Transcription
Medicinal Chemistry
all material is available online as pdf filesunder the following URL:!http://www.chem.uzh.ch/zerbe/MedChem/Course MedChem.html
The Medicinal Chemistry Course ADME (adsorption, distribution, metabolism and excretion) of drugsdrug-receptor interactionsdevelopment of drugs screening techniquescombinatorial chemistry (D.O.)classical medicinal chemistry, hit-to-lead developmentfragment-based drug designrational drug design / de-novo drug designnatural productscase studies of drug synthesis (D.O.)the common targets for drugs (receptors)biophysical methods for determination of structure and binding interactionsantibacterial drugsantiviral drugsanti-cancer drugsanti-inflammatory drugspatent issues (P.F.)
Books and other information sourcesMonographs: G. Patrick: Introduction to Medicinal Chemistry, Oxford University Press, 2005(very good introduction) H.-J. Böhm, G. Klebe, H. Kubinyi: Wirkstoffdesign. Der Weg zum Arzneimittel(Spektrum Lehrbuch) (very interesting, easy to read) G. Thomas: Medicinal Chemistry: An Introduction (Wiley), (inexpensive introduction) H. P. Rang, M. M. Dale, J. M. Ritter: Pharmacology, Churchill Livingstone; 6th ed. E.J. Corey, B. Czakó, L. Kürti, Molecules and Medicine (Wiley) D.S. Johnson, J.J. Li: The Art of Drug Synthesis (Wiley)!Journals: Nature Reviews Drug Discovery Drug Discovery Today ACS Journal of Medicinal Chemistry Trends in Pharmacological Sciences
Society before 18001 childbed feverof the mother2 infection of appendix3 accidents3quality oflife21age
Medicine ca. 19501 childbed feverof the motherasepsis2 infection of the appendix3 accident tetanusvaccination3quality oflife21ageanesthesia,antibiotics
Medicine after 1950quality oflifeage
most common cause of death for 22-44 year old people8
65 years and older.MaleFemaleCardiac Infarction2,9%Pneumonia2,8%Pancreatic Cancer3,0%3,7%StrokeStroke3,5%3,8%Prostate CancerCardiac Infarction4,3%4,7%obstructive lung disease(smokers lung)Cardiac insufficiency6,1%6,9%Cardiac insufficiencyColon Cancer8,3%7,7%Lung 2,4%1,7%2008hypertension-relatedheart conditionBreast cancerPneumonia2,3%Cardiac arrhythmia2,1%Lung Cancer2,1%obstructive lung disease(smokers lung)
Medicine in the antiquity Chinese medicine: (3500 BC)– chinese herbs, some of the ingredients are still in use today, e.g.Reserpin (blood high pressure; emotional and mental control), Ephedrine(Asthma) Egyptian medicine (3000 BC)– Papyrus Ebers, 877 descriptions and recipes Greek medicine (from 700 BC)– illness is no punishment from God, medicine is considered a science– diseases are due to natural causes– Hippocratic oath Roman medicine (from approx. 200 BC):– invention of hospitals– large influence of greek medicine– Materia Medica: pharmaceutical descriptions
Medicine in the Middle Ages (400 to 1500 AC) The church preserves greek traditional recipes Era of horrible epidemics (e.g. Pest, Lepra, Pox, Tuberculosis) Arabic medicine: Development of medical procedures for drug preparation(distillation)afterwards. Development of scientific approaches: Pox: Edward Jenner discovered that people who worked withcattle and had caught the cowpox disease (a mild diseaserelated to smallpox) were immune and never caught smallpox. Heinoculated a boy with blister fluid from a woman with cowpox.He later inoculated the same boy with fluid from smallpox, anddiscovered that the boy was immune against the disease. Bill Withering introduces extracts of Digitalis for treatment ofheart problems Louis Pasteur discovers that microorganisms are responsiblefor diseases and develops vaccinations against rabies. Heintroduces attenuated viruses for treatment of rabies.
until 1900 Digitalis (isolated from the plant digitalis, stimulation ofthe heart muscle) Chinin (alkaloid from peruvian bark, treatment of malaria,fever lowering) Ipecacuanha (from the bark of ipecac, treatment ofdiarrhea) Aspirin (from the meadow bark, against fever and pain) Mercury (- syphilis)12
Discovery of Penicillin Alexander Flemming discovers in 1928 that a fungus grew on abacterial plate containing staphylococci. Close to the fungus allbacteria were killed. Biotechnological production of penicillins was establishedduring the second world war and helped saving the life of manysoldiers13
Robert Koch!Nobel laureate 1905"for his discovery and treatment oftuberculosis"
osaBacteria under the electron microscopeEscherichia ColiCholeraStapphylococcus AureusPseudomonas Aeruginosa
Since then. Early 1900: synthetic drugs, foundation of pharmaceuticalindustry since 1930: screening of natural products, isolation of theirbioactive ingredients late 70 ies: Development of recombinant drugs (proteins, e.g.interferons). Development of biotechnology 2000: Deciphering of the human genom, gene therapy (?),Investigation of the molecular basis of disease future: Personalized medicine?
ComplexityHistory of drug developmentfocus onmolecular functionaccidentialobservationfocus oncell-biologyfocus onbiochemistrytaken from: Real World Drug Discovery, R. Rydzewski, Elsevier 2008
Blockbuster (2004)Best-selling pharmaceutical products 2002–2004ProductCompanyTrade (Generic) nameSales figures for 2002(US billion)CompanyIMSSales figures for 2003(US billion)CompanySales figures for 2004(US billion)IMSCompanyIMSLipitor (Atorvastatin)Pfizercholesterol-lowering8.60 medication9.23 7.9010.310.8612.00Zocor (Simvastatin)Merck5.60agent lipid-lowering6.205.016.105.205.90Plavix (Clopidrogrel)anti-platelet medicationBMS and Sanofi-Aventis 3.10NA4.203.705.205.00Advair (Fluticasone; Salmetrol)GSK2.00NA anti-asthma medication3.60NA4.504.70Norvasc (Amlodipine)Pfizeragent3.804.004.33 blood pressure-lowering4.504.464.80Zyprexa (Olanzapine)Eli-Lilly3.604.00 anti-depressant4.274.804.424.80Paxil (Paroxetine)GSK1.90NA anti-depressant3.003.903.903.90Nexium (Esomaprazole)AstraZeneca1.973.30produced in the3.80stomach 3.88 decreases theNAamount of acid4.80Zoloft (Sertraline)Pfizer2.74NA anti-depressant3.103.403.36NACelebrex (Celecoxib)Pfizer3.00NA drug anti-inflammatory1.902.503.30NAEffexor (Venlafaxine)Wyeth2.00NA anti-depressant2.70NA3.303.70Prevacid (Lansoprazole)Takeda and Abbott3.103.80Diovan (Valsartan)Novartis3.10NAFosamax (Alendronate)Merck3.10NARisperdal (Risperidone)J&J3.30produced in the4.00stomachdecreases the3.60amount of acid 3.701.66NA2.50NA prevents vasoconstrictionNA agent 2.50NAanti-osteoporosis 2.202.10NAmedication 2.50 antipsychoticNA3.00NAGlobal pharma market IMS US 550 billion; global biotechnology market valued at US 55 billion; global generic market US 62 billion.Table lists top 15 Medicines in 2004 with sales of over US 3 billion.Abbreviations: BMS, Bristol-Myers Squibb; GSK, GlaxoSmithKline; J&J, Johnson and Johnson; NA, not available.
Blockbusters 2013 (C&N news, supl. 09/14)namedisease areacompanydrug classsales 20131Humira (adalimumab)RheumatoidarthritisAbbVieantibody 11 billion2Enbrel ion protein 8.75 billion3Advair (fluticasonepropionate and salmeterol)GSKsmall molecule 8.3 billion4Remicade (infliximab)Asthma, chronicobstructivepulmonary diseaseRheumatoidarthritisJohnson &Johnson/Janssenantibody 8.3 billion5Rituxan (rituximab)Roche/Genentechantibody 8 billion6Lantus (insulin glargine)Lymphoma,leukemia andrheumatoidDiabetesSanofiinsulin analogue 7.5 billion7Avastin (bevacizumab)CancerRocheantibody 6.5 billion8Herceptin (trastuzumab)CancerRoche/Genentechantibody 6.5 billion9Crestor (rosuvastatin)high cholesterolAstraZenecasmall molecule 6 billion10Januvia (sitagliptin)diabetesMercksmall molecule 6 billion
Top small molecule drugsOHHOO(CH 2 ) 6H 3C(CH 2 ) 4SalmeterolH 3CHOSNNHOOONHCH 3NCH 3HO 2 CFNClRosuvastatinOH 3CCH 3CNNNHNHNNFHBudesonideAripiprazoleNH 2 OOHSitagliptinCH 3CH 3 ONNFOHNHNImatinib mesylateHCH 3OFNCH 2OONClOH(CH 2 ) 4OHH 3CHNOHOHOOHNNHOHCFormoterolCF 3CH 3 NHSOOSF 3CNNH 2ONCH 3HO 2 CCH 2NNH 2DuloxetineNNNNONNNTelmisartanCelecoxibONH 2CH 3H 3CNH 2CO 2 HPregabalinTenofovirCH 3CH 3PO 3 H 2CH 3HNOOHNNOLenalidomideNSHOSCH 3 OOBr -O N CH 3CH 3OTiotropium bromideCH 3NSOCH 3CH 3NNN NHOEsomeprazoleNHO 2 CCH 3CH 3Valsartan
predicted blockbusters (sales started/start soon)DrugCompanyRevenue (Billion )OpdivoBristol-MyersSquibb 5.684melanoma (antibody)2PraluentRegeneron/Sanofi Sanofi 4.414cholesterol lowerer (antibody)3LCZ-696Novartis 3.731angiotensin receptor-neprilysininhibitor (small molecule)4IbrancePfizer 2.756breast cancer (small molecule)5IumacaftorVertex 2.737cystis fibrosis (small molecule)6Viekira PakAbbieVie 2.500antiviral cocktail (small molecule)7EvolocumabAmgen/Astellas 1.862cholesterol lowerer (antibody)8Gardasil 9Merck & Co. 1.637cancer vaccine for young women9BrexpiprazoleOstuka/Lundbeck 1.353schizonphrenia/depression (smallmolecule)10ToujeoSanofi 1.265long-lasting insulin (protein)11CosentyxNovartis 1.082anti-inflammatory drugs-watch-2015-1857100
Properties of typical drugs small, organic molecules (Lipinski’s Rule of Five):molecularweight 500, not too polar, not too manyfunctional groups that can serve as H-bond donors oracceptors or: natural products chemical synthesis should be not too complicated (price!) no reactive groups in the molecule
Typical drugsOOHNHClOHNFHNCOOHNNCiprofloxacinHO HOHHNNOHNGefitinibNH2H navirNHO OSImipenemLamivudineOFOONONOHCH3NHNNOSO 3N
Blockbusters are often similar.HOOChiralNHOOODDT Vol. 7, No. 10 May 2002ClN NNONNHHNOSMeLovastatinONNLosartanO razoleOSimvastatinValsartanDrug Discovery TodayFigure 8. Structural similarity in blockbusters. Examples of structural similarities betweencompounds within a given class: 3-hydroxy-3-methylglutaryl CoA (HMGCoA) reductaseinhibitors (lovastatin and simvastatin), angiotensin II antagonists (losartan and valsartan),and proton-pump inhibitors (omeprazole and lansoprazole).
Recombinant DrugsSUPPLEMENTARY INFORMATIONIn format provided by Goodman (NOVEMBER 2009)Table S2 Top five products by consensus revenue in 2013EProductCompany2013E consensusrevenue (billions)2012E–2013E% changeAvastinRoche 8.906%Advair DiskusGlaxoSmithKline 8.58-10%HumiraAbbott 7.982%Mabthera/RituxanRoche 7.563%LantusSanofi-Aventis 6.847%
Portfolio share of biologics
Derivates of Natural Products
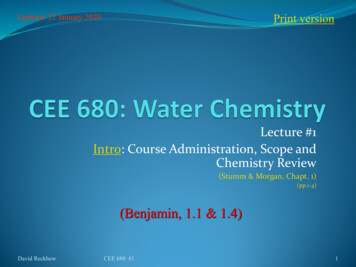
Gleevec: Target Identification Identification of an oncogene (a gene that results in increasestumorgenic activity):– chronic myelogenous Leukaemia is characterized by excessiveproliferation of certain cells– CML results from gene translocation between chromosomes 9and 22– as a result a BCR-ABL gene is created, that encoded for theBCR-ABL kinase– The sole expression of the BCR-ABL gene is identified as thesole oncogenic event resulting in induction of Leukaemia in mice.Capdeville, Nat.Rev.Drug.Discov. 1 (2002),493
Gleevec: Medicinal Chemistry Lead compound identified from screen for inhibitors ofthe protein kinase C (PCK). Strong binding is retained whenthe pyridyl unit is added. Presence of an amide group on the phenyl ring providedinhibitory activity against tyrosine kinases such as BCR-ABLkinase (target hopping) Substitution at position 6 of the diaminophenyl ringabolished PCK inhibitory activity while retaining it attyrosine kinases (increasing selectivity) Improvement of ADME properties. Addition of a polarside-chain markedly increases both solubility and oralbioavailability. To avoid the mutagenic potential of anilinecompounds a CH2 spacer was inserted.Capdeville, Nat.Rev.Drug.Discov. 1 (2002),493
Gleevec binds to the inactive conformation ofBCR-ABL the structures of active kinases aresimilar. Hence it is difficult to find aselective inhibitor for kinases Gleevec binds to the inactive form,which is structurally different in thevarious kinases, and thereby achievesgood selectivity
Gleevec: Pharmacological Profiling In-vitro studies– The selective inhibitory activity of Gleevec was demonstratedon a cellular level on the constitutively active p210(BCR-ABL)kinase.– Inhibition of autophosphorylation of BCR-ABL by Gleevec In-vivo studies– treatment of BCR-ABL transformed cell-lines with Gleevecresults in dose-dependent reduction of tumor growth– the anti-tumor effect is specific for BCR-ABL expressing cells– Gleevec re-activates apoptosis in BCR-ABL cells by suppressingthe capacity of STAT5 to activate the expression of the antiapototic protein BCL-XL.– Gleevec restores normal cell-cycle progressionCapdeville, Nat.Rev.Drug.Discov. 1 (2002),493
Gleevec: Clinical DevelopmentChronic phaseAdvanced phasesAccelerated phaseMedian 4–6 years stabilizationMedian duration upto 1 yearBlastic phase (blast crisis)Median survival3–6 months Demonstration of dose-response relationship in patients withchronic phase CML. mathematical modelling of data confirmed the useful therapeuticdose to be around 400mg a large multinational study with close to 1000 patients from allthree phases of the disease revealed that treatment was mostefficient when started in an early phase of disease progression approval by FDA in 2001 efficiency of Gleevec can be improved by co-administration ofinhibitors of P-glycoprotein studies of factors leading to Gleevec resistanceCapdeville, Nat.Rev.Drug.Discov. 1 (2002),493
Time-Frame for DevelopmentCapdeville, Nat.Rev.Drug.Discov. 1 (2002),493
Fighting resistances arising from Gleevec resistances occur upon selective pressure for forming mutationsthat do not bind any more to Gleevec a non-competitive inhibitor may suppress formation of drugresistant BCR-ABL mutants because resistant strains need todevelop mutations in two unrelated regions of the proteinsimultaneously a allosteric inhibitor was developed that binds to the myristatebinding site of the BCR-ABL kinase (GNF-2/GNF-5) combination therapy with Gleevec and GNF-2 seems to completelysuppress formation of resistant forms of BCR-ABL kinaseZhang et al., Nature 2010 (463), 501.
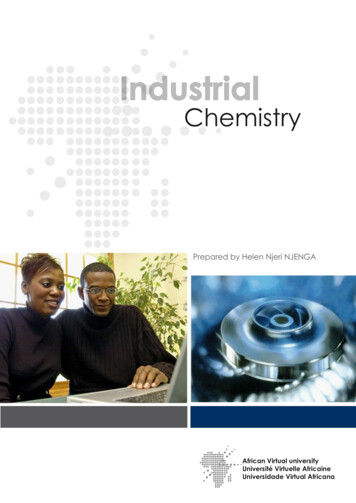
Development of allosteric inhibitors of BCR-ABL122.0122.0123.0123.0124.0124.0125.08.07.0 p.p.m.125.08.07.0 p.p.m.ATP binding!sitemyristyl binding!siteZhang et al., Nature 2010 (463), 501.
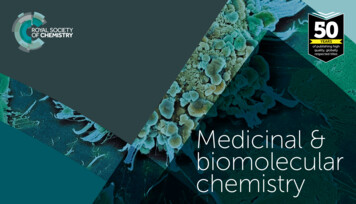
combinations are more resistanttowards resistanceMutations indicated by red spheres on Ablwith size proportional to the degree of resistance84759191968172Resistant colonies025P112S T315lH 2N01002044Day 1202002Day 910GNF-225952566Catalytic site9670Kinase domainSH3 domainS229P1005096Day 21Y128D42125 105ImatinibGNF-2 1 µM imatinibConcentration (µM)SH2 tCOOHEffect of various concentrations of GNF-2, imatinib, or combinationsof both on the number of emerging Ba/F3.Bcr–Abl-resistant clonesZhang et al., Nature 2010 (463), 501.
The Medicinal Chemistry Course ADME (adsorption, distribution, metabolism and excretion) of drugs drug-receptor interactions development of drugs screening techniques combinatorial chemistry (D.O.) classical medicinal chemistry, hit-to-lead development fragment-based drug design rational drug design / de-novo drug design natural products