)OSUDERM.org Most common Face andscalp “butterfly rash”SEBORRHEICDERMATITIS Can affect intertriginousareas esp in children Yellow/greasy scaleOSUDERM.org Cause: Pityrosporum ovale /- itch4
Seborrheic dermatitisTreatment Zinc, selenium sulfide, or ketoconazoleshampoos Leave in for 3-5 min before rinsing UseU on sideid off nose andd eyebrowsbtoot Scalp: Clobetasol solution Face: Intermittent (minimize use)hydrocortisone 1-2.5%, ortacrolimus/pimecrolimusPhoto from J.KaffenbergerPhoto from J.KaffenbergerSeborrheic dermatitis pearls Manage expectations: can’t cure, can control Assoc with Parkinson’s and AIDsACNE Can overlap with psoriasis “sebopsoriasis”5
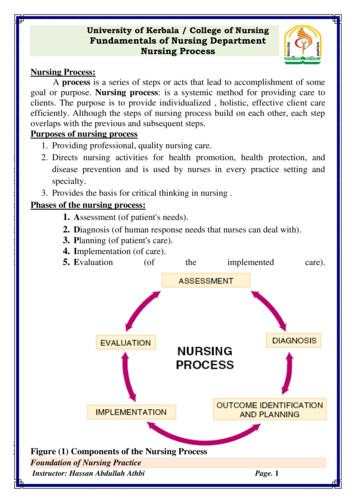
One size fits allPhoto from J.KaffenbergerOne size fits allPhoto from J.Kaffenberger1. Non-inflammatory: ComedonesPhoto from J.KaffenbergerPhoto from J.KaffenbergerPathogenesis of acne.One size fits allPhoto from J.Kaffenberger1. Non-inflammatory: Comedones2. Inflammatory Papules Pustules Nodules CystsPhoto from J.Kaffenberger6
Non-inflammatory acne- abnormal keratinization- increased sebum productionOSUDERM.orgOSUDERM.orgOpen comedones blackheadsClosed comedones whiteheadsInflammatory AcnePathogenesis: Abnormalkeratinization Increasedsebumproduction Inflammation P. acnesOSUDERM.orgLesions: PapulesPustulesNodulesCystsNon-inflammatory acne Treatment:- **Retinoid**- Adapalene- TretinoinT ti i- Tazarotene- Benzoyl peroxide wash or gel- Salicyclic acidInflammatory acne Treatment – target all causes! “Triple therapy”1. Antibioticsy y100mgg PO BID Doxycycline Minocycline 100mg PO BID Minimize course to 3-6 months2. Retinoid3. BPO7
Inflammatory acne - severeSPECIAL CASESOSUDERM.orgOSUDERM.org- Nodules 0.5cm in diameter and depth- Cysts- ScarsSevere inflammatory acneTreatment- Isotretinoin- Synthetic Vitamin A Derivative- Highly teratogenic – controlled by gov’t- Numerous A/E:-XerosisHyperlipidemia? depression/suicide? IBD- Send to derm if not part of IpledgeprogramInflammatory acne – adult female“O” distributionTreatment:- Hormonal therapy- OCPs- 3 “approved”- Reality: all likely work,- Ideally pick one w/ low androgenicprogestin- (norgestimate, desogestrel, drospirenone,3rd gen progestins)- Spironolactone (off-label)- Blocks androgens- Dose: 50mg BID, can increase to 100mg POBID- S.E.: Breast tenderness, irreg periods,headache, feminization of male fetus8
Acne pearls Biggest cause of treatment failure: Poorcompliance * Counsel – takes 2-3 months fortherapy to work!ROSACEA Diet and acne .the jury is still outRosaceaRosacea4 Types:1 Erythrotelangiectatic1.2. Papulopustular3. Phymatous4. OcularOSUDERM.orgOSUDERM.orgOSUDERM.org9
RosaceaTreatment:1. Erythrotelangiectatic Aug 2013: Brimonidine topical gel, 0.33% Alpha-2 adrenergic agonist2. Papulopustular MetrogelM tl or metrocreamt Oral doxycycline (off-label) Anti-inflammatory dosing3. Ocular Oral doxycycline (off-label)4. Phymatous Surgery/ Shaw scalpelRhinophymaOSUDERM.orgOSUDERM.orgRosacea pearls Anti-inflammatory dosing of doxycycline Doxycycline 20mg PO BID, 40mg PO daily,50mg PO BID Effective Lower incidence of GI side effectsACTINICKERATOSES Ask about eye symptoms Dry, gritty eyes Need oral doxycycline10
Actinic KeratosesOSUDERM.orgTreatment: Cryotherapy “Field therapy”: 5-fluorouracil,imiquimod, diclofenac New therapy: ingenol mebutate Intracellular protein kinase C agonist cellular necrosis Also immunostimulatory getcytotoxic Ts against dysplastic cells Face 0.015% x 3 days,Trunk/extremities 0.05% x 2 days Face/scalp: 83% median reduction,Trunk: 75% median reductionActinic keratoses pearls Don’t need to treat them all – treatbothersome areasIMPETIGO Field therapy – can be difficult espfor elderly pts11
ImpetigoPhoto from J.Kaffenberger Most common: S.aureus “Honey-colored”crusts more thanpustules More superficial thanecthyma More likely in kids w/atopic dermTreatment: Topical antibiotic,antibacterial wash More severe: oralantibiotic(cephalexin)Managing the“STAT acneconsult”lt”When to consultyour localdermatologist?dt l i t?Common rashes in primarycare Part 2:Ben Kaffenberger, MDAssistant ProfessorDivision of DermatologyThe Ohio State University Wexner Medical Center12
Objectives (I can Identify common patterns of)1. Dermatitis/EczemasA. Atopic DermatitisB. Asteatotic eczema (Eczema craquele)C. Allergic/Irritant Contact DermatitisD. Stasis DermatitisE. Dermatophyte infectionsF. Tinea VersicolorG. Scabies2. Urticaria3. Hidradenitis Suppurativa4. Severe cutaneous adverse reactions fromdrugsPsoriasis AtopicDermatitisTopical Steroids You need to knowLow: Hydrocortisone 2.5% crm/ointMedium: Body – Triamcinolone 0.1%crm/ointHigh Potency: Body, thick plaques –Betamethasone dipropionateaugmented 0.05% crm/oint/lotAtopic Dermatitis13
Childhood Atopic DermatitisTreatment of Atopic Dermatitis (AD) Moisturization (most important) Avoid triggers (food allergens,infections, airborne allergens) Antihistamines Topical steroids For severe disease:Send to dermatologist!Asteatotic Eczema – EczemacraqueleAsteatotic Eczema Always elderly patients Always on the legs Worst in the wintertime Best treatment moisturization(ammonium lactate althoughtriamcinolone can be beneficialinitially)14
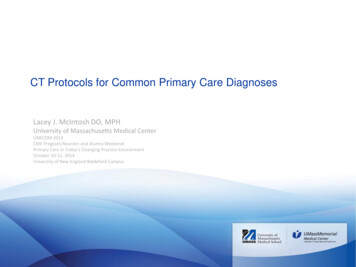
Contact DermatitisContact Dermatitis – Poison IvyToxicodendron radicans.Contact Dermatitis – Poison IvyContact Dermatitis – Nickel Very common, probably 75% of thepopulation is sensitized “Streaky Dermatitis” New spots can appear for days after rashstarts Blister fluid does not spread the rash Treat with 3 weeks of prednisone if severeotherwise high-potency topical steroids15
Contact Dermatitis – NickelContact Dermatitis – TripleAntibiotic ointment (neomycin orbacitracin) Most common cause of chronicallergic contact Common sources of exposure:Jewelry (earrings, watches, etc)Clothing (belts, snaps, rivets, etc)Coins, Keys, EyeglassesInternet for sources of nickel free jewelryContact Dermatitis - NeomycinContact Dermatitis – Fragranceand Preservatives Very common, up to 10% of thepopulation is allergic Both Neomycin (most common causeof allergic contact dermatitis fromtopical medications) and Bacitracin - If a patient has usedneomycin/bacitracin, have patientperform a “repeat open applicationtest”16
Contact Dermatitis – Fragrance andPreservativesContact Dermatitis – Perianal Face, Neck, Hands Common exposures:Shampoo, soap, conditioner, hair products,moisturizer, perfume, deodorant VVery difficultdiffi lt tot avoidid thesethsubstancesb taseven products that say “hypoallergenic” or“dermatologist tested” often havefragrances Allergic patients only react to somefragrances and preservativesIrritant Hand Dermatitis- Ask about diarrhea and use of diaper wipes- If using diaper wipes – stop and give highpotency steroidIrritant Hand Dermatitis Most commonly due to repetitive exposureto soap and water Interdigital and dorsal hands- Ask about frequency of handwashing Hand sanitizer is less damaging than soap Need thick ointment to protect17
Stasis DermatitisStasis Dermatitis For mild cases, compression is key Predisposed by lower limb injury,surgery, obesity, lymphedema, andincreased age May apply Triamcinolone underneathstockings Contact dermatitis is commonLymphedema - Stasis Dermatitis ElephantiasisTineaAsk about knownTriggers.If none pinpointed,Titrate cetirizine to20 mg daily.Can start H2blocker as well.If no improvementRefer to derm, canconsider furtherimmunosuppression18
Tinea Look for annular/arcuateappearance Also look for interdigital scale,mild tinea pedis KOH examinationi ti or skinki bibiopsywill confirm Treat with Ketoconazole 2% creambid UNLESS features suggestivefor hair-follicle involvementTinea VersicolorTinea Versicolor Upper body, summer time, young-adults,typically in humid environments Scrape with slide or fingernail, scaling canconfirm it Treat: Fluconazole 300 mg x 2, 1 wk apart For maintenance, have patient use OTCdandruff shampoo (zinc pyrithione,selenium, or ketoconazole) as body washtiw19
ScabiesScabies Finger websAsk about knownTriggers.If none pinpointed,Titrate cetirizine to 20 mg daily.Can start H2 blocker as wellwell.If no improvementRefer to derm, can consider furtherimmunosuppression Antecubital fossa Axilla Breasts/Groin Permethrin (5%)! Neck down full body –Everyone in house Everything washed in a hot cycle thefollowing AMUrticariaUrticaria - HivesAsk about knownTriggers.If none pinpointed,Titrate cetirizine to 20 mg daily.Can start H2 blocker as well.Ask about knownTriggers.If none pinpointed,Titrate cetirizine to 20 mg daily.Can start H2 blocker as well.If no improvementRefer to derm, can consider furtherimmunosuppressionIf no improvementitRefer to derm, can consider furtherimmunosuppression20
UrticariaHidradenitis suppurativa Itchy, evanescent, and transient wheels *If greater than 24 hrs in one place, it isnot urticaria!! Common causes include strepinfections drugsinfections,drugs, hymenopteraenvenomations Never scaly Titrate cetirizine (start 10 mg bid) fortreatmentHidradenitis suppurativa Treatments:Severe Cutaneous Adverse ReactionsStevens-Johnson Syndrome Topical acne treatments Weight loss Chronic antibiotics (Doxycycline 100 mgbid) ?Adalimumab, infliximab? Needs referralto dermatology. If severe and can’t get into dermatology –consider referral to plastics/gen surg forexcision and skin grafting21
Stevens-Johnson SyndromeStevens-Johnson SyndromeStevens-Johnson SyndromeLastly – Bed Bugs or Cimex lectularius Acute death of epidermis due to exposureto a medication Key early finding is pain/involvement ofmultiple mucous membranes, followed bysloughinggg of the skin Usually within 1-3 weeks of starting med Aromatic Anticonvulsants, allopurinol,Sulfa, NSAIDS, High Mortality - Stop med, calldermatology/hospital with dermatologycapabilitiesC. Wayne Elliott Plant and Pest diagnostic center.- ppdc@cfaes.osu.edu, 614-292-5006Thanks Everyone22
Anti-inflammatory dosing 3. Ocular Oral doxycycline (off-label) 4. Phymatous Surgery/ Shaw scalpel Rhinophyma OSUDERM.org OSUDERM.org Rosacea pearls Anti-inflammatory dosing of doxycycline Doxycycline 20mg PO BID, 40mg PO daily, 50mg PO BID Effective Lower