Transcription
NOTE: The electronic version of this document or form is the latest and only acceptable version. You are responsible to ensure anyprinting of this document is identical to the e-version.SKIN CARE: PRESSURE INJURY PREVENTIONClinical ProtocolApproved: March 2020Next Review: March 2023Clinical Area: All inpatient clinical and emergency department areasPopulation Covered: All Adult and Pediatric Inpatients and Emergency Department patientsCampus:Ballard, Cherry Hill, Edmonds, First Hill,Issaquah, Mill Creek, RedmondImplementation Date: January 2002Related Procedures, Protocols, and Job Aids:Camera Photography, Video and Audio RecordingSacral Dressing Application for Pressure Ulcer PreventionVacuum Assisted Wound Closure (VAC) Therapy ManagementWound Management: ComplexUsing Digital Photography for Patient Care (Haiku Photo Capture)Perineal Skin Care/Diaper Dermatitis Management Guideline for Neonates and Diapered ChildrenSkin Injury Prevention Related to Respiratory TherapyGo directly to:Patient AssessmentBasic Skin Care / Pressure Ulcer BundleSkin and Wound TreatmentBraden ScoringDefinitionsMoisture Associated Skin Damage (MASD)Nail CareSkin TearsPressure Injury Debrief and HandoffPurposeTo provide guidelines for assessment, prevention, and interventions of common skin-related issues.Policy StatementNone.LIP Order RequirementElements of this protocol require a licensed independent practitioner’s (LIP) order.Responsible PersonsRN, LIP, Nursing Assistants (NA-C), Wound Ostomy Nurse (WON)Clinical Protocol: SKIN CARE: PRESSURE INJURY PREVENTION 2020 Swedish Health ServicesPage 1 of 9
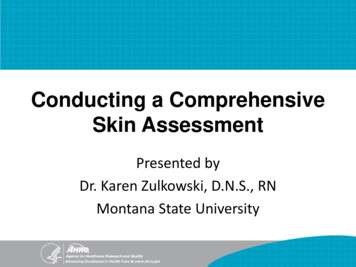
Prerequisite InformationIdentification of the patient who is at risk for the development of pressure injury is essential to the success of anyskin care program. Risk factors including immobility, pressure, friction, shear, nutritional deficit, sensory deficit,inactivity, dehydration, edema, incontinence, excess moisture, diabetes, vascular disease. 6. IIAThe Braden Scale for predicting pressure injury risk is a validated tool that allows nurses to reliably score adultpatients level of risk for developing pressure injuries. 1. IVAThe Braden QD Scale is a validated tool that allows nurses to reliably score pediatric patients level of risk fordeveloping pressure injuries.The incidence of pressure ulcers and their complications can be significantly reduced with optimal nursingintervention, combined with patient and caregiver participation and education. 6. IIAPressure injuries generally develop over bony prominences and are an ischemic response to sustained pressureand/or damaging forces (shear, friction, moisture). This ischemic response can result in soft tissue death. 6. IIAPROCEDURE or PROTOCOL Requires an LIP orderResponsiblePersonStepsPATIENT ASSESSMENTRNBony prominence sitesInitial skin assessmentA skin assessment is performed and documented within 12 hours of admission on all patients,as well as prior to any elective procedure. Assessment head to toe and front to back skinassessment includes:Clinical Protocol: SKIN CARE: PRESSURE INJURY PREVENTION 2020 Swedish Health ServicesPage 2 of 9
1.Examination under skin folds, under all potential pressure points, and under anydevices, unless contraindicated due to physiologic instability.2.The RN completes the admission screening, the Braden Scale (adults) and Braden QD(pediatrics), and the skin/wound assessment in the electronic medical record (EMR).NOTE: For pediatric and neonatal patients, review the visual aids in the Skin InjuryPrevention Related to Respiratory Therapy policy.NOTE: A pressure injury documented within 24 hours of admission is consideredpresent on admission (POA). 2. National GuidelinesRN, LIP3.to beIf the patient is found to be at risk for developing a pressure injury, the Pressure InjuryPrevention Bundle is initiated. Criteria for initiation of the bundle include: Braden scale of 18 or less (adults)Two of the sub-scores of the Braden have scores of 2 or less (adults)Braden QD Scale of 13 or greater (pediatrics)The Pressure Injury Bundle includes five elements: 1) Skin prophylaxis, 2) Pressureredistribution, 3) Positioning, 4) Moisture management, and 5) Nutrition support.4.If the patient is admitted with a dressing, it should be removed by the RN to assess theskin unless contraindicated. Examples of possible exceptions include: Stabilizing bracesNegative pressure therapy dressings (VAC)NOTE: RN should clarify exceptions with the LIP. If a VAC dressing has beenin place longer than outlined in the Vacuum Assisted Wound Closure (VAC)Therapy Management policy for frequency of dressing changes, the LIP shouldbe notified. 5.RN, LIP, WONReview orders for surgical wounds or patients post procedure, as these may havebeen placed by the LIP post procedure.Each alteration in skin integrity (pressure-related and non-pressure-related) must have anew LDA added in the EMR. At a minimum, the RN is expected to document thelocation, measurements and color of the wound bed, and actions or interventions taken.Each dressing change is dated and timed on the dressing and documented in theflowsheet.Pressure Injury assessmentIf the patient has a pressure injury present on admission (POA) or develops a hospitalacquired pressure injury (HAPI):See addendum, Present on Admission: Pressure Ulcer Documentation Process.1.2.Notify LIP of pressure injury (POA or HAPI). The LIP is responsible for documentingthe POA pressure injury in the admission history and physical (H&P). 2. National GuidelinesAt a minimum, the RN is expected to document the location, measurements and colorof the wound bed, and actions or interventions taken upon discovery of the pressureinjury. 6. IIAClinical Protocol: SKIN CARE: PRESSURE INJURY PREVENTION 2020 Swedish Health ServicesPage 3 of 9
3.4.5.6.7.The bedside nurse may identify and document Stage 1 pressure injuries. Remove thepressure source from the area (i.e., turn patient or reposition). Wait 30 minutes andthen reassess the wound by testing for blanchability. 6. IIAAside from Stage 1 pressure injuries, the pressure injury is staged by a WON and thoseRNs who have completed pressure injury staging education modules with documentedcompetency.A wound care consult is needed for any injury other than a Stage 1.Photograph the injury and placing the picture into the EMR. See Using DigitalPhotography for Patient Care (Haiku Photo Capture).If the pressure injury is hospital acquired: the nurse is to initiate the Pressure InjuryDebrief and Handoff. This form is to be completed, a copy is to be provided to the unitmanager, and the original is to accompany the patient should the patient transfer toanother unit. The checklist should be completed, which includes initiating an eQVRand obtaining a wound care consult.Ongoing skin assessmentRNOngoing assessment is completed by the RN a minimum of every shift and documented in theassessment flow sheet of the EMR. The documentation includes any alteration in skin integrity,new risk factors, and actions taken. The pressure injury prevention bundle is initiated if thepatient is found to be at risk: Braden scale of 18 or less (adults)Two of the sub-scores of the Braden have scores of 2 or less (adults)Braden QD Scale of 13 or greater (pediatrics)BASIC SKIN CARE / PRESSURE INJURY BUNDLERN, LIPPatients at SMC will receive basic skin care. Elements of this include:Skin Prophylaxis1.2.3.Consider the use of certain devices for prevention of pressure injury. These devicesinclude a silicone bordered sacral dressing (see Sacral Dressing Application forPressure Ulcer Prevention). 4. IVBOff-loading cushions for chairs. 4. IVBUse of pillows and protective heel boots to float heels or other areas. Use of thesedevices is particularly important in patients who are at high risk for pressure injury.4. IVBNOTE: The use of such devices does NOT replace regular skin inspection andfrequent repositioning. 4. IVBPressure redistribution1.2.3.4.5.Most adult and bedded pediatric patients at SMC are on a low air loss/pressureredistribution surface. Some patients will need alternative surfaces based on specialneeds (i.e. bariatric surface). 4. IVBUse single-layer breathable pads. There should be no more than 3 layers of pads and/orlinens between the patient’s skin and the air mattress.Protect the patient from lying on lines, tubes and wrinkled linen.4. IVBPosition to avoid allowing the body tissue to be compressed or under pressure from bedrails, arms of chairs, etc. 4. IVBRegardless of Braden Score or Braden QD score, all efforts should be made to reducepressure over bony prominences and under medical devices.4. IVBNOTE: The turn assist feature on beds does not offload the sacral pressure. Thisfeature should primarily be used during the physical act of turning the patient tohelp the staff member with the turn. 4. IVBClinical Protocol: SKIN CARE: PRESSURE INJURY PREVENTION 2020 Swedish Health ServicesPage 4 of 9
NOTE: Head of Bed greater than 45 degrees should be avoided for extendedperiods of time to minimize sacral pressure. As warranted by patient conditionand LIP orders, alternatives to this are HOB at 30 degrees and ReverseTrendelenburg. 4. IVBHead of bed, bassinet, crib for pediatrics is patient dependent. If they are on theventilator-associated prevention protocol, review Ventilator-AssociatedPneumonia (VAP) Bundle: Pediatric.NOTE: Specialty beds, including air fluidized beds do not eliminate or minimizethe frequency of the turning and repositioning requirement.Positioning (EMR: Keep Turning/Repositioning)1.RN, LIP2.RN, LIPAll patients, regardless of presumed ability, may need assistance withpositioning.6. IIAA turn schedule is initiated if the patient has a total Braden score of 18 or less, or a subscore of 2 or less in the mobility, sensory, and/or activity categories for adult patientsand a Braden QD of 13 or greater for pediatric patients. Turn every 2 hours, howeverpatients may be turned more frequently based upon individual need. 6. IIANOTE: All actual positions must be documented if the patient is on a turnschedule.For adult patients, if the Braden score is 18 or less and the patient is able to turn themselves,their actual position will need to be documented every 2 hours. If the patient does not turnthemselves every 2 hours, the RN should prompt the patient to turn. 6. IIANOTE: If an adult patient refuses a turn and has a Braden score of 18 or less, therefusal should be documented. Notify the LIP for ongoing refusal to turn.4.When a patient is in the chair, shift the patient’s weight every two hours.4. IVBMoisture management1.2.Bathing: Use disposable washcloths, cleansing foam and pre-moistened wipes forbathing. The use of pH (hydrogen ion concentration) neutral soap is encouraged. Useof wash basins is discouraged due to infection control.Incontinence hygiene:a.b.c.d.e.Patients who are incontinent should receive prompt care to avoid skinbreakdown. This includes, but is not limited to toileting schedules andmoisture barrier products.Do not use adult briefs unless the adult patient is out of bed.While in bed, one incontinence pad is preferred under the patient.Do not leave a patient on a bedpan for greater than 10-15 minutes.Use moisture protection devices, creams, ointments to keep skin folds dry,change as needed.Nutrition1.2.For adults with a Braden Nutrition subscore of 2 or less, a nutrition consult should beplaced in the EMR.3. IIIA Pediatric patients receive a nutrition review, but if the nurse isconcerned, they may place a nutrition consult.Consider lab values that may indicate nutritional risk (i.e. Albumin, Prealbumin,Hemoglobin A1C, and Transferrin). Patients with disease processes which may causenutritional compromise should be considered at risk also (i.e. Renal Disease, Cancer,Crohn’s disease, etc.).3. IIIAClinical Protocol: SKIN CARE: PRESSURE INJURY PREVENTION 2020 Swedish Health ServicesPage 5 of 9
2.3.A patient who is NPO is not automatically at risk. However, consider recent nutritionaldeficit (lengthy NPO status, poor caloric intake, and/or poor glucose control).3. IIIAThe RN is responsible for verifying the nutrition consult and maintaining or initiatingthe nutritional interventions established by the dietary department.SKIN AND WOUND TREATMENTRN, WON1.Nursing interventions: When a wound is present and the WON is not available toconsult, the RN should utilize the Wound Care: Complex policy.NOTE: Ultimately, the dressing selection is less important in the healing of apressure injury than aggressive pressure relief to the injured area.2.3.RN, LIPCleanse or irrigate all wounds with normal saline prior to the application of dressings.The pressure ulcer bundle is instrumental in both prevention and treatment of allpressure injuries.Moisture-Associated Skin Damage (MASD) (This includes incontinence-associateddermatitis [IAD]) 7. IVA1.2.3.Assess the cause of MASD and discuss interventions with the LIP.Assess for signs/symptoms of yeast infection, report to LIP if applicable.Skin care once a shift and PRN due to stooling:a. b.Clean with foam or spray cleanser and pat dry.If yeast is present (appears bright red and may have red pustules), applyantifungal powder or cream per order, obtained through the Pharmacy).c.d. e.Apply moisture barrier products liberally to all affected areas.Notify the wound care nurse if there is no improvement after 48 hours.Consider a fecal management system if applicable.Clinical Protocol: SKIN CARE: PRESSURE INJURY PREVENTION 2020 Swedish Health ServicesPage 6 of 9
Skin Tears1.2.3.4.5.6.7.Cleanse the area with normal saline.If the loose skin flap is still hanging, then bring it together with a cotton tip applicatorto cover the exposed area.Apply a non-adhesive contact dressing.Cover with dry gauze and Kerlix (roll gauze), secure with a tubular dressing. If theskin tear is in an area where tubular dressings are not feasible, use dry gauze and securewith tape. Minimize the amount of tape directly on the skin.Use No Sting Barrier film around the peri-wound areas to reduce risk of maceration,and also where tape is required to secure the dressing.Consult wound care nurse for large or extensive skin tears.Consult the LIP if localized signs of infection or inflammation are noted.DefinitionsBlanchable – skin erythema that loses all redness when pressed and is due to vascular dilation.Non-blanchable erythema indicates the presence of red blood cells outside of the blood vessels(extravasation).Forms Pressure Injury Debrief & Handoff FormSupplemental InformationNone.Regulatory Requirement1. Centers for Medicare and Medicaid Services, Department of Health and Human Services. (2015). Conditionof participation: Patient's rights. 42 C.F.R. § 482.13(c)(1).2. DNV GL-Healthcare USA, Inc. (2014). IC.1.SR.1. NIAHO accreditation requirements: Interpretiveguidelines & surveyor guidance (version 11). Milford, OH: DNV GL-Healthcare USA, Inc.References1. Bergstrom, N., & Braden, B. (n.d.). Braden Scale for Predicting Pressure Sore Risk. Retrieved3, 2017, from anuary2. Centers for Medicare & Medicaid Services. (2016). OASIS-C2 guidance manual-effective 1-1-2017. Chapter3: F-1. Retrieved January 3, 2017, from Downloads/OASIS-C2- Guidance-Manual- 6-29-16.pdf3. Doley, J. (2010). Nutrition management of pressure ulcers. Nutrition in Clinical Practice, 25, 50–60.4. McInnes, E., et al. (2011). Support surfaces for pressure ulcer prevention. Cochrane Database ofSystematic Reviews, 2011(4), CD001735.5. Sernekos, L. A. (2013). Nutritional treatment of pressure ulcers: What is the evidence? Journal of theAmerican Association of Nurse Practitioners, 25, 281–288. Accessed January 17, 2017 via the Web 6924.12025/pdf6. Wound, Ostomy and Continence Nurses Society. (2016). Wound, Ostomy and Continence NursesSociety’s guidance on OASIS-C2 integumentary items: Best practice for clinicians. Mt. Laurel,Pierce, B.NJ:Clinical Protocol: SKIN CARE: PRESSURE INJURY PREVENTION 2020 Swedish Health ServicesPage 7 of 9
7. Zulkowski, K. (2012). Diagnosing and treating moisture-associated skin damage. Advances in Skin & WoundCare, 25, 231–2368. Curley, MAQ, Hasbani, NR, Quigley, SM, Stellar, JJ, Pasek, TA, Shelley, SS, Kulik, LA, Chamblee, TB,Dilloway, MA, Caillouette, CN, McCabe, MA, Wypij, D. Predicting pressure injury risk in pediatric patients:the Braden QD Scale. J Pediatr 2018;192:189-95.9. Chamblee, TB, Pasek, TA, Caillouette, CN, Stellar, JJ, Quigley, SM, Curley, MAQ. How to Predict PediatricPressure Injury Risk with the Braden QD Scale. Am J Nurs. 2018 Nov;118(11):34-43.AddendaAddendum 1- Pressure Ulcer Staging, Example 1Addendum 2- Braden ScaleAddendum 3- Pressure Ulcer Staging, Example 2How to Order a Specialty Bed / Bariatric Bed and Rental ProductsSpecifications for Specialty BedsNail CarePediatric Braden QD ScalePressure Injury Debrief and HandoffSpecialty Bed Order Algorithm (Edmonds only)Skin Care for End of Life CareSTAKEHOLDERSAuthor/ContactBirgit Petersen, BSN, RN, CWCN, Skin NQL LeaderNicole Roehrig, MSN, RN, CPN. Pediatric Clinical Nurse SpecialistExpert ConsultantsHAPI Steering Team (March 2017)Wound Healing CenterPediatric Quality and Safety Committee (Dec 2019)SponsorMargo Bykonen, MSN, Chief Nursing Officer01230201.doc(rev.03/12/20)Clinical Protocol: SKIN CARE: PRESSURE INJURY PREVENTION 2020 Swedish Health ServicesPage 8 of 9
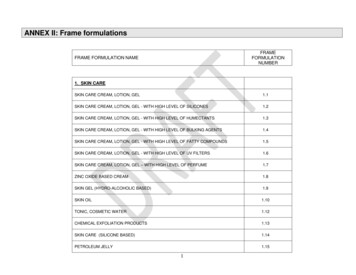
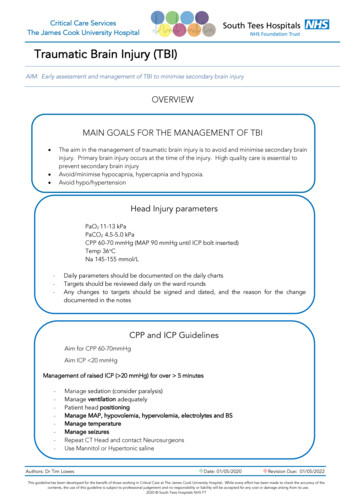
Addendum 1Pressure Ulcer Staging, Example 1Stage 1 Pressure Injury: Non-blanchable erythema of intact skinIntact skin with a localized area of non-blanchable erythema, which may appear differently in darkly pigmentedskin. Presence of blanchable erythema or changes in sensation, temperature, or firmness may precede visualchanges. Color changes do not include purple or maroon discoloration; these may indicate deep tissue pressureinjury.Stage 2 Pressure Injury: Partial-thickness skin loss with exposed dermisPartial-thickness loss of skin with exposed dermis. The wound bed is viable, pink or red, moist, and may alsopresent as an intact or ruptured serum-filled blister. Adipose (fat) is not visible and deeper tissues are not visible.Granulation tissue, slough and eschar are not present. These injuries commonly result from adverse microclimateand shear in the skin over the pelvis and shear in the heel. This stage should not be used to describe moistureassociated skin damage (MASD) including incontinence associated dermatitis (IAD), intertriginous dermatitis(ITD), medical adhesive related skin injury (MARSI), or traumatic wounds (skin tears, burns, abrasions).Clinical Protocol: SKIN CARE: PRESSURE INJURY PREVENTION 2020 Swedish Health ServicesAddendum
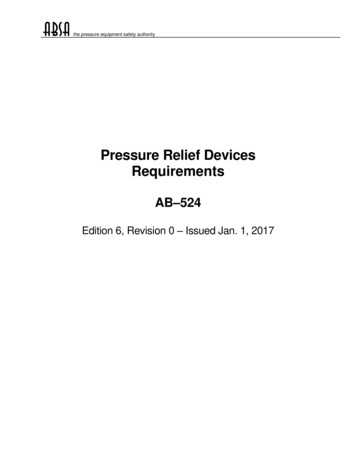
Stage 3 Pressure Injury: Full-thickness skin lossFull-thickness loss of skin, in which adipose (fat) is visible in the ulcer and granulation tissue and epibole (rolledwound edges) are often present. Slough and/or eschar may be visible. The depth of tissue damage varies byanatomical location; areas of significant adiposity can develop deep wounds. Undermining and tunneling mayoccur. Fascia, muscle, tendon, ligament, cartilage and/or bone are not exposed. If slough or eschar obscures theextent of tissue loss this is an Unstageable Pressure Injury.Stage 4 Pressure Injury: Full-thickness skin and tissue lossFull-thickness skin and tissue loss with exposed or directly palpable fascia, muscle, tendon, ligament, cartilage orbone in the ulcer. Slough and/or eschar may be visible. Epibole (rolled edges), undermining and/or tunnelingoften occur. Depth varies by anatomical location. If slough or eschar obscures the extent of tissue loss this is anUnstageable Pressure Injury.Clinical Protocol: SKIN CARE: PRESSURE INJURY PREVENTION 2020 Swedish Health ServicesAddendum
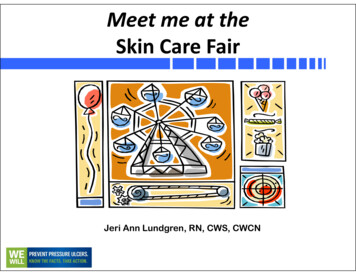
Unstageable Pressure Injury: Obscured full-thickness skin and tissue lossFull-thickness skin and tissue loss in which the extent of tissue damage within the ulcer cannot be confirmedbecause it is obscured by slough or eschar. If slough or eschar is removed, a Stage 3 or Stage 4 pressure injurywill be revealed. Stable eschar (i.e. dry, adherent, intact without erythema or fluctuance) on the heel or ischemiclimb should not be softened or removed.Deep Tissue Pressure Injury: Persistent non-blanchable deep red, maroon or purple discolorationIntact or non-intact skin with localized area of persistent non-blanchable deep red, maroon, purple discoloration orepidermal separation revealing a dark wound bed or blood filled blister. Pain and temperature change oftenprecede skin color changes. Discoloration may appear differently in darkly pigmented skin. This injury resultsfrom intense and/or prolonged pressure and shear forces at the bone-muscle interface. The wound may evolverapidly to reveal the actual extent of tissue injury, or may resolve without tissue loss. If necrotic tissue,subcutaneous tissue, granulation tissue, fascia, muscle or other underlying structures are visible, this indicates afull thickness pressure injury (Unstageable, Stage 3 or Stage 4). Do not use DTPI to describe vascular, traumatic,neuropathic, or dermatologic conditionClinical Protocol: SKIN CARE: PRESSURE INJURY PREVENTION 2020 Swedish Health ServicesAddendum
Addendum 2 Braden ScaleClinical Protocol: SKIN CARE: SKIN CARE: PRESSURE INJURY PREVENTION 2020 Swedish Health ServicesAddendum.
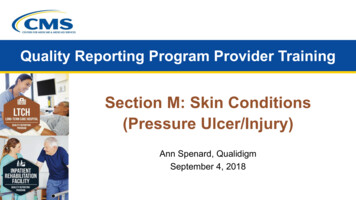
Addendum 3Pressure Injury Staging, Example 2Deep TissueInjuryUnstageableStage 1Stage 2Stage 3Stage 4Goal:ProtectionGoal:Protection, moisthealing andabsorptionGoal:Protection, fill depthand absorptionGoal:Protection, fill depth andabsorptionGoal:Protect frompressure, friction,shear and moistureGoal:Protection, fill Depth anddebridement s:Apply Skin Sealantaround the wound every24 hoursApply Skin Sealantaround the woundevery 24 hours If the wound issuperficial, fill withHydrofiber and coverwith foam every 3days and PRN If the wound is deeper,fill with salinemoistened gauze andcover with ABD padchange daily and prnfor drainage Cover the woundwith siliconeborder dressingevery 3 days orleave open to airfor observationApply Skin Sealantto the wound every24 hoursApply Skin Sealantaround the woundevery 24 hoursOR If the wound hasdrainage, coverwith a foamdressing andchange every 3days and PRN Apply a barriercream threetimes daily andPRNApply Skin Sealantaround the woundevery 24 hourSee Stage 2 If the wound isdeeper, fill withHydrofiber thencover with foamdressing everythree days andPRN(any wound where the baseis not visible)Apply Skin Sealant aroundthe wound every 24 hours See Stage 3 Exception: for dryeschar, Cover only withdry dressing and changedaily.April 2017Clinical Protocol: SKIN CARE: SKIN CARE: PRESSURE INJURY PREVENTION 2020 Swedish Health ServicesAddendum.
BASIC SKIN CARE / PRESSURE INJURY BUNDLE Patients at SMC will receive basic skin care. Elements of this include: Skin Prophylaxis 1. Consider the use of certain devices for prevention of pressure injury. These devices include a silicone bordered sacral dressing (see Sacral Dressi