Transcription
From ABC to ADHDEric Tridas, MDAprilil 3 & 4A4, 2009The Hawai’i Branch of theInternational Dyslexia Association
The Developmental WebDevelopmental al EmotionalSocialSoca Interactionte act oHealthBehavioral &CognitiveMedicalEnvironmental
Developmental WebContributing Factorsto Clinical Presentation
Developmental ProfileVISUALPROCESSINGAUDITORYINPUTLONG NEUSSHORT TERMATTENTIONNCOGNITIVEETACTILE-KINESTHETIC
Visual Perceptual Problems KEDLIKETHIS! ORI FTH EWOR DSBE GINA NDEN DI NPLACESTH ATDON’NTM AKES ENSET OY OU? TAHW FI EHT SRETTEL EREW DESREVER, orOUT FO ODRER w re o n al paT oset aelv e g e.e ds m c er hhd t
Language Processing PhonologySemanticsMorphologyS tSyntaxDiscourseMetalinguisticsPragmatics
Tactile-kinesthetic Processing Impacts Fine Motor Function– Progresses in a proximal-distal fashion– Affected by: Sense of body position or movementVisual spatialpprocessingpgVerbal-motor integrationMotor planningMotor sequentialqmemoryyMonitoringToneCoordination
Memory Short Term Active working Long Term
Short Term Memory Holds information for a few seconds Limited storage capacity Depends on:– VolumeV l– Modality Visual,Vil AAuditory,ditTTactiletil - KinestheticKith ti– Attention
Working Memory Intermediate durationg an idea in mind while developing,p g Holdingelaborating, clarifying, using it––––Recalling answers while thinking of the questionComplex math problemsReading (summarizing/comparing while decodingS l ti colorSelectingl whilehil rememberingb i whath t you aredrawing
Working Memory Factors affecting it:– Attention– Rate– Volume– Automaticity of skill
Long Term Memory Unlimited storage capacity Long duration Retrieval affected by:– RelevancyR loff stimulusti l– Frequency of use– StrategySt tforf memorizationi ti (consolidation)(lid ti )
Output Oral– Casual– Benefits from tone, gestures, etc. Written– Very formal– Depends on fine motor / graphomotorfunction Motor sequences, pencil grip, spatialorganization
Fine Motor Function Progresses in a proximal-distal fashion Affected by:––––––––Sense of body position or movementVisual spatial processingVerbal motor integrationVerbal-motorMotor planningMotor sequential memoryMonitoringToneCoordination
Behavioral ENIAATTENTION
Medical FactorsCHRONIC HEALTHPROBLEMSASSOCIATED HEALTHPROBLEMSIATROGENIC HEALTHPROBLEMS
Environmental MPERAMENTPHYSICAL FACILITYCURRICULUM DEMANDSTEACHERShouse
Developmental WebManagement
Educational ManagementEducational TherapySpeech & Language TherapyOccupational lumeRateTechnologyComplexity
Psychological ManagementADULT FOCUSEDBehavioral TherapyCHILD FOCUSEDCognitive Therapy
Medical ManagementMEDICATIONSURGERY
Environmental ManagementHOMESCHOOL
DyslexiaEtiology
Phonological Processing
Phonology Phoneme:––––Building block of wordsS ll t unitSmallestit off speechhThere are 40 - 52 phonemes in the English languageAre put together to form words Words can be broken down into their elementalsounds allowing us to decipher words Deficits in phonology strongly correlate withreading problems
Phonologic System Processing and production of speechsounds Earliest language system to develop It is natural – does not have to be taught It is the foundation of language
Phonological Processing gicalMemory
Fluency The ability to read text– Quickly– Accurately– With good understanding The hallmark of a good reader Is the bridgeg between decodingg andcomprehension It is acquiredqword-by-wordy
Dyslexia Etiology Language problem specific to thePhonologic Module– Functional part of the brain where Sounds of language (phonemes) are puttogether to form words Words are broken down into their elementalsounds (phonemes) Discriminates words from noise– Learning to read is not a natural biologicalprocess
Dyslexia: NeurobiologyPhoneme ProcessingSSpeechVisual Word - FluencyTypical ReadersDyslexic Readers
TypicalypReaders:Elision versus RepetitionleftEden et al., 2004right
Dyslexia: NeurobiologyControlEden et al. Nature 1996Dyslexic
Reading: NeurobiologyPhonological processingPhoneme Processingcatkæt
Reading: NeurobiologyVisual - FluencyVisual Word - Fluencycat
Reading Disability(D x F) C ReadingD DecodinggF FluencypC ComprehensionM. Joshi; IDA National Conference November 2004
Reading on Meaning
Early IdentificationWhat to look for
Early Signs of Dyslexia By age of onset:–––––Delay in speakingDifficulty in pronunciationInsensitivity to rhymePoor word retrieval or word findingNaming the letters and their sounds
Early Signs of Dyslexia Infants and toddlers– Delay in speaking First word by 1 yearPhrases by 18 - 24 monthsParents may ascribe it to family history– Speech delay and dyslexia are familial
Early Signs of Dyslexia Preschool years– Difficulty in pronunciation No “baby talk” by 5 or 6 years of ageTypical problems:– What to listen for» Omission of initial sounds: lephant for elephant,chi-en for chicken» Inverting sounds: aminal for animal
Early Signs of Dyslexia Preschool years– Insensitivity to rhyme Unable to recite nursery rhymes– Children that remember nursery rhymes tend to begoodd readersd Unable to differentiate between similar anddifferent words– Can not focus on parts of the words» What rhymes with: food, talk
Early Signs of Dyslexia Poor word retrieval or word finding– Talking around a word (circumlocution)– Uses words like “stuff” or “things”
Early Signs of Dyslexia Naming the letters and their sounds– Before entering Kindergarten Knows the names of upper and lower case letters– Before entering 1st grade Knows the names and sounds of letters Alphabetic principle– Sequence of letters number and sequence of sounds MatchesM t h bbeginningi i soundsd off wordsd Pronounces beginning sounds of words Counts phonemes in small words
Early Signs of Dyslexia Typical development– 4 – 6 y/o aware that words come apart– 6 y/o 70% can count phonemes in small words Early signs of dyslexia– After 1 year of reading instruction (end of 1stgrade) can’tcan t separate sounds of spoken word
Common Signs of Dyslexia Problems with:– Phoneme segmentation– Phoneme deletion– Specific word retrieval (i(i.e.e tornado forvolcano, prostitute for prosecute)– Rapid word retrieval
History Screening: Infancy Single words by 1 yr Phrases by 2 yrs FamilyF il hihistorytoff llanguage orreading problemsY N
History Screening: PreschoolEnd of K – 4 Omission of soundsY N – Eliminates initial sounds(i.e., lephant for elephant) Inverts sounds( i l ffor animal)(aminali l) Insensitivity to rhyme– Can’t memorize nursery rhymes– Can’tC ’t ttellll if wordsd rhymeh Does not know lower case alphabet
History Screening: KindergartenBy the end of year CAN NOT: Name upper and lower casealphabet Name most letter sounds Match beginning sounds to words Pronounce beginning sounds ofwordsYN
History Screening:st1GradeBy the end of year CAN NOT: Can separate and / or countsounds in a word FindFi d ththe righti ht wordsdYN
Screening Test: End ofst1Grade Alphabetic principle– Names beginning letters of words– Names beginning sounds of words– Names ending letters of words– Names ending sounds of words– Can tell # of sounds in a wordPF
Screening Test: K.5 and Rhymingst1GradePF – Say a word that rhymes with Food Walk– Can recite a rhyme
History Screening: Infancy Single words by 1 yr Phrases by 2 yrs FamilyF il hihistorytoff llanguage orreading problemsY N
History Screening: PreschoolEnd of K – 4YN Omission of sounds – EliEliminatesi t initiali iti l soundsd(i.e., -lephant for elephant, chi-en for chicken) Inverts sounds(aminal for animal) Insensitivity to rhyme– Can’t tell if words rhyme Does not know lower case alphabet
History Screening: KindergartenBy the end of year CAN NOT: Name upper and lower casealphabet Name most letter sounds Match beginning sounds to words Pronounce beginning sounds ofwordsYN
History Screening:st1GradeBy the end of year CAN NOT: Can separate and / or countsounds in a word FindFi d ththe righti ht wordsdYN
Screening Test: End ofst1Grade Alphabetic principle– Reads the words accurately– Names beginning letters of words– Names beginning sounds of words– Names ending letters of words– Names ending sounds of words– Can tell # of sounds in a wordPF
Screening Test: K.5 and Rhymingst1GradePF – Say a word that rhymes with Food Walk
InterventionWhat to do about it.
Research Based Reading Instruction Essential Components– Phonemic awareness Recognize,gremember and manipulatepindividual sounds– Phonics and word recognition Sound – symbol relationship, word meaning– Reading Fluency Read with sufficient speed an accuracy to supportcomprehension– Vocabulary development Individual word meanings– Reading comprehension Verbal reasoning, background knowledge, comprehensiongstrategies
Reading Instruction Other components– Basic writing skills Compose English with accuracy, fluency andclarity of expression– Comprehending and using language The ability to listen and understand themeaningi off whath t someone isi sayingi
Effective Reading Instruction Explicit– Clearly and directly explained not left to discovery Systematic– The speech sounds, spelling patterns, sentence structures, textgenre and language conventions Cumulative– ContinualC til reviewione skillkill bbuildsild on anotherth Multisensory Sequential and Incremental– ManageableMbl stepst Data driven– Emphasis, speed of instruction and support are determined bystudent'sstudents progress
Dyslexia: Management Critical to start before 3rd grade It is almost impossible to remediateafter 4th grade
Earlyl Interventioni IS Urgent 10TH %ile 5th Grade reader 50,000 words/year 50TH %ile 5th grade reader 600,000 words/year Average students receiveapproximately 10 TIMES asmuchh practiceti ini a yearAnderson, Wilson & Fielding 1998
ain activationprofile becomesnormal followingsuccessful remedialtrainingSimos, Fletcher, et al. Neurology,2002Post-testing
What About Attention?ADHD:What it is and what is not!
ADHD: Historical TimelineHyperkineticHki ti RReactiontiof Childhood (DSM-II)Attention Deficit HyperactivityDisorder (DSM-III-R)Minimal Brain Damage1902193019601968198019871994Minimal Brain DysfunctionyADHD-like syndromefirst describedAttention Deficit Disorder or Hyperactivity (DSM-III)Attention Deficit/Hyperactivity Disorder (DSM(DSM-IV)
DiagnosticgCriteria for ADHD:DSM-IV Persistent symptoms of inattention and/or impulsivity andhyperactivity Onset of symptoms before age 7 Impairmentpin 2 or more settingsg ((eg,g, school,, work,, home)) Evidence of clinically significant impairment in social,academic,, or occupationalpfunctioningg Symptoms not a result of other disordersDiagnostic and Statistical Manual of Mental Disorders. 4th ed. Text Revision.Washington, DC: American Psychiatric Association; 2000.
DSM-IV DiagnosticgCriteriaSymptoms for ADHD Inattention ( 6)– IIs carelessl– Has difficultysustainingg attentionin activity– Does not listen– Does not followthrough with tasks– Is disorganized–AAvoids/dislikesid /di lik ttaskskrequiring sustainedmental effort– Loses important items– Is easilyy distracted– Is forgetful in dailyactivitiesDiagnostic and Statistical Manual of Mental Disorders. 4th ed. Text Revision.Washington, DC: American Psychiatric Association; 2000.
DSM-IV DiagnosticgCriteriaSymptoms for ADHD (cont’d) Hyperactivity ( 6)–––––Squirms and fidgetsCannot stay seatedRuns/climbs excessivelyCannot play/work quietlyIs on the go/drivenby a motor– Talks excessively Impulsivity— Blurts out answers— Cannot wait turn— Intrudes/interrupts othersDiagnostic and Statistical Manual of Mental Disorders. 4th ed. Text Revision.Washington, DC: American Psychiatric Association; 2000.
ADHD: DSM-IV Subtypes ADHD Combined Type– CriteriaC te a aaree metet foro botboth inattentionatte t o aanddimpulsivity/hyperactivity ( 6 of each) ADHD Inattentive Type– Criteria met for inattention but not forimpulsivity/hyperactivity ( 6) ADHD Hyperactive-Impulsive Type– Criteria met for impulsivity/hyperactivitypy ypy but not forinattention( 6)
ADHD ComorbidADHD:Cbid CConditionsdi stanceusedisorder5Cooperative Group. Arch Gen Psychiatry 1999; 56:1076–1086.R. Attention-deficit Hyperactivity Disorder. A Handbook for Diagnosis and Treatment, 2nd ed. New York: Guilford Press, 1993.3Biederman J, et al. Am J Psychiatry 1991; 148:565–577.4Milberger S, et al. J Am Acad Child Adolesc Psychiatry 1997;36:37–44.5Biederman J, et al. J Am Acad Child Adolesc Psychiatry 1997;36:21–29.2Barkley
ComorbidityCbiditIsI CommonCWith ADHDComorbidityIs Common With ADHDADHDADHDCONDUCT (10%)OppositionalOppositionalppDiDisorderd (40-50%)(40(40-50%)50%)DisorderConduct (10%)ADHD Only AnxietyDisorderDisorder(35%)(35%)
Etiology
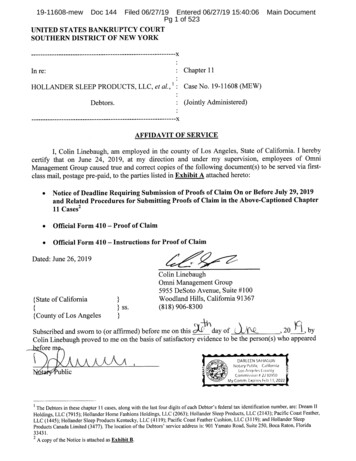
AAVarietyVariety ofof FunctionalFunctional&& StructuralStructuralDifferences Appear in the ADHD BrainADHDNormal Controlsy 21 mm1 x 10-2y 2121 mm1 x 10-31 x 10-21 x 10-3MGH-NMR Center & Harvard- MIT CITP Reprinted by permission of Elsevier Science from Anterior cingulateand the RI and bythepermissionCounting StroopcingulateMGH-NMRcortexCenter& Harvard- inMITCITPrevealed byReprinted, by BushScienceG, Fraziercortex 1999dysfunctionin ADHDbyPsychiatry.fMRIRauchSL, et al., Biological Psychiatry 45(12), Copyrightby theG,SocietyofrevealedBiologicalStroop , by BushFrazierJA, RauchSL, et al.,
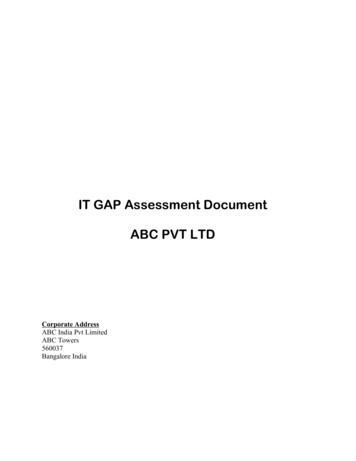
Twin Studies Show ADHDIs a Genetic DisorderBreast cancerHudziak, 2000AsthmaSchizophreniaHeightNadder, 1998Levy,y, 1997Sherman, 1997Silberg, 1996Gjone, 1996Thapar, 1995Schmitz, 1995Edelbrock, 1992Gillis, 1992Goodman, 1989Willerman, 197300.20.40.60.8Average genetic contribution of ADHD based on twin studiesFaraone. J Am Acad Child Adolesc Psychiatry. 2000;39:1455-1457. Hemminki. Mutat Res. 2001;25:11-21.Palmer. Eur Resp J. 2001;17:696-702.ADHDMean1
Impairment Caused by ADHDHow does it present?Impact on quality of life
nM di lMedical
Impairment ADHD is a disorder of performance, notskill ADHD disrupts executive function ADHD creates problems with selfselfregulation ADHD iincreases hhealthlth risksi k
Impairment ACADEMIC– Production vs. Knowledge BEHAVIOR - EMOTIONAL– Spacey/Over-ReactiveSpacey/Over Reactive vsvs. Defiant SOCIALIZATION– InsatiableIti bl vs. MMaliciousli i MEDICAL– Cigarette smoking, Car accidents, SUD
ADHD: Impairment over tionshipsLowself-esteemADHDLegaldifficultiesMotor vehicleaccidentsInjuriesSmoking andsubstance abuse
ADHD: Impact on FamilyParents of children with ADHD experiencehigher levels of: StressSelf blameSelf-blameSocial isolationDepressionMarital discordMash and Johnston. J Clin Child Psychol. 1990;19:313.Murphy and Barkley. Am J Orthopsychiatry. 1996;66:93.
ADHD : AdultsPerformance Limitations Despite similar educational levels and IQscores, non-medicated adults with ADHDdisplay:– Significantly more academic difficulty in school(25% repeat a grade)– Lower levels of occupational advancementFaraone S, et al. Biol Psychiatry. 2000;48:9-20.Biederman, et al. Am J Psychiatry. 1993;150:1792-1798.
ADHD Affects Socialization Children are stigmatized by their behavior– Disruptive behavior TroublemakersBad sportsmanshipExcessive talkingCannot sit stillU fUnfocused,d nott responsivei tto othersthImpulsive aggression–Immaturity and impulsiveness CenterCenter of attention Breaks the rules Blurting out answers Peer rejection Adolescents continue to demonstrate socialproblems Poor participation in group activities Few friends Vulnerable to antisocial groups, drug abuseAACAP. J Am Acad Child Adolesc Psychiatry. 1997;36:85S-121S.Barkley RA. J Am Acad Child Adolesc Psychiatry. 1991;30:752-761.
Increased Traffic Violations and Motor VehicleA idAccidentsini AdolescentsAd landd AdultsAd l withihADHD9080P 0.004subjeects (%)70Control n 23ADHD n 25P 0.07P 0.0760P Barkley RA, et al. Pediatrics. accidentssuspended
Increased Smoking with ADHD50%Adult patients with ADHD48.5%Cuurrent smmokers40 8%40.8%40%29%30%25.8%20%*SmokersPomerleau, et al. J Subst Abuse. 1995;7:373-378.Quit ration 71GenerallGpopulation*P 0.0110%0%ADHD
Earlier Initiation ofSmoking with ADHDSmokingg probabillity0.60.5ADHD n 128C t l n 109Control1090.46- to 17-year-old boys0.30.2010.100246810P 0.003Milberger S, et al. J Am Acad Child Adolesc Psychol. 1997;36:37-44.12Age141618202224
P 0.001P 0.001Biederman J, et al. Biol Psychiatry. 1998;44:269-273.Biederman J, et al. Pediatrics. 1999;104:e20-e25.Prevalennce of subsstance abuuse (%)Lifetime hhistory of ssubstance use (%)Untreated ADHD Is Associated WithHigher Risk of Substance AbuseP 0.001P 0.001
Adolescent & Adult Outcome Symptoms Persist in 50-65% Associated Problems– Conduct– Emotional– Socialization– Education– Employment Satisfactory Outcome in 6060-70%70%
Management of ADHD
Good Managementgof ADHDInvolvesMultimodalTherapyMultimodal TherapyMedicationPsychosocial TherapyStimulantsParent TrainingAntidepressantsChild-Focused TreatmentSNRI’sAlternativesSchool-Based InterventionNormalizationin ManyAreasNormalizationin ManyAreas
MTA StudyStStudyd ObjectiveObjObjectiveti andanddDesignDesignD iObjective: To compare the long-term efficacy of pharmacotherapy, behavioraltherapy, and combination therapy in the treatment of ADHDProtocol: Population: 579 children with ADHD combined type, aged 7-9.9 years In a 4-group parallel design, children randomly assigned to:– Medication alone (primarily methylphenidate)– Behavioral therapy alone– Combination of medication and behavioral treatment– Routine community care (medication and behavioral treatment) Duration of study treatment: 14 monthsThe MTA Cooperative Group. Arch Gen Psychiatry. 1999;56:1073-1086.
MTA Study:y Treatment Outcome:Teacher-Rated nattention(MTAGroup,1999)2.52 Community Control 1.5Behavior ModificationMedical Management1Combination TherapyComb,Med Mgt Beh, essmentPoint(Days)400400The MTA Cooperative Group. Arch Gen Psychiatry. 1999;56:1073-1086.
Improvvement at 114 months ((%)Long term Outcomes of Therapies forLong-termADHD in the MTA Study7065605550454035302520151050Hyperactive Impulsive Symptoms(Teacher ybasedtreatment
The Developmental WebDevelopmental ProfileBehavioral ProfileHealthEnvironmentEducational &DevelopmentalAcademic – OccupationalBehavioral – EmotionalSocial InteractionHealthBehavioral &CognitiveMedicalEnvironmental
American Academy of Pediatrics:G id liGuidelinesforf theth TTreatmenttt off ADHD Establish a treatment program that recognizes ADHD as achronic conditionSpecify appropriate target outcomes to guide managementPrescribe stimulant medication and/or behavior therapy toimprove target outcomes in children with ADHDIf the treatment program has not met target outcomes,evaluate:–––– Original diagnosisUse of all appropriate treatmentsAdherence to the treatment planPresence of coexisting conditionsUsing information from parents, teachers, and the child,follow-up to evaluate target outcomes and adverse effectsAAP. Pediatrics. 2001;108:1033-1044.
Types of Medications Used InManaging henidateAmphetaminesAtomoxetineImmediate ReleasePulseOROSTransdermaldextroamphetamineMixed AmphetamineslisdexamfetamineImmediate ReleasePulseImmediate ReleasePulseImmediate ReleasePulse
DopamineNorepinephrineR t k pumpsReuptakeMedicationReceptors
DopamineNorepinephrineR t k pumpsReuptakeMedicationReceptors
Proposed Effect of StimulantsIncrease Dopamine creases Dopamine Reuptake
Medications: Clinical Impact Increase control of attentionIncrease impulse controlDecrease activityDDecreasedidisruptiveti bbehaviorh iImprove handwriting (in 50%)
Medications: Clinical Impact Academic Increase Production Behavior Increase ComplianceDecrease Disruption Socialization Increase Awareness
Stimulant Medications Side Effects– Insomnia (50-60%)– Anorexia (50-60%)– Irritability (30%)– Headache– Stomachache– Nausea– Tics
Atomoxetine: Side Effects AnorexiaDizziness - SleepinessDyspepsiaDDermatitistitiConstipationMood SwingsTransient elevation of liver enzymesIncreased suicidality
Medications: Duration of Action Short Acting: Intermediate Acting: Long Acting:4 hours6 – 8 hours8 – 12 hours24 hhours
Medications Short-Acting Ritalin, Dexedrine, DextroStat,Focalin Methylin (Tablet,Chewable & Liquid) Intermediate-Acting Ritalin SR, Metadate ER,Adderall, Ritalin LA, MetadateCD Methylin ERCD,ER, Focalin XR Long-Acting Dexedrine Spansules, Cylert,Adderall-XR ConcertaAdderall-XR,Concerta,Daytrana, Vyvanse 24 hours Strattera
MPH OROS (Concerta )20IR MPH 10 mg tid (n 15)CONCERTA 36 mg qd (n 15)Concenttration(ng/mmL)161284002468Time (h)MedicineMedicinePushCompartment CompartmentCompartmentOuter Coatof Medicine#2#11012
MPH SODAS (Ritalin LA)Pulse ReleaseSODAS is a trademark of Elan Corporation, Plc
Pulse Delivery System ime (h)10121416
Mixed Amphetamine Salts(Adderall XR )Formulation StudyBioequivalence of Adderall XR 20 mg QD to Adderall 10 mg BIDMean DD- and L-ammphetaminnePlassma Conceentration(ng/mLL)30Adderall 10 mg BIDAdderall XR 20 mg 6202428Time (h)Tulloch et al. Pharmacotherapy 2002;22:1405.323640444852
MatrixDaytranayDOTOTransdermal Technology Methylphenidate is mixed with adhesiveDOT Matrix is a trademark of Noven Pharmaceuticals, Inc.
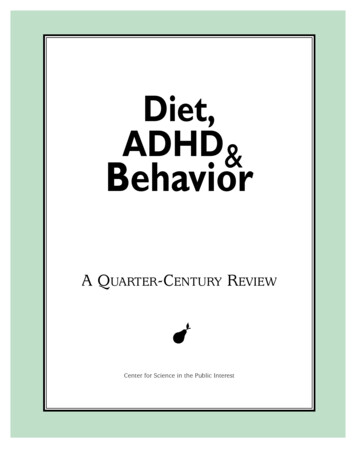
Pharmacokinetics with DaytranaMean Plasma ConcentrationCoff d-methylphenidate10 mg Daytrana20 mg Daytrana30 mg Daytrana5040Mean Plasmad-MPHdMPH Conc(ng/mL)3020100012345678Time post-dose (hr)Patchapplied910PatchremoveddLower limit of quantification 0.25 ng/mL.Pierce et al. Poster presented at the AACAP Annual Meeting. Toronto. October 20, 2005.1112
Application and Removal/Disposal Holding the patch down, therest of the liner should beremoved slowly and theexposed half should bepressed against the skin TheTh patchh shouldh ld bbe pressedddown with the palm of the handfor 30 seconds Upon removal, the patchshould be folded in half, withg, andstickyy sides together,discarded immediately in toiletor lidded container
Vyvanse Is a pro-drug– Inactive until the body breaks it down Combines an amphetamine and anamino acid– Dextroamphetamine and lysine It lasts12 hrs Not affected by GI transit time or pH
Atomoxetineo o e eEfficacy (Strattera(Se )
Behavioral ManagementWhat to do at Home
Core Principlesp for BehaviorManagement Immediacy of ConsequencesFrequency of ConsequencesSaliency of ConsequencesFrequent Changes in RewardsA t Don’tAct,D ’t YackY kPositives Before NegativesAnticipate ProblemsPick Your Fights - PrioritizepVariabilityyExpectPractice Forgiveness
It is not your faultfault But it is your problem
ADHD: Historical Timeline Hyperkinetic Reaction of Childhood (DSM-II) Attention Deficit Hyperactivity Minimal Brain Damage Disorder (DSM-III-R) 1902 1930 1960 1968 1980 1987 1994 Minimal Brain Dysfunction Attention Deficit Disorder or - Hyperactivity (DSM