Transcription
Clinical ScienceKahngZirconium Abutments for ImprovedEsthetics in Anterior RestorationsbyLuke S. Kahng, C.D.T.Mr. Kahng is the founder and owner ofCapital Dental Technology Laboratory,Inc., in Naperville, Illinois. The laboratory specializes in all fixed restorationsand its LSK 121 division provides personalized custom cosmetic work. Mr.Kahng stresses education, communication, and a team approach to patientcare. A member of the AACD, his training has included extensive study withRussell DeVreugd, C.D.T., Dr. FrankSpear, Dr. Peter Dawson, and others.Mr. Kahng is the official clinician forGC America, Bisco, and Captek. He isa frequent lecturer and program facilitator for dentists and dental technicians,and has published articles in PracticalProcedures and Aesthetic Dentistry andDental Dialogue. He can be contactedat luke@lsk121.com.Several esthetically pleasing materials are available for restoring anteriorteeth. All-ceramic or metal-free restorations are considered to be high in esthetics. In planning a course of treatment when there are missing teeth, a single-tooth implant is often preferred because it leaves the adjacent teeth intact.In the all-ceramic category, zirconium implant abutments provide a highly desirable option. The zirconium abutment becomes a particularly esthetic choicewhen there is a gum line location to consider. When a zirconium abutment isused, the problem of matching the shade of adjacent teeth while hiding thedark color of the metal abutment is avoided.The following case history of an oral surgeon undergoing an anterior restoration also illustrates that, although many patients from different professionsmight not be as sensitive to the esthetics involved, future patients will have anincreasing role in planning and determining the requirements for their restorations. Patients are becoming more educated about the advances in dentistrytoday and they see esthetic opportunities that never existed to them before.The zirconium abutment becomes a particularly esthetic choice when thereis a gum line location to consider.Case HistoryIn the summer of 2003 the patient suffered a traumatic accident, whichresulted in a palatal displacement of tooth #8. He immediately repositionedthe tooth in its socket, but there was a slight incisal discrepancy. He soughttreatment within 30 minutes of the accident.90 The Journal of Cosmetic Dentistry Winter 2007Volume 22 Number 4
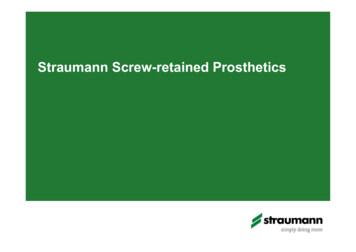
Clinical ScienceKahngFigure 1: View of preparations—#8 is an implant and#9 a preparation for all-ceramic restoration.Findings, Diagnosis, andInitial TreatmentTooth #8 was found to be 1 mmlonger than tooth #9, there wasslight bleeding at the gingival margin of tooth #8, but all other hardand soft tissues surrounding thearea were within normal limits anddid not show any signs of trauma.1A periapical radiograph revealed afracture of the apical 3 mm of tooth#8. The tooth was then splinted tothe adjacent teeth with orthodonticwire and composite.The repairs were left in place forone month, during which time thepatient did not improve. The toothshowed substantial sensitivity tocontact and to temperature. A rootcanal was then performed, but thetooth continued to show sensitivityto any form of pressure, especially atthe apex.In the fall of 2003, tooth #8 wasextracted and extra bone was placedin the socket. A treatment plan waxup was fabricated in the laboratory,along with a surgical stent and a bullet/cone-shaped flipper. The patientwore the flipper for approximatelyVolume 22 Number 4Figure 2: Incisal view showing a 4.3-mm wide, 13mm long tapered implant. Note the position of thelaterals; to follow contour is a challengeto match symmetrically.one year in order to preserve the papillae. During that period, a gingivalcleft formed in the palatal tissue. InOctober 2004, a 4.3-mm wide, 13mm long tapered implant (Steri-OssReplace Select, Nobel Biocare; YorbaLinda, CA) was placed.As the patient is a dental professional, his appearance and dentalesthetics are extremely important.Both arches were bleached in orderto achieve optimal color. It was decided in April 2005 to use a zirconium abutment. Tooth #9 was prepared for a zirconium restoration.The impressions were taken of theimplant and also of the preparationof tooth #9 using a pick-up impression.As the patient is a dentalprofessional, his appearance anddental esthetics are extremelyimportant.FabricationA tissue cast was fabricated fromthe final impression. The zirconiumabutment was generated by a computer-aided design/computer aidedmanufacturing (CAD/CAM) process.2 The combination of zirconiumoxide and CAD/CAM gives strengthand esthetics. A full treatment planwax-up was completed in order tocheck the proper contour and roomavailable, and an index was madeof the full wax-up from laboratoryputty to assist in fabricating the zirconium abutment and substructurefor the restoration.After removal of the provisionalrestoration and temporary abutment, the final abutment was secured. Once the fit was assessed radiographically, the abutment screwwas torqued to 35Ncm. The screwaccess holes were obturated with alight-cured temporary restorativematerial.The zirconium crowns (Procera) were then tried in. The gingival of the crown on tooth #8 onthe implant abutment was tight atthe tissue, so it was adjusted with adiamond abrasive. The crowns werethen cemented using resin-modifiedglass ionomer cement; and, afterWinter 2007 The Journal of Cosmetic Dentistry 91
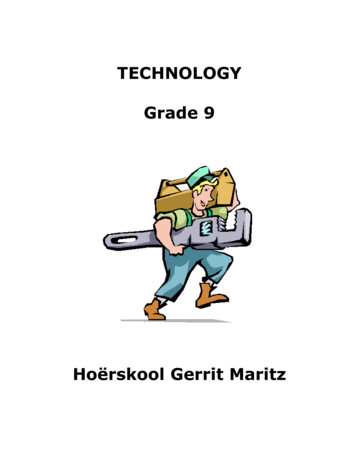
Clinical ScienceKahngFigure 3: Master model with milled zirconiumabutment, still in its machining sleeve.Figure 4: Zirconia abutment is tried in and preparedfor restoration.Figure 5: Full contour wax-up on master modelto check contour and room available for finalrestoration.Figure 6: Zirconia copings are checked with puttymatrix made from wax-up. The labial separationbetween the teeth and width of the proposed crownsare assessed.taking care to see that all of the excess cement was removed, the occlusion was checked to see whether anyadjustments were needed.Treatment DescriptionAs seen in Figures 1 and 2, onecan design an abutment angle upto a 30 angle, the taper, finish line,height, width and cross sectionalform, creating the natural form andemergence profile of the tooth.3 Itis quick and easy to create an abutment using CAD/CAM; or, if oneprefers, to do so using a conventional wax-up that is scanned. The abut-ment can be made in either zirconiaor titanium.As shown in Figure 3, the shapeof the abutment comes already complete from the manufacturer, but thetechnician removes the machiningsleeve and does any minor contouring needed. Then, the abutment canbe tried and checked in the patient’smouth (Fig 4). A full wax-up (Fig 5)was completed to check the propercontour and room available. Thewax-up is a valuable tool to checkfor room available for the copingand porcelain application. An index fabricated from laboratory puttywas made of the full wax-up to aid92 The Journal of Cosmetic Dentistry Winter 2007in the fabrication of the restorations. An abutment and coping canbe evaluated with the matrix (Fig 6).The matrix is used to evaluate boththe labial separation between theteeth and the width of the proposedcrowns.The key to achieve symmetry of therestorations is the width.The technician, working with thedentist, completes the shade mapping by doing a detailed multilayered porcelain shade mapping (Fig7). Not all teeth in a patient’s mouthVolume 22 Number 4
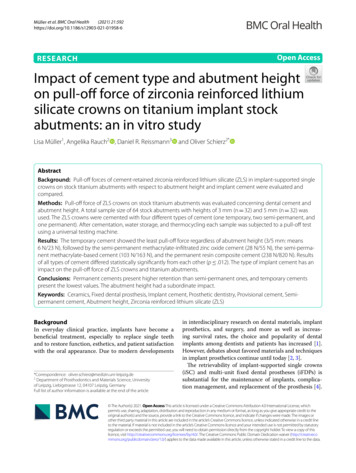
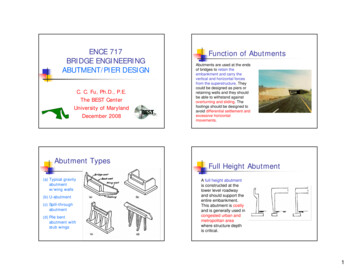
Clinical ScienceKahngFigure 7: Shade map completed by the technician.Figure 8: Samples made by the author illustratethe color variation between incisors to canine topremolars and to molars and should be takeninto consideration.Figure 9: Laboratory porcelain sample test for theopal, enamel and transparency. The color is slightlydifferent from the factory-made shade tab, because ofvariations in laboratory oven temperature.Figure 10: Ultra-violet light sample test checking thefluorescence in the porcelain.are the same natural color; usuallythe canines tend to be darker thanthe others. The incisors are typicallythe whitest, and the molars tend tobe a shade between. The goal is toachieve optimum color matching ofthe adjacent teeth (Fig 8).nician in mimicking shadow zoneswhere a restoration will lose bothchroma and brilliance. As shownin Figure 10, it is important to havefluorescence in the porcelain, the ultra-violet light shows the degree offluorescence.The technician also utilizes porcelain system color-matching tabs.The technician’s fabricated samplesare shown in Figure 9, the laboratory porcelain sample test for theOpal Blue, Enamel 1, and Transparent Clear (Nobel Biocare) to checkthe manufacture color wheel andthe oven temperature from the laboratory. These samples help the tech-Figure 11 shows that the zirconium is white. The internal colorsgive the chroma shade so that therestoration matches a patient’s natural teeth. Note that the molar distallingual cusp has no porcelain on it,showing the white zirconium coping understructure. However, whilethis coping is basically white, a technician can change the foundationVolume 22 Number 4(Fig 12) by using base liner. Thebase liner is used as a wash-bakeon the zirconium frame to start thebase shade. The first application ofporcelain is to get optimal chromausing a dentin shade. Using thedentin and base liner, this will startto make the base chroma shade ofthe restoration. The incisal thirdis modified with dentin and OpalEnamel 2 powder mixed at a 1:1 ratio. Then technician applies a whitestain at the gingival of the tooth foreffect (Fig 13). The first temperaturefiring is important, firing at 900 Cto make sure the porcelain has ma-Winter 2007 The Journal of Cosmetic Dentistry 93
Clinical ScienceKahngFigure 11: The zirconium coping is white; internalcolors give the chroma shade and the finishedrestoration matches natural tooth. The molar distallingual cusp has no porcelain on it, showing thewhite zirconium coping.Figure 12: Base liner is a foundation used as a washbake on the zirconium frame to change the whitecolor of zirconium coping and start the base shade.Figure 13: Porcelain powder application and additionof fluorescent transparent white stain internally atgingival, unlike the opaque white stain at the incisal.Figure 14: First bake of crowns (will check the properfiring temperature).tured at the correct temperature toachieve proper colors (Fig 14).In addition, a thin layer of Transparent Clear powder and Enamel isapplied to the restoration. The Transparent Clear is applied in a thin layerbetween the dentin and the enamel.It brings out true-to-nature depth tothe color of the tooth. The porcelainpowders are applied to the lingualto mimic color and contour, andthe buildup is completed. Thereafter the crowns are fired and checkedfor proper temperature after comingout of the furnace.The key to achieve symmetry ofthe restorations is the width.4 Wecan increase and decrease the widthusing either horizontal or verticalstriated lines giving an illusion ofblending in with the natural teeth(Fig 15).sal margin starting from the middlethird of the tooth, or accentuation ofthe vertical ridges and lines are somethings that will give the illusion ofdecreasing the width.5The movement of the buccaltransition line angles toward the interproximal areas, flattening of thebuccal face, or accentuation of thehorizontal ridges and lines are somethings that will give the illusion ofincreasing the width.To give the illusion of reducedlength accentuated breakdown ofthe three planes of the buccal facein the apico-coronal direction, clearconvexity of the cervical third, clearlingualization of the incisal third, oraccentuation of the horizontal ridges and lines are done.4The movement of the buccal transition line angles toward the centerof the tooth, increasing convexityof the buccal face in the mesiodistaldirection, rounding the disto-inci-94 The Journal of Cosmetic Dentistry Winter 2007To give the illusion of increasedlength minimal breakdown in thethree planes of the buccal face in theapicocoronal direction, reductionVolume 22 Number 4
Clinical ScienceKahngFigure 15: Illusion of increased and decreased widthis to achieve symmetry of restorations.Figure 16: After bisque-bake and final contour,surface texture is checked with articulating paper.Figure 17: Try in of tooth #8 over a milled zirconiumabutment.Figure 18: Crown was tight at gingival, adjustmentmade using a diamond, being careful not to losetexture.Figure 19: Rubber wheel gingival area to a mediumpolish.Figure 20: Hand polished to a high shine to matchsame amount of shine of crown.Volume 22 Number 4Winter 2007 The Journal of Cosmetic Dentistry 95
Clinical ScienceKahngFigure 21: Try in of tooth #9.Figure 22: Right lateral view checking the line angles.Figure 23: Postoperative view: Immediate shot of thetwo zirconium crowns; #8 is a zirconium crown over amilled zirconium implant abutment.and/or elimination of convexity ofthe cervical third, with mesial anddistal transition line angle extendedup to the cervical area, or accentuation of the vertical ridges and linesare worked upon.Even though the color of a crowncoming out of the furnace can matchthe adjacent teeth perfectly, changing its surface texture will affecthow it blends into the surroundingdentition. Surface texture can affectmany factors, including brightness,color saturation, and luster (Fig 16).A technician can apply multiple porcelain buildup layers and demonstrate technical ability in this regard,but the quality of the surface textureof the result demonstrates how ultimately skillful they must be.The zirconium crowns were triedin (Fig 17). The gingival of the crown#8 on the implant abutment wastight at the tissue, so it was adjusted(Fig 18) with a diamond abrasive.You do not have to reglaze, but canhand polish. After the adjustmentwith the diamond, a rubber wheelis used (Fig 19) so the area has nicetexture and not too rough. Thenhand polished to a high shine (Fig20) and the crown is ready to try in(Fig 21) again.The final restorations werechecked showing the line angles, andemergence profile matching other96 The Journal of Cosmetic Dentistry Winter 2007teeth in the mouth and the implantwith crown (Fig 22). The immediate view of the zirconia crowns hasan emergence profile matching thecrown color matching of adjacentteeth inward and outward the sameangulation and shade matching wasan esthetic match (Fig 23).Observations andConclusionsZirconium can be a very usefulchoice in spite of the higher degreeof care required in working with it.Clearly, it possesses a higher flexural strength, approximately 1,200MPa.4 It eliminates the need formetal, and it gives excellent colorVolume 22 Number 4
Clinical ScienceKahngmatching.4 When combined withinternal staining, it allows the technician to have full control over thechroma, hue, and color value of atooth; and its ability to allow lightto pass through it creates a superior appearance of depth and life inthe tooth. But because its opacity ishigh, the dentist and the technicianmust be extremely meticulous. Also,when there is a lack of room, theremay be difficulty in achieving colorvalue and the proper degree of translucency. In providing a good supportframework, it generally requires asmuch room as possible.Today we expect all patients tobe well educated in dental advancements, and, working as a team, thedentist, the dental technician andthe patient can achieve the highestlevels of function and esthetics.AcknowledgementThe author thanks Dr. Cheryl A.Nakfoor, Streamwood, Illinois, for herdental work on this case; and Dr. Russell A. Spinazze, Mt. Prospect, Illinois,the patient.References1. Kois JC. The restorative-periodontal interface: Biological parameters. Periodontology 2000 11(1):29-38, 1996.2. Francischone CE, Vasconcelos, LW. MetalFree Esthetic Restoration: Procera Concept.Hanover Park, IL: Quintessence; 2003.3. Garber DA, Salama MA. The aestheticsmile: Diagnosis and treatment. Periodontology 2000 11(1):18-28, 1996.4. Fradeani M. Esthetic Rehabilitation inFixed Prosthodontics, Volume 1, EstheticAnalysis: A Systematic Approach to Prosthetic Esthetic Analysis. Hanover Park, IL:Quintessence; 2004.5. Gurel G. The Science and Art of Porcelain Laminate Veneers. Hanover Park, IL:Quintessence; 2003.vVolume 22 Number 4Winter 2007 The Journal of Cosmetic Dentistry 97
90 The Journal of Cosmetic Dentistry Winter 2007 Volume 22 Number 4 Several esthetically pleasing materials are available for restoring anterior teeth. All-ceramic or metal-free restorations are considered to be high in es- . showing the white zirconium cop-ing understructure. H