Transcription
Leukemia: AML, CML, ALL and CLLWWW.RN.ORG Reviewed October, 2019, Expires October, 2021Provider Information and Specifics available on our WebsiteUnauthorized Distribution Prohibited 2019 RN.ORG , S.A., RN.ORG , LLCBy Wanda Lockwood, RN, BA, MAPurposeThe purpose of this course is to define leukemia, describe currenttreatment, and describe the characteristics, symptoms, diagnosis, andtreatment for the 4 primary types of leukemia: AML, CML, ALL, andCLL.GoalsUponto: completion of this course, the healthcare provider should be ableDefine leukemia.Discuss hematopoiesis of leukemia.Differentiate between acute and chronic forms.Describe at least 8 common symptoms of leukemia.Discuss normal and abnormal laboratory tests.Explain how to calculate the absolute neutrophil count.Discuss the implications of neutropenia.Discuss the normal platelet count and the implications ofthrombocytopenia.Discuss the 3 common stages of chemotherapy.Explain the cell cycle and the difference between cell cyclespecific agents and cell cycle-non-specific agents.Discuss 10 different types of chemotherapeutic agents.Explain 3 types of radiation commonly used for leukemia.Discuss hematopoietic stem cell transplantation.Discuss acute myelogenous leukemia (AML), includingcharacteristics, symptoms, diagnostic findings, and treatmentconsiderations.Discuss subtypes of AML.Discuss chronic myelogenous leukemia (CML), includingcharacteristics, symptoms, diagnostic findings, and treatmentconsiderations.Discuss the 3 different phases of CML.
Discuss acute lymphocytic leukemia (ALL), includingcharacteristics, symptoms, diagnostic findings, and treatmentconsiderations.Discuss subtypes of ALL.Discuss chronic lymphocytic leukemia (CLL), includingcharacteristics, symptoms, diagnostic findings, and treatmentconsiderations.Discuss two classification systems for CLL.IntroductionLeukemia is a group of malignant disorders affecting the blood andblood-forming tissues in the bone marrow, lymphatic system, andspleen. The word leukemia literally means “white blood” because it is aneoplastic proliferation of one type of blood cell, typically a leukocyteor white blood cell. Leukocytosis, an increased white blood cell count,is a normal response to infection, but when leukocytosis becomeschronic or progressively elevates without obvious cause, then it mayindicate malignancy.In 2010, approximately 43,050 men and women (24,690 men and21,840 women) in the United States were diagnosed with leukemia,and 21,840 died of the disease. Leukemia accounts for 33% ofcancers in children and 1340 deaths yearly, so it is often thought of asa disease of childhood. In children, the highest incidence is between 1to 4 and the highest death rate between 10 and 19. However,incidence is 10 times higher in adults. The median age for diagnosis is66, and median age of death from leukemia is 74.Despite much research into leukemia, the cause is often elusive.Leukemia appears to result from a combination of factors, which caninclude genetic predisposition, chromosomal changes, chemical agents(benzene), chemotherapeutic agents, radiation, immunocompromise,and viruses. Although viruses have been tied to leukemias in animals,only adult T cell leukemia is known to result from a virus, human T cellleukemia virus type 1 (HTLV-1).
Regardless of the type of leukemia, the abnormal cells in the bonemarrow depress production of other cells, resulting in a number ofadverse effects: Anemia occurs as erythrocyte (red blood cell) production falls. Risk of infection occurs if neutrophil count decreases. Clotting factors decrease, increasing risk of bleeding asthrombocytopenia (reduced platelet count) occurs. Risk of physiological fracture increases as periosteum weakensbecause of proliferation of cells in the bone marrow. Hypertrophy and fibrosis may occur in other organs, such as theliver, spleen, and lymph glands because of infiltration ofmalignant cells. Increased intracranial pressure, ventricular dilation, and irritationof the meniges with resultant headache, vomiting, papilledema,nuchal rigidity, coma, and death can occur from infiltration ofmalignant cells into the central nervous system. Hypermetabolic state deprives cells of nutrients and causes lossof appetite, weight loss, general fatigue, and muscle atrophy.Classification
Hematopoiesis, the process by which blood cells are formed, involvesproduction of specific cells from stem cell precursors according to bodyneeds. In leukemia, a defect occurs in the myeloid or the lymphoidstem cell. The most common feature of all types of leukemia isunregulated proliferation of leukocytes in the bone marrow.Leukemias are classified as lymphoid or myeloid, depending on theaffected stem cell type. Usually leukemias classified as blast cell orstem cell refer to lymphoid defects. Additionally, leukemias areclassified as acute or chronic.The 4 primary types of leukemia are acute lymphocytic/lymphoblasticleukemia (ALL), acute myelogenous leukemia (AML) or acutenonlymphoblastic leukemia (ANLL), chronic myelogenous leukemia(CML), and chronic lymphocytic leukemia (CLL) with a number ofsubtypes. Leukemias are often referred to by a number of differentnames, depending on the involved cell, and this can be confusing attimes.Acute and chronic forms differ in cell maturity and onset: Acute forms: Onset is often abrupt, within weeks, and deathmay occur within weeks to months without treatment.Proliferation of abnormal cells leaves little room for normal cellproduction. Cells may proliferate in the liver and spleen as well,
and they may infiltrate other organs, such as the meninges,gums, lymph nodes, and skin.Typically, leukocyte development halts at the blast phase, somost affected leukocytes are undifferentiated or blasts. Withacute leukemia, the white blood count may remain low becausethe cells are halted at the blast stage. Acute forms may occur inboth adults and children. Chronic forms: Onset is much slower, often over months oryears. Normal cell production may occur as well for a long periodof time, but in late stages of chronic disease, the abnormal cellsinterfere with normal cell production. The majority of leukocytesare mature. Chronic forms are rare in children.Laboratory testsLeukocytes are white blood cells (WBCs). Normal total values varyaccording to age. The white count usually increases with infection andreturns to normal when infection subsides.Leukocyte countTotal1-3 years: 6000 to 17,5008-13 years: 4500 to 13,500Adult:4500 to 11,000The differential is the percentage of each type of leukocyte out of thetotal. An increase in the white blood cell count is usually related to anincrease in one type and often an increase in immature neutrophils,known as bands, referred to as a “shift to the left,” generally anindication of an infectious process. Normal WBC for adults: 4,500-11,000. Acute infection: 11,000 , 30,000 indicates a severe infection. Viral infection: 4,000 and below.Because the proportion of most leukocytes is small, only an increase inneutrophils or lymphocytes is usually significant enough to result inincreased total white count with leukemia.DifferentialCell type1 yr10 yrsAdult
Neutrophils (Total)Neutrophils (bands)Neutrophils(segments)Absolute neutrophilcount 1%28%54%3%51%59%3%58%1500 to 85001800 to 800061%4.8%2.6%0.4%38%4.3%2.4%0.5%1800 to770034%4%2.7%0.5%Absolute neutrophil count (ANC) is an important measure used todetermine the degree of neuotropenia. The total ANC should be about1800 to 2000 mmm3 or higher. Risk of infection is significant if thelevel falls to 1000 and severe at 500. ANC is not calculated directly butis determined from the total white count and the percentages ofneutrophils and bands: ANC Total WBC X (% neutrophils % bands/100Using this formula, if the white blood count is 3200 with 70%neutrophils and 3% bands, the calculation would indicate that despitethe low WBC count, the patient does not have neutropenia: ANC 3000 X 73/100 2190If the white count is 5300 with 10% neutrophils and 1% bands,neutropenia is evident despite the normal WBC: ANC 5300 X 11/100 583Why is neutropenia important?The ANC falls with increased destruction of neutrophils or decreasedproduction. With leukemia, neutropenia is a direct result of both theleukemic disease process and chemotherapy used to treat it, so it is aprimary concern during therapy.Neutropenia increases the risk of both exogenous (environmental) andendogenous (GI tract, skin) infection, depending on the severity andduration. A short-lasting severe neutropenia may pose less actual riskthan a longer mild neutropenia.There are no specific symptoms related to neutropenia, so without
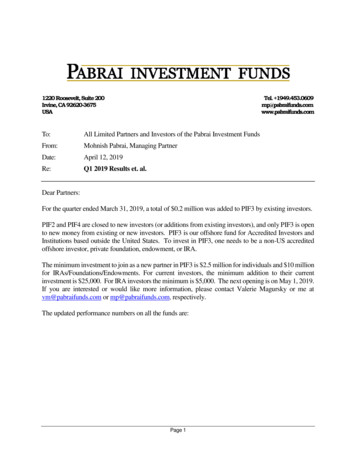
regular blood testing, it may go undiagnosed until infection occurs. Insome cases, chemotherapy is withheld or reduced until the ANC rises,but this puts the patient at increased risk from the malignancy,especially if the treatment has a potential for cure. In that case,growth factors (G-CSF or CM-CSF) may be administered to stimulateproduction. As the bone marrow recovers, neutrophil production mayincrease again.Patients who exhibit both neutropenia and fever usually have aninfection and are hospitalized for broad-spectrum intravenousantibiotic therapy. Cultures of blood, urine, and sputum and chest xray are done to try to determine the site of infection and thepathogenic agent. When cultures and sensitivities are completed, theantibiotic regimen may be modified. Patients receiving antibiotics mustbe carefully monitored for superinfection, especially fungal.Oral moniliasisMaintaining adequate nutrition is necessary as decreased proteinstores impair the immune system. Invasive procedures, such as IVs,increase risk of infection.Measures to prevent infection in those with neutropenia include: Monitor blood count daily and temperature every 4 hours,notifying physician if temperature 38 C (101 F). Prohibit visitors with illness, including cold or sore throat. Provide private room if ANC 1000. Prohibit fresh flowers as stagnant water may breed bacteria. Change water in all containers (include humidifiers) every day. Plan patient care so that patient is seen before others if possibleto avoid carrying contamination from one patient to another Eliminate fresh salads and unpeeled fresh fruit or vegetables. Provide HEPA filter mask if patient is outside of room. Ensure total body hygiene daily and wash perineal area aftereach BM.
Provide oral hygiene after meals and every 4 hours duringdaytime, avoiding lemon glycerine swabs, mouthwash, andhydrogen peroxide.Avoid plastic cannulas for peripheral IVs if ANC 500.Follow protocols for IV insertion and care, using antimicrobialsolution to cleanse skin before insertion.Thrombocytopenia is a common finding with leukemia. Normal values:Platelet 150,000 toIncreased bleeding 50,000 and increasedcount400,000 mmm3 clotting 750,000.Why is thrombocytopenia important?Like neutropenia, thrombocytopenia can result from reduced plateletproduction or increased platelet destruction caused by leukemia orchemotherapy. Additionally, severe infection, which often occurs withneutropenia, can suppress platelet production.As the platelet count drops 50,000, the ability of the blood to clotdecreases. With invasive procedures, a count 50,000 increases riskof bleeding, but otherwise, risk is not usually significant until countdrops to 20,000, at which point common indications include: Petechiae. Nasal bleeding. Gingival bleeding. Excessive menstrual flow.Severe risk of bleeding occurs with a platelet count 5000: CNS hemorrhage. GI hemorrhage.A bone marrow biopsy is often used to determine the cause of plateletdeficiency.
Reduced platelet production (which can occur with acuteleukemias and chemotherapy): Platelet transfusions mayincrease platelet count. Increased platelet destruction (which can occur with CLL):The bone marrow shows increased megakaryocytes (cells fromwhich platelets develop) and normal or increased production ofplatelets as the body attempts to compensate. If platelets arebeing destroyed, platelet transfusions provide little relief as thetransfused platelets are also destroyed. In this case, treatmentis usually similar to that for idiopathic thrombocytopeniapurpura: Immunosuppressive agents, such as prednisone,cyclophosphamide, azathioprine, and dexamethasone.Standard treatment protocolThe protocol for treatment varies depending onthe type of leukemia. Generally, a combinationof drugs is given as this approach is moreeffective than monotherapy. There are generally3 stages to chemotherapy: Induction Consolidation MaintenanceInductionPatients are usually hospitalized for 4 to 6 weeksduring initial treatment. The purpose is to induceremission with bone marrow clear of disease and blood
counts within normal limit. During this time, chemotherapy eradicatesboth leukemic cells and normal myeloid cells, so the person becomesseverely neutropenic, anemic, and thrombocytopenic, putting patientsat risk for severe infections and bleeding. Patients may developbacterial, fungal, and viral infections, and severe mucositis, whichcauses diarrhea and impairs nutritional absorption.Supportive care includes administering blood products, such as packedred blood cells and platelets, providing antibiotics to treat infections,Granulocytic growth factors (G-CSF or GM-CSF) may shorten theperiod of neutropenia by stimulating the bone marrow to increaseproduction of leukocytes.After the patient has recovered from the effects ofinduction, consolidation treatment is provided over4 to 8 months, often with the samechemotherapeutic agents used during induction but at lower dosagesin order to kill any remaining malignant cells. Intrathecalchemotherapy may be administered concurrently as a prophylaxis toprevent CNS involvement. This treatment may be done on anoutpatient basis with multipl
Leukemia is a group of malignant disorders affecting the blood and blood-forming tissues in the bone marrow, lymphatic system, and spleen. The word leukemia literally means “white blood” because it is a neoplastic proliferation of one type of blood cell, typically a leukocyte or white blood cell. Leukocytosis, an increased white blood cell count,File Size: 534KBPage Count: 32