Transcription
Time to take gumdisease seriouslyThe societal and economicimpact of periodontitisCOMMISSIONED BYSPONSORED BY
Time to take gum disease seriouslyThe societal and economic impact of periodontitisTable of contents3Executive summary5About this report7Introduction8Chapter 1: A spotlight onperiodontitis and gum health12Chapter 2: Filling the gaps A societal approach to good oral health17Chapter 3: The cost effectivenessof good oral health24Conclusion26Appendix I: Country profiles32Appendix II: Tables and Figures36Appendix III: Modelling methods44 Appendix IV: References The Economist Intelligence Unit Limited 20212
Time to take gum disease seriouslyThe societal and economic impact of periodontitisExecutive summaryPeriodontal (gum) diseases are strikinglycommon across the globe, but also largelypreventable. Left untreated, they are the maincause of tooth loss and considered one of themain threats to oral health. In Western Europe,a region which offers some of the mostadvanced healthcare services to the generalpublic, developments in the preventionand management of periodontitis appearstagnant. The prevalence of periodontitis hasremained largely unchanged over the last 25years. The evidence-base shows periodontitis,which is the severe form of gum disease, hasassociations with diabetes, cardiovasculardiseases and over 50 non-communicablediseases. Recognition of these mutual riskfactors and knowledge sharing betweendentistry and general health are scarce inclinical practice. Similar to general health, poororal health is also strongly associated withlower socioeconomic status. Unlike accessingthe General Practitioner (GP), which in mostof Western Europe are free at the point ofaccess, many report avoiding dental checkups due to the upfront costs. This avoidanceonly exacerbates poor oral health in socioeconomically deprived neighbourhoods.Given the prevalence and preventablenature of periodontitis, new ways of thinkingabout gum health are needed to increaseawareness and action at national level. ThisEconomist Intelligence Unit (EIU) report aimsto capture the attention of policy makers insix European countries (France, Germany,Italy, the Netherlands, Spain and the UnitedKingdom), emphasising the economic andsocietal benefits of action and inactionin the early treatment of periodontitis.To improve early detection and preventionof periodontitis, this report arrives atthe following recommendations:Prevention, diagnosis and managementof periodontitis is cost-effective. Firstand foremost, the role of home care ledby patients is of paramount importance toprevent gingivitis and periodontitis. Oureconomic analysis shows that both eliminatinggingivitis (the precursor to periodontitis)using home care prevention techniques (suchas tooth brushing and interdental brushing)and increasing the rate of diagnosis andmanagement of periodontitis to 90%, hasa positive return on investment in all of theEuropean countries in this study. Makingefforts to eliminate gingivitis, thus preventingprogression to periodontitis, would saveconsiderable costs over a 10 year time periodcompared with ‘business as usual’ (36Bn Eurosin Italy to 7.8Bn Euros in the Netherlands).Neglecting to manage gingivitis cansignificantly increase costs and reduce HealthyLife Years (HLYs); therefore an emphasis onself-care and prevention is critical from bothan individual and a societal perspective.Better integration of dental and generalhealthcare. The value of integrating thesesystems in practice is still developing. Beingable to share information across disciplinesmay both improve patient care due to thecommon risk factors shared between somedental and physical health conditions andcontribute significantly to dental/general healthresearch. Integration may also encourageshared responsibility across healthcaredisciplines to address unmet oral health needsin vulnerable and marginalised communities. The Economist Intelligence Unit Limited 20213
Time to take gum disease seriouslyThe societal and economic impact of periodontitisA synergy of societal and individualpublic health campaigns are needed.One without the other would exacerbateoral health inequalities which we see bothwithin and across countries. Societal levelprevention is of crucial concern to theprevention of periodontitis, especially asit is a disease highly prevalent in deprivedareas. Individual public health campaignsneed to pay special attention to less affluentcommunities and embed preventionand early intervention interventions intocommunity settings such as schools (forthe prevention of caries) and health centres(for the prevention of gum disease).Improving the affordability of dental care.The cost of accessing a dentist is a barrierto receiving treatment early for many ofthe general public. Because of these costs,people are more likely to access the dentistwhen there is something wrong rather thanfor check-ups or preventative treatmentwhich is essential for avoiding periodontitis.Although dental care appears ‘free on paper’in countries such as the UK and France, onlypart of the dental procedures for treatingperiodontitis are covered and the remainderis paid for out-of-pocket. In countries such asSpain and Italy, most if not all periodontitistreatment is paid for out-of-pocket or viaprivate insurance. Periodontitis treatment fora low-income family is therefore renderedalmost unaffordable. In this study we haveprovided the evidence that professionallymanaged periodontitis is in fact cost-effectiveand therefore publically covered dental carefor periodontitis deserves a review from policymakers and commissioners Europe-wide. The Economist Intelligence Unit Limited 20214
Time to take gum disease seriouslyThe societal and economic impact of periodontitisAbout this reportThis report describes the methods and mainfindings from The Economist IntelligenceUnit’s research which assesses the evidencelinking improved periodontal health to betteroverall health outcomes, and showcases theeconomic and societal implications associatedwith periodontal health across six Europeancountries: France, Germany, Italy, theNetherlands, Spain and the United Kingdom.These countries were selected for theirgeographic, demographic, epidemiologic,and socioeconomic comparability. Professor Thomas Kocher, Director ofthe Periodontics unit; Chairman of theDepartment of Restorative Dentistry,Periodontology, Endodontics, PreventiveDentistry and Periodontics at the DentalSchool of Greifswald, Germany. Professor Stefan Listl, Professorin Quality & Safety of Oral HealthCare at Radboud University; Directorof Translational Health Economicsat Heidelberg University.The report presents the results of aliterature review and an economic returnon-investment model for preventing andmanaging periodontitis, analysed foreach country separately. To supplementthe information found in the publishedliterature, we conducted interviews withexperts, extracts of which are displayedin italics throughout the report. To note,the findings and views expressed in thisreport are those of the EIU. We extend oursincere appreciation to the following fortheir time and contributions to this work: Professor Bruno Loos, Professor inPeriodontology at the Academic Centrefor Dentistry Amsterdam (ACTA);Director of Research at ACTA. Professor Wagner Marcenes, Professorin Oral Epidemiology, Chair of AHi(affordablehealthinitiative.com). Professor Jose Nart, Professor,Chairman and Program Director,Department of Periodontology,UIC-Barcelona, Vice President of theSpanish Society of Periodontologyand Osseonintegration. Professor Ian Needleman, Professorof Restorative Dentistry and EvidenceBased Healthcare at UCL EastmanDental Institute; Honorary Consultantin Periodontology with UCLH, inspecialist practice at PerioLondon. Professor Panos Papapanou,Professor of Dental Medicine; Chairof the Section of Oral, Diagnostic andRehabilitation Sciences; Director ofthe Division of Periodontics, ColumbiaUniversity College of Dental Medicine. Professor Philippe Bouchard, Professorand Chairman of the Department ofPeriodontology, U.F.R. d’Odontologie, ParisGarancière, Université de Paris, France. Dr Stephan Carner, Associate Professor,Department of Periodontology, U.F.R.d’Odontologie Paris-Garancière,Université de Paris, France. Dr Nigel Carter, Chief Executive ofthe Oral Health Foundation, UK. Dr Pierpaolo Cortellini, Founder and boardmember of the European Research Groupin Periodontology, Private Practice, Italy. The Economist Intelligence Unit Limited 20215
Time to take gum disease seriouslyThe societal and economic impact of periodontitis Dr Andres Pascual La Rocca, SpecialistMember of the Spanish Society ofPeriodontology and Implants, Spain.Professor Mariano Sanz, Professor andChair of Periodontology, University ofComplutense of Madrid, Professor in theFaculty of Odontology, University of Oslo.Professor Lior Shapira, EFP President2021-22, Professor and Chair ofPeriodontology, at the HebrewUniversity–Hadassah Faculty ofDental Medicine in Jerusalem, Israel.Professor Maurizio Tonetti, ChairProfessor Shanghai Jiao Tong UniversitySchool of Medicine, Director ShanghaiPerioImplant Innovation Center, Shanghai9th People Hospital, Shanghai JiaoTong University; Executive directorof the European Research Group onPeriodontology, Genova, Italy.Dr Olaf Veth, Periodontist, OralImplantologist, Private practice,Zwolle, The Netherlands; assistingprofessor at the Department ofPeriodontology, ACTA, Amsterdam.Professor Freidus van Der Weijden,Owner of the Clinic for Periodontology andImplantology, Professor of the Departmentof Periodontology, ACTA, Amsterdam.Economic modelling conducted by David Tordrup, Managing Director andHealth Economist, Triangulate Health Ltd Tim Jesudason, Health Economist,Triangulate Health LtdEIU project team Chrissy Bishop – Project lead Araceli Irurzun Perez – project research Yogita Srivastava – project researchThanks to the European Federationof Periodontology team for providingclinical context and sources of data: Professor Iain Chapple, Professor/Head of Periodontology, Consultant inRestorative Dentistry at BirminghamDental School/Hospital. Sharon Legendre, Head ofOperations at the EuropeanFederation of Periodontology. Professor Nicola West, Professorof Periodontology, Head of ClinicalTrials Unit, Consultant in RestorativeDentistry Bristol Dental Hospital UK. The Economist Intelligence Unit Limited 20216
Time to take gum disease seriouslyThe societal and economic impact of periodontitisIntroductionYou would not ignore bleeding fromyour eye, so why would you ignorebleeding from your mouth?Professor Maurizio Tonetti,Executive Director of the EuropeanResearch group on Periodontology.Periodontitis may not be the first disease thatcomes to mind when thinking about globalpublic health problems, but periodontaldisease, consisting of both gingivitis andperiodontitis, is in fact the most commonglobal disease, alongside dental caries.1Periodontitis manifests across a spectrumof severity ranging from inflammation todisability. It is caused by inflammation of thegums and underlying bone due to build-up ofdental plaque. Symptoms range from bleedingand discomfort, to periodontal ligament lossand deterioration of the bone which holdsthe teeth in place. This can result in loss ofchewing function, speaking function, inabilityto smile and ultimately, relate with others.2Although treatable in a majority of cases,if left untreated, periodontitis is the maincause of tooth loss and is consideredone of the main threats to oral health inadults.3 It is also a threat to general health,as severe periodontitis, along with caries,tooth loss and other oral conditions areresponsible for more years lost to disabilitythan any other human disease,4 notablydue to its association with systemicdiseases like diabetes and cardiovasculardiseases, and causing physical discomfort.Periodontitis is sometimes referred to as a“silent disease”5 due to its slow and gradualprogression and its mild early symptoms.6This is a misnomer. Rather than silent,periodontitis is misinterpreted, as itsawareness among the general public, dentists,and other health professionals remainslow. Studies show three out of four adultswith periodontitis do not know they have acondition at all.7 While most general dentalpractitioners can manage uncomplicatedperiodontitis, gaps in advanced services exist.8This study captures the socioeconomicburden of periodontitis in two ways. Intangible, quantitative terms using aneconomic model and through exploringexisting policies and periodontitis practices,in addition to interviews with dental experts.In doing so, we hope to pave the way fora spotlight on periodontitis preventionpolicies across Europe, highlightingdisparities in best practices and proposingkey recommendations moving forward.Ultimately, this study seeks to reach four key aims:1.Evaluate the prevalence of periodontaldisease and review current policy2.Explore the integration of generalhealth with dental health tobetter manage periodontitis3.Understand the impact of individualand societal level oral healthprevention techniques to pinpointpotential improvements4.Compare economic and societal costsand benefits of action and inaction inthe treatment of early periodontitis. The Economist Intelligence Unit Limited 20217
Time to take gum disease seriouslyThe societal and economic impact of periodontitisChapter 1: A spotlight onperiodontitis and gum healthVery early periodontitis is oftenundiagnosed and causes variousproblems later in life such asdeveloping severe periodontitis.Severe periodontitis is the real publichealth problem, it does not onlyaffect the health of the gums, it hasimplications to the general health ofthe patient and their well-being.Professor Mariano Sanz, Professor and chair ofperiodontology, University of Madrid, Spain.Periodontitis fulfils Aubrey Sheiham’s (adental epidemiologist) criteria of a publichealth issue, due to its high prevalence,its impact on individuals and on society,and the fact that it remains preventableand treatable.9 Clinical definitions ofperiodontitis vary which has downstreamconsequences on the ways in which thedisease is measured in the population.Prevalence estimates can be over- orunderestimations,10 but on the whole, theavailable data indicates periodontitis isboth persistent and of high prevalence.“It is important to consider whendetermining the impact of periodontitisas a public health problem to understandthe proportion of the population affectedcompared to other health conditions”.Professor Panos Papapanou, Director ofthe Division of Periodontics, ColumbiaUniversity College of Dental Medicine.Periodontitis is the sixth-most prevalenthealth condition globally. According tothe Global Burden of Disease (2017)the prevalence of severe periodontitiswas 11% affecting approximately 743million people. Compared to some othercommon diseases, it is almost on par withthe prevalence of sexually transmittedinfections (16%) and is more common thancardiovascular disease (prevalence 6.6%).4 Theprevalence of milder forms of periodontitisare staggeringly common, affecting atleast half of the global population.11,12 The Economist Intelligence Unit Limited 20218
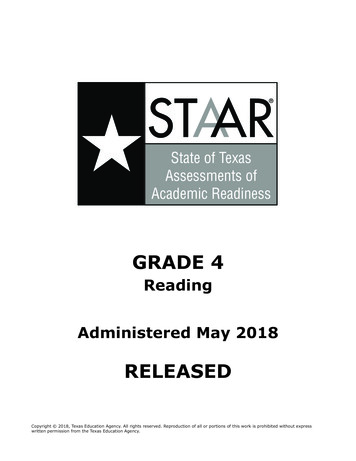
Time to take gum disease seriouslyThe societal and economic impact of periodontitisPrevalence of the main causes of global diseases for 195 countries and territories in 2017 4(%)Non-communicable diseasesNeurological disordersSexually Transmitted InfectionsDiabetes and kidney diseasesSevere periodontitisCardiovascular diseasesRespiratory infectionsMaternal and neonatal disorders0102030Across the six countries included in thisanalysis, prevalence has remained fairlystable over a 20-year time-period, butcontrasts remain between countries inEurope. For example, in 2010 the prevalenceof periodontitis in Spain stood at 4.3%, lowerthan the global average of 11%, but wasrelatively higher in Italy, at 13.1% (Table 1).There is also a clear pattern with age – morepeople have periodontitis when they are older.405060708090100Table 1 shows higher prevalence amongpeople aged 65-74 compared to ages 35-44in all countries where data is available. Reliableand comparable prevalence data is, however,difficult to come by,11 with the best estimatescoming from the Global Burden of Disease(GBD) study which covers severe cases only.10Table 1: Prevalence and incidence of severe periodontitis in Europe.CountryPrevalence of severeperiodontitis per 100population (GBD data)10Prevalence ofall periodontitispatients (Usingcommunityperiodontitis indexscores of 3 and 4)aged 65-74 as a % ofthe populationPrevalence ofall periodontitispatients (Usingcommunityperiodontitisindex scores of 3and 4) aged 3544 as a % of .Prevalenceof severe andmoderate perioin people ages20-75.Prevalence ofall perio in arandom sampleof people who’saverage agewas 5819902010Multiple datesMultiple 7)13No 8-22.3)10.5(4.6-20.9)No dataNo dataItaly13.6(11.6-15.7)13.1(11.2-15.3)No dataNo data16.2%1434.95% severe1540.78%moderate15 The Economist Intelligence Unit Limited 20219
Time to take gum disease seriouslyThe societal and economic impact of periodontitisIn Germany, about 30-40% of allextracted teeth are done so because ofperiodontal disease, and this seemsto be unchanged for the last 15 years.Professor Thomas Kocher, Director of Periodontics,Dental School of Griefswald, Germany.Despite improvements in the quality of oralhealth services in Europe and increasedawareness of the importance of oral hygiene,16the data suggests these have had littleimpact on the prevalence and incidence ofperiodontitis. In most European countries,the proportion of the population reportingunmet needs remains significantly higherfor dentistry than for general medical care.Around 8% of people in Portugal, Latvia andGreece reported unmet needs for dental carein 2018.17 A survey carried out in Portugal,Romania and Sweden showed that 74.9%of adolescents were not aware of the factthat tooth brushing can prevent periodontaldisease.18 The available evidence indicatesan urgent need for heightened awarenessof the burden of periodontitis, to improveboth prevention policies and access to care.Risk factors of periodontitisIncreasing age is a well-documented riskfactor for periodontitis. A steep increasein prevalence is shown in 30 and 40-yearolds19 and is generally highest in 65 to74 year olds.11 Only 1.7% of cases areamong younger populations.20 As theEuropean population continues to age,the demand for periodontal detectionand treatment rises, making it crucial todesign more effective prevention strategiesand trigger efficient policy responses.Periodontitis is often labelled a ‘socialdisease’, stressing its sensitivity to inequalitiesand behaviour.21-23 Less stringent dentalcare routines, poorer access to dentalpractices, and less frequent attendanceat preventative dental check-ups areassociated with living in disadvantagedareas.23 Periodontitis prevalence is clusteredamongst socioeconomically deprivedgroups across Europe,7 such as people livingin poverty, ethnic minorities and isolatedolder adults who have poor access to dentalcare. The disparities in dental outcomes andcare access between affluent and deprivedcommunities are so severe that a socialdeterminants-of-health approach must bepart of the process to improve outcomes.24Lifestyle choices also have a direct impacton the prevalence of periodontitis, and aremainly modifiable behaviours. Several studieshave consistently reinforced that smokingand poor diet are critical risk factors forperiodontal disease.4,12 Directly modifyingbehaviours, therefore, is a simple yet powerfulpolicy message for mitigating periodontitis.The periodontal pathway of careKnowing if you have gingivitis or periodontitisrequires an oral health assessment anddiagnosis. Around 90% of people havegingivitis globally, which is a superficialinflammation that presents as bleedinggums.25 Gingivitis if not managed canprogress to periodontitis, which is a deeperseated gum inflammation that destroys thebone that holds the teeth in the jaws. Thepresence of gingivitis is both a warning signand the primary intervention point for theprevention of periodontitis. Periodontitisalso presents with bleeding gums and thedamaged caused is irreversible, but can bestabilised such that teeth can be retained. The Economist Intelligence Unit Limited 202110
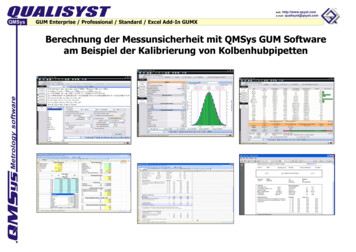
Time to take gum disease seriouslyThe societal and economic impact of periodontitisBoth gingivitis and periodontitis arepreventable and also treatable. The primarycare general dental practitioner has thecapacity to diagnose and manage 95%of periodontal cases.3 Treating gingivitisprevents the development of periodontitisand is simple to achieve in most people.The mainstay of treatment is reducingdental plaque build-up on teeth at andbelow the gum line. The role of home careby patients is of paramount importanceto prevent gingivitis and periodontitis,but requires training and instructionfrom the dental team, including speciallytrained dental nurses, dental hygienistsor dental surgeons. Treating periodontitisis more complex and costly, however therole of patient-delivered home care, withmeticulous tooth brushing and interdentalbrushing remains the most important aspectof treatment. Successful managementof periodontitis has also been shown tobenefit general health and well-being.The pathway for treatment and preventionof periodontitis should be life-long, patientcentered and composed of incrementalsteps3,26 (see Figure 2). This pathway ofcare is two-fold. It starts with an initialdiagnosis aimed at staging and gradingthe severity of the periodontal disease,27followed by sequential management of thedisease, which aims to regenerate boneand reverse gingival inflammation.28The official European treatment guidelinesfor periodontitis are split into 4 steps(Figure 2).3 If prevention is not achieved andperiodontitis is diagnosed, the first step ofmanagement involves informing the patientof the diagnosis and providing personallytailored treatment options with support onbehaviour change to ensure optimal oralhygiene and risk factor control. The secondstep of treatment aims to address the causesof the disease by controlling, and ultimatelyreducing the accumulation of plaque andcalculus. If the endpoints of therapy havenot been achieved through the second step,the third step may include surgery. Anysuccessfully treated periodontitis patientremains a periodontitis patient for life andundergoes supportive periodontal care.This last stage aims to maintain periodontalstability by combining therapeutic andpreventive methods, since periodontaldisease can progress if maintenance is suboptimal and risk factors are not controlled.3Figure 2: The periodontal pathway of care.Intervention point:ManagementStep 1 iagnosedperodontitisExtractunsavableteethStep 2 treatmentStep 3 treatmentStep 1 treatmentIntervention point:PreventionStabilised periodontitisStep 3 treatmentUnmanaged The Economist Intelligence Unit Limited 202111
Time to take gum disease seriouslyThe societal and economic impact of periodontitisChapter 2: Filling the gaps - A societalapproach to good oral healthOral health and general healthPeriodontitis can increase the risk oftype II diabetes and cardiovasculardisease, the inflammation ischronic. Having periodontalinflammation is more than acosmetic issue, the patient’s wellbeing is very much involved.Professor Philippe Bouchard, Professorand Chairman of Periodontology, U.F.R.d’Odontologie, France.While periodontitis is an urgent publichealth issue in and of itself, a growing bodyof evidence associates periodontitis withother systemic diseases. These associationsoccur via shared underlying pathways andexposure to common risk factors, such asage, socio-economic status and lifestylechoices. Periodontitis may also be a riskfactor for many systemic conditions due tothe presence of bacteria in the bloodstreamand pro-inflammatory proteins whichcan affect other parts of the body.4,29The evidence for these associations isstrongest for diabetes and cardiovasculardisease (CVD). There is a developing body ofevidence that suggests periodontitis patientsoften exhibit symptoms of coronary arterydisease.30,31 Some studies have found thatperiodontal disease is likely to cause a 19%increase in risk of cardiovascular disease,which increases to a 44% increased risk inpeople aged 65 and over.8 Bidirectional linksbetween periodontitis and diabetes havealso been established, meaning people withtype 1 and type 2 diabetes are at greaterrisk of developing periodontitis, just aspeople with periodontitis are at greaterrisk of developing type 2 diabetes.12Beyond CVD and diabetes, emerging evidencelinks periodontitis with cognitive decline,32Alzheimer’s disease33 and dementia.34,35 Someauthors suggest that periodontitis is a riskfactor for cognitive decline;35,36 others reportthat people with cognitive decline simplysuffer from inadequate oral health, stemmingfrom a loss in functionality, and are thereforemore likely to develop periodontitis.34An association between periodontal diseaseand various adverse pregnancy outcomes hasbeen reported.37-40 There are also tentativelinks with other conditions such as cancer,41rheumatoid arthritis42 and respiratory disease.43While further research is needed to studythese links in detail, there is sufficient evidencehighlighting the need for more integratedcare pathways between dentistry and generalhealth, breaking down the traditional silos andadvising patients diagnosed with periodontitisof the risks to general health and vice versa. The Economist Intelligence Unit Limited 202112
Time to take gum disease seriouslyThe societal and economic impact of periodontitisIntegrated general health anddental health care pathwaysThere is a split between the waymedicine is delivered and the waydentistry is delivered. The twodon’t talk to each other. In the UKfor example, although dentistryand medicine are all under thesame roof of the NHS, there is nointegration between dentistryand doctors. You can refer fromdentistry to secondary care butthere is no joined up thinking.Dr Nigel Carter, Chief Executive of the OralHealth Foundation, United Kingdom.In the periodontal treatment pathway, thereare opportunities to integrate general healthcheck-ups with oral health examinations.Better management of oral health could leadto better management of comorbidities, andthus lower overall health costs. This meansthe traditional segregation between dentaland general medical practice would greatlybenefit from being integrated in some way.Dental treatment and preventative adviceare mainly delivered in the dental chair,meaning that patients are consumers of aservice rather than being actively engaged ina preventative approach.44 Clinical treatmentteams could better adopt a dual role inproviding dental treatment, but also advisingpatients on how they can make choices thatimprove and maintain their general andoral health in synergy. Costs could also besaved by reducing the need for duplicationof prevention advice, and the number ofcontacts with different health professionals,by creating clinical pathways that complementboth dental and general medicine.45Using the link between diabetes andperiodontitis as an example, an integratedcare pathway could look as simple asensuring that patients with diabetes are signposted to a general dental practitioner forperiodontal screening. In addition, patientsattending a dental check-up could expectan oral health needs assessment, a clinicalexamination, screening for periodontitis andif periodontitis is diagnosed, an awarenessraising exercise about the risk of diabetes.8Many pilots and operational systems exist,showcasing how integration between generaland oral health can work. Yet there arestill lessons to be learnt in terms of bettermanaging comorbidities. For example, inEurope, the NHS has conducted research anddrawn networks of communication betweengeneral and dental health and aims to haveall parts of England served by an integratedcare system from April 2021.46 While thesenetworks have proven to be pioneeringexercises, in practice they have encounteredmany barriers to success, such as the cost ofdentistry (reported as too ambiguous or high)and failing to systematically address patients’and community’s needs. Further, the GermanDiabetes Association (DDG) is working onchecklists for general health practitionerswhich include oral care considerations.47There is very limited access tointegrated electronic healthrecords for dentists to reviewhealth information which wouldmake it very easy to exchangeinformation between oral andgeneral health care providers.Professor Stephan Listl, Quality andSafety of Oral Health Care, RadboudUniversity, The Netherlands. The Economist Intelligence Unit Limited 202113
Time to take gum disease seriouslyThe societal and economic impact of periodontitisThe increasing recognition of oral healthas a key contributor to overall health, hasencouraged the need for linking oral healthdata to general health data electronicallyto determine if certain dental servicesare associated with other types of healthoutcomes.48 Very few examples of integratedelectronic dental and medical recordsexist, despite dentists and physiciansagreeing that sharing information in thisway would be extremely useful.49The importance of homecare led by the individualDespite efforts to improve dentalhealth promotion, many peopleonly visit the dentist when there is atangible problem, not for check-upswhich have a preventative focus.Pro
The Economist Intelligence Unit imited 2021 Table of contents 3 Executive summary 5 About this report 7 Introduction 8 Chapter 1: A spotlight on periodontitis and gum health 12 Chapter 2: Filling the gaps - A societal approach to good oral health 17 Chapter 3: