Transcription
TOBACCO DEPENDENCE:A 2-PART PROBLEMMEDICATIONS for CESSATIONTobacco DependencePhysiologicalBehavioralThe addiction to nicotineThe habit of using tobaccoTreatmentMedications for cessationTreatmentBehavior change programTreatment should address the physiologicaland the behavioral aspects of dependence.NICOTINE WITHDRAWAL SYMPTOMS:Time Course* and ManagementIrritability / Frustration / AngerAnxietyDifficulty concentratingRestlessness / ImpatienceDepressed mood / DepressionInsomniaImpaired task performanceIncreased appetiteWeight gainCravings1 weekQuitdateMost symptoms manifestwithin the first 1–2 days,peak within the first week,and subside within 2–4 weeks.6 monthsCan persist for months toyears after quitting4 weeks12 weeksFormertobacco userRecent quitterMedications significantly improve success rates.FDA-APPROVED MEDICATIONSfor CESSATIONPharmacotherapy is not recommended for: Nicorette (OTC) Generic nicotine gum (OTC)Insufficient evidence of effectivenessSmokeless tobacco users Nicotine polacrilex gum*Pregnant smokers Nicotine lozenge*No FDA indication for smokeless tobacco cessation Nicorette (OTC) Generic nicotine lozenge (OTC)Individuals smoking fewer than 10 cigarettes per dayAdolescents Fiore et al. (2008). Treating Tobacco Use and Dependence: 2008 Update.Clinical Practice Guideline. Rockville, MD: USDHHS, PHS, May 2008.Data from Hughes. (2007). Nicotine Tob Res 9:315–327.PHARMACOTHERAPY:Use in SPECIAL POPULATIONS “Clinicians should encourage allpatients attempting to quit to useeffective medications for tobaccodependence treatment, except wherecontraindicated or for specificpopulations* for which there isinsufficient evidence of effectiveness.”* Includes pregnant women, smokeless tobacco users, light smokers, and adolescents. Cognitive & behavioral coping strategies Medications for cessation*Timeline aspect of the figure is not according to scale.PHARMACOTHERAPYNicotine transdermal patch*Nonprescription sales (patch, gum, lozenge) are restricted toadults 18 years of ageNRT use in minors requires a prescriptionRecommended treatment is behavioral counseling. NicoDerm CQ (OTC) Nicotrol (OTC) Generic nicotine patches (OTC)5Nicotine nasal spray* Nicotrol NS (Rx)Nicotine inhaler* Nicotrol (Rx)Bupropion SR Zyban (Rx) Generic bupropion SR (Rx)Varenicline Chantix (Rx)* Nicotine replacement therapy (NRT) products.Copyright 1999-2019 The Regents of the University of California. All rights reserved. Updated January 2019.1
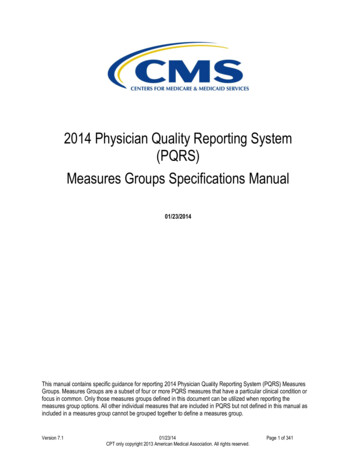
PLASMA NICOTINE CONCENTRATIONSfor NICOTINE-CONTAINING PRODUCTSNICOTINE REPLACEMENT THERAPY (NRT)RATIONALE for USE25CigaretteReduces physical withdrawal from nicotine CigarettePlasma nicotine (mcg/l)Allows patient to focus on behavioral andpsychological aspects of tobacco cessation Moist snuff20Eliminates the immediate, reinforcing effectsof nicotine that is rapidly absorbed via tobaccosmoke Moist snuffNasal spray15Inhaler10Lozenge (2mg)Gum 00302/9/1900402/19/1900502/29/190060Time (minutes)NRT products approximately doubles quit rates.NICOTINE GUMNRT: PRECAUTIONS Patients with underlying cardiovasculardisease Recent myocardial infarction (within past 2weeks) Serious arrhythmias Serious or worsening anginaNicorette; generics Resin complex NicotinePolacrilinSugar-free chewing gum baseContains buffering agents to enhancebuccal absorption of nicotineAvailable: 2 mg, 4 mg; original, cinnamon,fruit, and mint (various) flavorsNRT products may be appropriate for these patientsif they are under medical supervision.NICOTINE LOZENGENicorette Lozenge and Nicorette Mini Lozenge;generics Nicotine polacrilex formulation Delivers 25% more nicotinethan equivalent gum doseSugar-free mint, cherry flavorsContains buffering agents toenhance buccal absorption ofnicotineAvailable: 2 mg, 4 mgNICOTINE GUM & LOZENGE:DOSINGDose based on the “time to first cigarette” (TTFC)as an indicator of nicotine dependenceUse the 2 mg gum/lozenge:If first cigarette of the day issmoked more than 30 minutesafter wakingUse the 4 mg gum/lozenge:If first cigarette of the day issmoked within 30 minutes ofwakingCopyright 1999-2019 The Regents of the University of California. All rights reserved. Updated January 2019.2
NICOTINE GUM & LOZENGE:DOSING (cont’d)NICOTINE GUM:DIRECTIONS FOR USEChew slowlyRecommended Usage ScheduleWeeks 1–6Weeks 7–91 piece q 1–2 h 1 piece q 2–4 hWeeks 10–121 piece q 4–8 hStop chewing atfirst sign of pepperytaste or tinglingsensationChew againwhen pepperytaste or tinglefadesPark betweencheek & gumDo not use more than 24 pieces of GUM or 20 LOZENGES per day. NICOTINE GUM/LOZENGE:ADDITIONAL PATIENT EDUCATIONNICOTINE LOZENGE:DIRECTIONS for USE Place in mouth and allow to dissolve slowly (nicotinerelease may cause warm, tingling sensation) Do not chew or swallow Occasionally rotate to different areas of the mouth Lozenges will dissolve completely in about 20 30minutes To improve chances of quitting, use at least nine piecesdaily during the first 6 weeksThe gum/lozenge will not provide the same rapidsatisfaction that smoking providesThe effectiveness of the nicotine gum/lozenge may bereduced by some foods and beverages: Coffee Juices Wine Soft drinksDo NOT eat or drink for 15 minutes BEFORE orwhile using the nicotine gum or lozenge.NICOTINE GUM/LOZENGE:ADD’L PATIENT EDUCATION Chewing the lozenge or using incorrect gumchewing technique can cause excessive and rapidrelease of nicotine, resulting in: Lightheadedness/dizziness Nausea and vomiting Hiccups Irritation of throat and mouth IndigestionNICOTINE GUM/LOZENGE:ADD’L PATIENT EDUCATION(cont’d) (cont’d)Adverse effects of nicotine gum and lozenge: Mouth and throat irritation Hiccups Gastrointestinal complaints (dyspepsia, nausea)Adverse effects associated with nicotine gum: Jaw muscle ache May stick to dental workCopyright 1999-2019 The Regents of the University of California. All rights reserved. Updated January 2019.3
NICOTINE GUM/LOZENGE:SUMMARY NicoDerm CQ; genericDISADVANTAGESADVANTAGES TRANSDERMAL NICOTINE PATCHMight serve as an oralsubstitute for tobaccoMight delay weight gainCan be titrated to managewithdrawal symptomsCan be used incombination with otheragents to managesituational urgesRelatively inexpensive Need for frequent dosing cancompromise adherence Continuous (24-hour) nicotine delivery system Nicotine is well absorbed across the skin Gastrointestinal adverse effects(nausea, hiccups, anddyspepsia) may be bothersome Specific to nicotine gum:Transdermal delivery to systemic circulation avoidshepatic first-pass metabolismPlasma nicotine levels are lower and fluctuate lessthan with smoking Might be problematic for patientswith significant dental work Proper chewing technique isnecessary for effectiveness and tominimize adverse effects Chewing might not be acceptable ordesirable for some patientsTRANSDERMAL NICOTINE PATCH:DOSINGProductNicoDerm CQLight SmokerHeavy Smoker 10 cigarettes/day 10 cigarettes/dayStep 2 (14 mg x 6 weeks)Step 1 (21 mg x 6 weeks)Step 3 (7 mg x 2 weeks)Step 2 (14 mg x 2 weeks) 10 cigarettes/day 10 cigarettes/dayStep 3 (7 mg x 2 weeks)GenericStep 2 (14 mg x 6 weeks)Step 1 (21 mg x 4 weeks)Step 3 (7 mg x 2 weeks)Step 2 (14 mg x 2 weeks)TRANSDERMAL NICOTINE PATCH:DIRECTIONS for USE Choose an area of skin on the upperbody or upper outer part of the armMake sure skin is clean, dry, hairless,and not irritatedApply patch to different area each dayDo not use same area again for atleast 1 weekStep 3 (7 mg x 2 weeks)TRANSDERMAL NICOTINE PATCH:DIRECTIONS for USE (cont’d) Remove protective liner andapply adhesive side of patchto skinPeel off remaining protectivecoveringPress firmly with palm ofhand for 10 secondsMake sure patch sticks wellto skin, especially aroundedgesTRANSDERMAL NICOTINE PATCH:DIRECTIONS for USE (cont’d) Wash hands: Nicotine on hands can get into eyes ornose and cause stinging or rednessDo not leave patch on skin for more than 24 hours—doing so may lead to skin irritationAdhesive remaining on skin may be removed withrubbing alcohol or acetoneDispose of used patch by folding it onto itself,completely covering adhesive areaCopyright 1999-2019 The Regents of the University of California. All rights reserved. Updated January 2019.4
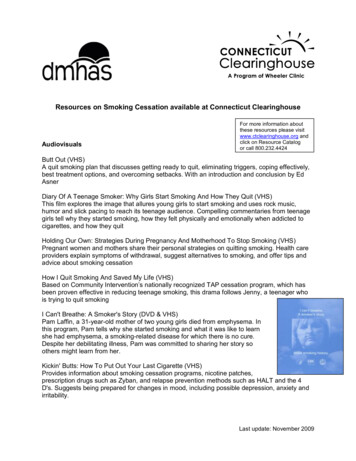
TRANSDERMAL NICOTINE PATCH:ADD’L PATIENT EDUCATION (cont’d)TRANSDERMAL NICOTINE PATCH:ADDITIONAL PATIENT EDUCATION Common adverse effects include:Water will not harm the nicotine patch if it isapplied correctly; patients may bathe, swim,shower, or exercise while wearing the patch Do not cut patches to adjust dose Can unpredictably effect nicotine delivery Patch may be less effectiveIrritation at the patch application site (generallywithin the first hour) Keep new and used patches out of the reach ofchildren and pets Sleep disturbances Remove patch before MRI procedures TRANSDERMAL NICOTINE PATCH:ADD’L PATIENT EDUCATION (cont’d) After patch removal, skin may appear red for 24 hours If skin stays red more than 4 days or if it swells or arash appears, contact health care provider—do not applynew patchLocal skin reactions (redness, burning, itching) Usually caused by adhesiveUp to 50% of patients experience this reactionFewer than 5% of patients discontinue therapyAvoid use in patients with dermatologic conditions (e.g.,psoriasis, eczema, atopic dermatitis)Mild itchingBurningTinglingAbnormal or vivid dreamsInsomniaTRANSDERMAL NICOTINE PATCH:SUMMARYADVANTAGES DISADVANTAGESOnce-daily dosingassociated with feweradherence problemsOf all NRT products, its useis least obvious to othersCan be used incombination with otheragents; delivers consistentnicotine levels over 24 hrs When used asmonotherapy, cannot betitrated to acutely managewithdrawal symptomsNot recommended for useby patients withdermatologic conditions(e.g., psoriasis, eczema,atopic dermatitis)Relatively inexpensiveNICOTINE INHALER:SCHEMATIC DIAGRAMNICOTINE INHALERNicotrol InhalerAir/nicotine mixture out Nicotine inhalation systemconsists of: MouthpieceCartridge with porous plugcontaining 10 mg nicotine and1 mg mentholSharp point thatbreaks the sealAluminum laminatesealing materialSharp point thatbreaks the sealDelivers 4 mg nicotinevapor, absorbed acrossbuccal mucosaMouthpiecePorous plug impregnatedwith nicotineAir inNicotinecartridgeReprinted with permission from Schneider et al. (2001). Clinical Pharmacokinetics40:661–684. Adis International, Inc.Copyright 1999-2019 The Regents of the University of California. All rights reserved. Updated January 2019.5
NICOTINE INHALER:DIRECTIONS for USENICOTINE INHALER: DOSING Initial treatment (up to 12 weeks) Increase prn to maximum of 16 cartridges/day In general, use 1 cartridge every 1–2 hoursGradually reduce daily dosage over the following6–12 weeksRecommended maximum duration of therapy is 6monthsNICOTINE INHALER:DIRECTIONS for USE(cont’d)Pull and separate mouthpiece into two parts NICOTINE INHALER:DIRECTIONS for USE Line up the markings on the mouthpiece again andpush the two pieces back together so they fit tightlyTwist top to misalign marks and secure unitNICOTINE INHALER:ADDITIONAL PATIENT EDUCATION Inhale into back of throat or puff in short breathsNicotine in cartridges is depleted after about 20 minutesof active puffing (cont’d)Press nicotine cartridgefirmly into bottom ofmouthpiece until it popsdown into place(cont’d)During inhalation, nicotine is vaporized and absorbedacross oropharyngeal mucosa Align marks on the mouthpieceStart with at least 6 cartridges/day during the first3–6 weeks of treatmentNICOTINE INHALER:DIRECTIONS for USE Cartridge does not have to be used all at once—try differentschedules (e.g., 5 minutes at a time) to find what works bestOpen cartridge retains potency for 24 hours Adverse effects associated with the nicotine inhalerinclude: Mild irritation of the mouth or throat Cough Hiccups Gastrointestinal complaints (dyspepsia, nausea)Severity generally rated as mild, and frequency ofsymptoms declined with continued useMouthpiece is reusable; clean regularly with milddetergentCopyright 1999-2019 The Regents of the University of California. All rights reserved. Updated January 2019.6
NICOTINE INHALER:ADD’L PATIENT EDUCATION NICOTINE INHALER: SUMMARY(cont’d)Use inhaler at room temperature ( 60 F); in coldenvironments, the delivery of nicotine vapor maybe compromisedUse the inhaler longer and more often at first tohelp control cravings (best results are achievedwith frequent continuous puffing over 20 minutes)Effectiveness of the nicotine inhaler may bereduced by some foods and beveragesDo NOT eat or drink for 15 minutes BEFOREor while using the nicotine inhaler.ADVANTAGES Might serve as an oralsubstitute for tobaccoCan be titrated to managewithdrawal symptomsMimics the hand-to-mouthritual of smoking Aqueous solution of nicotinein a 10-ml spray bottle Each metered doseactuation delivers 50 mcL spray 0.5 mg nicotine 100 doses/bottleRapid absorption acrossnasal mucosaPress in circles on sides of bottle and pull toremove cap Cartridges might be lesseffective in coldenvironments ( 60 F)Cost of treatmentOne dose 1 mg nicotine(2 sprays, one 0.5 mg spray in each nostril)Start with 1–2 doses per hourIncrease as needed to maximum dosage of 5 dosesper hour or 40 mg (80 sprays; ½ bottle) daily At least 8 doses daily for the first 6–8 weeks Termination:NICOTINE NASAL SPRAY:DIRECTIONS for USE Need for frequent dosingcan compromise adherenceNICOTINE NASAL SPRAY:DOSING & ADMINISTRATIONNicotrol NS Can be used incombination with otheragents to managesituational urgesNICOTINE NASAL SPRAY DISADVANTAGES Gradual tapering over an additional 4–6 weeks Recommended maximum duration of therapy is 3 monthsNICOTINE NASAL SPRAY:DIRECTIONS for USE (cont’d) Prime the pump (before first use) Re-prime (1–2 sprays) if spray not used for24 hoursBlow nose (if not clear)Tilt head back slightly and insert tip ofbottle into nostril as far as comfortableBreathe through mouth, and sprayonce in each nostrilDo not sniff or inhale while sprayingCopyright 1999-2019 The Regents of the University of California. All rights reserved. Updated January 2019.7
NICOTINE NASAL SPRAY:DIRECTIONS for USE (cont’d)NICOTINE NASAL SPRAY:ADDITIONAL PATIENT EDUCATION If nose runs, gently sniff to keep nasal spray in noseWait 2–3 minutes before blowing nose Avoid contact with skin, eyes, and mouth If contact occurs, rinse with water immediately Nicotine is absorbed through skin and mucous membranes What to expect (first week): Adverse effects should lessen over a few days Can be titrated to rapidlymanage withdrawalsymptomsCan be used incombination with otheragents to managesituational urgesDISADVANTAGES Need for frequent dosing cancompromise adherenceBUPROPION SR:Zyban; generics Nasal administration might notbe acceptable/desirable forsome patients; nasal irritationoften problematicNot recommended for use bypatients with chronic nasaldisorders or severe reactiveairway disease Non-nicotine cessation aidMechanism of action: atypical antidepressantthought to affect levels of various pamine Norepinephrine craving for cigarettes symptoms of nicotine withdrawalBUPROPION:CONTRAINDICATIONS Metabolism Undergoes extensive hepatic metabolism (CYP2B6) Elimination Urine (87%) and feces (10%) Half-life Bupropion (21 hours); metabolites (20–37 hours) Clinical effectsCost of treatmentAbsorption Bioavailability: 5–20%Regular use during the first week will help in development oftolerance to the irritant effects of the sprayIf adverse effects persist after a week, contact healthcare provider and consider alternative treatmentNICOTINE NASAL SPRAY:SUMMARYADVANTAGESHot peppery feeling in back of throat or noseSneezingCoughingWatery eyesRunny nose Patients with a seizure disorderPatients with a current or prior diagnosis ofbulimia or anorexia nervosaPatients undergoing abrupt discontinuation ofalcohol, benzodiazepines, barbiturates andantiepileptic drugsPatients taking MAO inhibitors (within 14 days ofinitiating or discontinuing therapy)Copyright 1999-2019 The Regents of the University of California. All rights reserved. Updated January 2019.8
BUPROPION:WARNINGS and PRECAUTIONSBupropion should be used with caution in thefollowing populations: Severe head injuryConcomitant use of medications that lower the seizurethreshold (e.g., other bupropion products,antipsychotics, tricyclic antidepressants, theophylline) Changes in mood (including depression and mania) Psychosis/hallucinations/paranoia/delusions Homicidal ideation Aggression/hostility/anxiety/panic Suicidal ideation, suicide attempt, completed suicidePatients with underlying neuropsychiatric conditionsAdvise patients to stop taking bupropion SR and contact a health care providerimmediately if symptoms such as agitation, depressed mood, or changes inbehavior or thinking that are not typical are observed or if the patient developssuicidal ideation or suicidal behavior.BUPROPION:ADVERSE EFFECTSBUPROPION SR: DOSINGTo ensure that therapeutic plasma levels of the drugare achieved, patients should begin therapy 1 to 2weeks PRIOR to their quit date.Common adverse effects include the following:Initial treatment 150 mg po q AM for 3 days 150 mg po bid for 7–12 weeksDoses must be administered at least 8 hours apartTapering not necessary when discontinuing therapy Oral dosing is simple andassociated with feweradherence problemsCan be used in combinationwith NRT agentsDry mouth Nausea Anxiety/difficulty concentrating Constipation Tremor Skin rashDISADVANTAGES Might delay weight gainBupropion might bebeneficial in patients withdepressionInsomnia (avoid bedtime dosing) VARENICLINEChantixBUPROPION SR: SUMMARYADVANTAGES Less common but reported effects:Then FDAboxedwarningremovedDec 2016Severe hepatic impairmentFor a comprehensive listing of warnings and precautions, refer to the manufacturer’s prescribing information. (cont’d)Neuropsychiatric symptoms and suicide riskPatients with an elevated risk for seizures, including: BUPROPION:WARNINGS and PRECAUTIONS Seizure risk is increasedSeveral contraindicationsand precautions precludeuse in some patientsPatients should bemonitored forneuropsychiatric symptoms Nonnicotinecessation aidPartial nicotinicreceptor agonistOral formulationRelatively inexpensive(generic formulations)Copyright 1999-2019 The Regents of the University of California. All rights reserved. Updated January 2019.9
VARENICLINE:MECHANISM of ACTION VARENICLINE:PHARMACOKINETICSBinds with high affinity and selectivity at 4 2neuronal nicotinic acetylcholine receptors Stimulates low-level agonist activity Competitively inhibits binding of nicotine symptoms of nicotine withdrawalBlocks dopaminergic stimulation responsible forreinforcement & reward associated with smokingNeuropsychiatric symptoms and suicide risk Changes in mood (including depression and mania) Psychosis/hallucinations/paranoia/delusions FDAboxedwarningremovedDec 2016Homicidal ideationAggression/hostility/anxiety/panicSuicidal ideation, suicide attempt, completed suicideAdvise patients to stop taking varenicline and contact a health care providerimmediately if symptoms such as agitation, depressed mood, or changes inbehavior or thinking that are not typical are observed or if the patient developssuicidal ideation or suicidal behavior.VARENICLINE: STANDARDDOSINGPrimarily renal through glomerular filtration and activetubular secretion; 92% excreted unchanged in urineHalf-life 24 hoursVARENICLINE:WARNINGS and PRECAUTIONS(cont’d)In some patients, use of varenicline has beenassociated with: Seizures Enhanced effects of alcohol Accidental injury Cardiovascular events Somnambulism Angioedema and hypersensitivity reactions Serious skin reactionsThese are rare events and most have not been causally linked to varenicline use.VARENICLINE QUIT APPROACHESPatients should begin therapy 1 week PRIOR to theirquit date. The dose is gradually increased to minimizetreatment-related nausea and insomnia.InitialdosetitrationUndergoes minimal metabolismEliminationVARENICLINE:WARNINGS and PRECAUTIONS Virtually complete ( 90%) after oral administration; notaffected by foodMetabolismClinical effects AbsorptionTreatment DayDoseDay 1 to day 30.5 mg qdDay 4 to day 70.5 mg bidDay 8 to end of treatment*1 mg bid* Up to 12 weeksFIXED QUIT approach– Set quit date for 1 week after starting varenicline– Continue treatment for 12 weeksFLEXIBLE QUIT approach– Start taking varenicline and pick a quit date between8 to 35 days from treatment initiation– Continue treatment for 12 weeksGRADUAL QUIT approach– Start taking varenicline and reduce smokingby 50% within the first 4 weeks, an additional50% in the next 4 weeks, and continue untilcomplete abstinence by 12 weeksImages from: -approaches.Copyright 1999-2019 The Regents of the University of California. All rights reserved. Updated January 2019.10
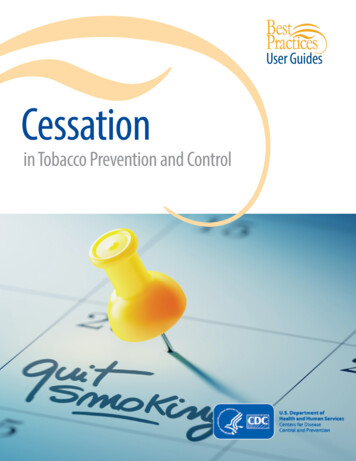
VARENICLINE:ADVERSE EFFECTSVARENICLINE:ADDITIONAL PATIENT EDUCATIONCommon adverse effects include the following: Nausea Insomnia Abnormal dreams Headache Doses should be taken after eating, with a full glass of water Nausea and insomnia are usually temporary side effects Less common adverse effects: Gastrointestinal (flatulence, constipation) Taste alteration If symptoms persist, notify your health care providerMay experience vivid, unusual or strange dreams duringtreatmentUse caution driving, drinking alcohol, and operatingmachinery until effects of quitting smoking with vareniclineare knownLONG-TERM ( 6 month) QUIT RATES forAVAILABLE CESSATION MEDICATIONSVARENICLINE: SUMMARY DISADVANTAGESOral dosing is simple andassociated with feweradherence problemsOffers a different mechanismof action for persons whohave failed other agents 30Cost of treatmentPatients should be monitoredfor potential neuropsychiatricsymptomsMost effective agent forcessation when used asmonotherapy28.5Active drugPlacebo2523.921.0Percent ngeNicotinenasal sprayNicotineinhalerBupropionVareniclineData adapted from Hartmann-Boyce et al. (2018). Cochrane Database Syst Rev;Cahill et al. (2016). Cochrane Database Syst Rev; Hughes et al. (2014). Cochrane Database Syst RevCOMBINATION PHARMACOTHERAPYRegimens with enough evidence to be ‘recommended’ first-line Combination NRTLong-acting formulation (patch) Produces relatively constant levels of nicotinePLUSShort-acting formulation (gum, inhaler, lozenge, nasal spray) Allows for acute dose titration as needed for nicotinewithdrawal symptomsBupropion SR Nicotine PatchTREATMENT OPTIONSMultiple Treatment Comparison Meta-AnalysisComparisonOdds ratio (95% CI)Nicotine gum vs PlaceboBupropion SR vs Placebo1.7 (1.5–1.9)1.9 (1.6–2.1)Nicotine patch vs PlaceboOther NRT* vs Placebo1.9 (1.7–2.1)2.0 (1.8–2.4)Combination NRT vs PlaceboVarenicline vs Placebo2.7 (2.1–3.7)2.9 (2.4–3.5)*Includes nicotine nasal spray, lozenge, and inhalerStrong evidence that combination NRT and varenicline are more effectivethan bupropion SR or NRT monotherapyCahill et al. (2013). Cochrane Database Syst Rev 5:CD009329.Copyright 1999-2019 The Regents of the University of California. All rights reserved. Updated January 2019.11
COMBINATION NRT:TREATMENT REGIMENSIDENTIFY KEY ISSUES toSTREAMLINE PRODUCT SELECTION* Nicotine patchDose: 21 mg/day x 4–6 wks 14 mg/day x 2 wks 7 mg/day x 2 wksPLUS Nicotine gum or lozenge (2 mg/4 mg; based on TTFC)Dose: Use 1 piece q 1–2 hours as needed (use at least 4-5/day)OR Nicotine inhaler (10 mg cartridge; delivers 4 mg nicotine vapor)Dose: Use 1 cartridge q 1–2 hours as neededOR Nicotine nasal spray (0.5 mg/spray)Dose: Use 1 spray in each nostril q 1–2 hours as neededDo you prefer a prescription or nonprescriptionmedication?Would it be a challenge for you to take a medicationfrequently throughout the day (e.g., a minimum of 9times)? With the exception of the nicotine patch, all NRTformulations require frequent dosing throughout the day.If patient is unable to adhere to the recommended dosing,these products should be ruled out as monotherapybecause they will be ineffective.Asking these two questions will significantly reduce the time required for product selection.* Product-specific screening—for warnings, precautions, contraindications,and personal preferences—is also essential.ADHERENCE IS KEY toQUITTING“Drugs don’t work in patients whodon’t take them.”Promote adherence with prescribed regimens C. Everett Koop, M.D., former U.S. Surgeon GeneralConsider telling the patient: Medication adherence should beaddressed at each encounter.ADHERENCE IS KEY toQUITTING (cont’d)Daily use (use according to dosing schedule, NOT as needed)Full duration of treatment regimen“If used properly, the medicines can make you morecomfortable while you are quitting.”“Medicines for quitting work best if you take them on aregular schedule, to prevent withdrawal symptoms beforethey occur. If you wait until you’re already craving a cigarette,it will be too late. The medicines don’t work as quickly asinhaled nicotine from a cigarette.”COMPARATIVE DAILY COSTSof PHARMACOTHERAPYWhen providing medication counseling, it is importantto emphasize three key facets of adherence:Average /pack of cigarettes in the US, 6.26 16 14Correct strength of medication Taken daily, according to a fixed schedule Taken for the full duration of therapyAt each encounter, assess withdrawal andadjust treatment as needed. /day 12 10 8 6 4 2 0TradeGenericGumLozengePatchNasal sprayInhaler 3.60 1.90 3.60 3.33 2.90 1.52 8.72 14.88BupropionSR 8.25 2.58Varenicline 15.14*Wholesale acquisition cost from Red Book Online. Thomson Reuters, December 2018.Copyright 1999-2019 The Regents of the University of California. All rights reserved. Updated January 2019.12
SUMMARY To maximize success, interventions should include behavioralcounseling and one or more medicationsEncourage the use of effective medications by all patientsattempting to quit smoking Exceptions include medical contraindications or specific populations forwhich there is insufficient evidence of effectivenessFirst-line medications that reliably increase long-term smokingcessation rates include: Bupropion SR Nicotine replacement therapy (as monotherapy or combination therapy) VareniclineVarenicline and combination therapy approaches demonstratethe highest level of efficacyCopyright 1999-2019 The Regents of the University of California. All rights reserved. Updated January 2019.13
1 piece q 1–2 h 1 piece q 2–4 h 1 piece q 4–8 h Do not use more than 24 pieces of GUM or 20 LOZENGES per day. NICOTINE GUM: DIRECTIONS FOR USE Park between cheek & gum Stop chewing at first sign of peppery taste or tingling sensation Chew slowly Chew again when peppery t