Transcription
Nutrition cover v4.pdf112/14/184:01 PMPROCEEDINGSAdvancing Global Nutritionfor Adolescent and Family Health:Innovations in Research and TrainingMohammed Bin Rashid Academic Medical CenterBuilding 14 PO Box 505276 Dubai Healthcare City Dubai United Arab EmiratesTel. 971 4 422 1740 Fax 971 4 422 5814 http://ghd-dubai.hms.harvard.eduIN COLLABORATION WITHISBN-10: 1-944302-12-3ISBN-13: ORKSHOP PROCEEDINGS
Nutrition cover v4.pdf212/14/184:01 PMCopyright 2018 by the Harvard Medical School Center for Global Health Delivery–Dubai.All rights reserved.Publications of the Harvard Medical School Center for Global Health Delivery–Dubai areavailable at www.ghd-dubai.hms.harvard.edu. Printed publications can also be requestedat ghd.dubai@hms.harvard.edu.Any opinion, findings, conclusions, or recommendations expressed in this publication donot necessarily reflect the views of Harvard Medical School. Harvard Medical School orits licensors at all times own and retain all right, title, and interest in and to theseProceedings (hereafter referred to as “the publication”) including all intellectual propertyrights therein and thereto. You may use and copy the publication, or portions of thepublication, provided that you reproduce all copyright notices, claims, or reservation ofrights appearing in the publication, as delivered to you, on all copies made pursuant tothis sentence.By using this publication, you acknowledge that (i) Authors are not guaranteeing thecompleteness or accuracy of the information contained herein, (ii) the publication doesnot represent nor comprise all of the data or other information that may be relevant toyou, (iii) portions of the publication may be outdated and may have been superseded bysubsequent changes in applicable law, regulation, or conditions affecting the treatmentof tuberculosis or the delivery of health care generally, and (iv) the Authors do not haveany duty to update the publication or, if updated, to provide further updated versions ofthe publication.To the maximum extent permitted under applicable laws, none of the Authors are liable,under any circumstance or under any theory of law, tort, contract, strict liability orotherwise, for any direct, indirect, special, incidental, consequential, exemplary orpunitive damages, or any other injury and/ or damage (actual or perceived), including,without limitation, damages based on errors, omissions, or reliance upon, use, oroperation of any ideas, instructions, procedures, products, or methods contained in thematerial included in the publication.By using the publication, you acknowledge and agree to the terms of this notice. Theauthors would like to thank Annie Smidt at Durable Creative (www.durablecreative.com)for design support in the production of this resource.International Standard Book NumberISBN-10: 1-944302-12-3ISBN-13: 978-1-944302-12-2Suggested citation: Advancing Global Nutrition for Adolescent and Family Health:Innovations in Research and Training. Proceedings of the Harvard Medical School Centerfor Global Health Delivery–Dubai. 2018, Dubai, United Arab Emirates.
Advancing Global Nutrition for Adolescentand Family Health:Innovations in Research and TrainingWorkshop ProceedingsRapporteur:Anna NicholsonPlanning Committee:Wafaie FawziChelsey CanavanSalmaan KeshavjeeHarvard Medical School Center for Global Health Delivery-DubaiHarvard Medical SchoolDepartment of Global Health and PopulationHarvard T.H. Chan School of Public HealthMohammed Bin Rashid University (MBRU)Dubai Healthcare City, Dubai, United Arab EmiratesFebruary 16-17, 2018
Advancing Global Nutrition for Adolescent and Family Health: Innovations in Research and TrainingContents1 Introduction71.1 Organization of the workshop81.2 Organization of the workshop proceedings82 Child and adolescent health and nutrition interventions92.1 Anemia interventions to improve adolescent health92.1.1 Introduction to adolescent nutrition92.1.2 Anemia in adolescents102.1.3 WHO recommendations on iron supplementation132.1.4 WIFS intervention in India142.1.5 Discussion152.2 Adolescent anemia working group proposals162.3 Integrated child health and nutrition interventions172.3.1 Risks associated with poor early child development outcomes172.3.2 Research opportunities for the ARISE network192.3.3 Integrating care, stimulation/early learning, and nutritioninterventions192.3.6 Early child development scale up trial in Pakistan212.3.7 Overview of integrated nutrition and stimulation interventions222.3.8 Discussion232.4 Mental health and child development working group proposals3 Adolescent sexual and reproductive health interventions23253.1 Interventions to improve adolescent sexual and reproductive health253.1.1 Child marriage as an outcome of adolescent reproductive andsexual health263.1.2 Interventions to prevent child marriage283.1.3 Lessons from past interventions to prevent child marriage283.1.4 Developing proposals for interventions293.1.5 Policy levers293.1.6 Discussion303.2 Creating demand for youth-friendly sexual and reproductivehealth interventions313.2.1 Risky sexual behaviors among adolescents in Ghana313.2.2 Teenage pregnancy and child marriage in Ghana333.2.3 Nutritional status of adolescents in Ghana33
3.2.4 Policy framework343.2.5 Proposed intervention to create demand for youth-friendly service353.2.6 Discussion363.3 Sexual and reproductive health working group proposals4 Urban food systems and food production interventions36394.1 Impact of urban food systems on health and nutrition394.1.1 Urbanization and the obesogenic environment394.1.2 Pesticides in food systems404.1.3 Research background and proposals414.1.4 Ongoing work in India424.1.5 Discussion434.2 Sustainable urban diets to improve health454.2.1 Food environments464.2.3 Food systems and environmental impacts484.2.4 Urban diet study494.2.5 Discussion504.3 Homestead food production interventions504.3.1 Nutrition-sensitive interventions and programs504.3.2 Theory of change for homestead food production524.3.3 Nutrition-sensitive homestead food production project in Tanzania534.3.4 Impact assessment of nutrition-sensitive interventions544.3.5 Optimal mix of interventions544.3.6 Discussion554.4 Schools and urban food systems working group proposals554.5 Homestead food production working group proposals575 Health and demographic surveillance systems5.1 Longitudinal health and demographic surveillance systems59595.1.1 Health and demographic surveillance system in Kersa andHarrar, Ethiopia595.1.2 ARISE study in Kersa and Harar605.2 Longitudinal demographic surveillance systems workinggroup proposals6 Synthesis and ways forward6.1 Short-term interventions factoring in limited scope and expense6264646.1.1 Market basket audit646.1.2 School-based surveys of food ecosystem and fruit andvegetable intake64
Advancing Global Nutrition for Adolescent and Family Health: Innovations in Research and Training6.1.3 Workshops with adolescents about approaching sensitive topics6.2 Larger interventions requiring more time and resources64646.2.1 Integrated interventions to delay marriage, delay pregnancy,and improve nutrition646.2.2 Integrated two-generational intervention646.2.3 Interventions around anemia and/or undernutritionamong adolescents656.2.4 Policy intervention to target fruit and vegetable consumption656.2.5 Smaller studies to inform school-based interventions656.3 Opportunities for writing and disseminationAppendices6567Appendix A. Workshop agenda67Appendix B. List of workshop participants69
AbbreviationsAAPH: Africa Academy for Public HealthARISE: Africa Research, Implementation Science, and EducationASRH: Adolescent Sexual and Reproductive HealthBMI: Body Mass IndexCHAMPS: Child Health and Mortality Prevention SurveillanceECD: Early Childhood DevelopmentHDSS: Health and Demographic Surveillance SystemsLHW: Lady Health WorkerLMIC: Low- or Middle-income CountryMUAC: Mid-Upper Arm CircumferencePOP: Persistent Organic PollutantsSHEP: School Health Education ProgramWASH: Water, Sanitation and Hygiene
Advancing Global Nutrition for Adolescent and Family Health: Innovations in Research and Training1 IntroductionOn February 16th and 17th 2018, a groupof international experts from a range ofdisciplines convened at the Harvard MedicalSchool Center for Global Health Delivery–Dubai for the workshop Advancing GlobalNutrition for Adolescent and Family Health:Innovations in Research and Training. Themeeting was organized by the Harvard T.H.Chan School of Public Health’s Departmentof Global Health and Population, with supportfrom the Center for Global Health Delivery(see Box 11 for a description of the Center’sactivities). Wafaie Fawzi of Harvard T.H.Chan School of Public Health (U.S.) openedthe workshop by welcoming participantsand thanking the Center for hosting themeeting. Adolescent health is addressed fromvarious vantage points, he explained, suchas nutrition, sexual and reproductive health,chronic diseases, mental health, and childdevelopment. A key aim of the meeting wasto collaborate toward developing concreteproposals for interventions and actions bydrawing upon on the experience and expertiseof the assembled participants.In 2014, the Africa Research, ImplementationScience, and Education (ARISE) Network waslaunched with the support of the Africa HealthPartnership at the school, which promotescollaborations with academic and researchinstitutions throughout Sub-Saharan Africa,and the Harvard-affiliated Africa Academyfor Public Health (AAPH), which is a regionalhub for health-related research, trainingand education, and knowledge translation.Harvard T.H. Chan School of Public Health andAAPH have been working together for over40 years to advance public health prioritiesin Sub-Saharan Africa. ARISE is a network forcollaborative education and research activitiesin Africa that brings together colleagues andinstitutions from seven countries in Africa toadvance training and research capacity in theregion. The ARISE Network has collected dataon all those dimensions of adolescent healththrough a uniform survey conducted in ninesites in Africa and also worked with partnersto conduct the survey in India. The workshopbrought together ARISE Network membersand others working to advance nutrition foradolescent and family health in the ARISEregion and beyond.7
Box 1. Harvard Medical School Center for Global Health Delivery - DubaiA brief overview of the work carried out by the Harvard Medical School Center forGlobal Health Delivery–Dubai was provided by Salmaan Keshavjee, the directorof the Center and an associate professor of global health and social medicine atHarvard Medical School. The Center was created with the aim of addressing a criticalgap in translating laboratory and clinical scientific advances into knowledge amongcommunities where people live and work. An ongoing challenge in global health isfinding ways to bring the fruits of modern medicine to bear on people’s lives in waysthat have meaningful, population-level impact, he said. The Center was created to buildon Harvard Medical School’s mission, to create and nurture a diverse community of thebest people to alleviate human suffering. The Center’s work focuses on delivering carefor health conditions with burdens that are compounding rapidly worldwide, but whichare not receiving the urgent attention from the global health community that they soincreasingly warrant. These areas of focus include diabetes, obesity, cardiovasculardisease, mental health, access to surgical care, and infectious diseases includingtuberculosis and hepatitis C virus. The Center’s guiding rubric is to address maternaland child health within each of these areas of focus. The Center brings togetherexperts from around the world for meetings and workshops, with outputs ranging fromproceedings to policy briefs that are shaping policy and driving action far and wide, saidKeshavjee.Source: Keshavjee, Presentation at Advancing Global Nutrition for Adolescent and FamilyHealth: Innovations in Research and Training 2018.1.1 ORGANIZATION OF THEWORKSHOP1.2 ORGANIZATION OF THEWORKSHOP PROCEEDINGSThe two-day workshop featured eightpresentations related to advancing globalnutrition for adolescent and family health.Topics included anemia, adolescent sexualand reproductive health, early childhooddevelopment, urban food systems and diets,homestead and school-based food productioninterventions, and health and demographicsurveillance systems. Smaller working groupsessions were interspersed throughout theworkshop, in which participants generatedproposals for intervening in each of those sixfocus areas. The workshop concluded with asynthesis and group discussion.The proceedings of the workshop arestructured into six chapters. The secondchapter summarizes the presentationsand working group discussions focused onchild and adolescent health and nutrition.Adolescent sexual and reproductive healthinterventions, presentations, and workinggroup discussions are presented in thethird chapter. The fourth chapter describespresentations and discussions on urban foodsystems and food production interventions,while the fifth chapter covers health anddemographic surveillance systems. The sixthchapter provides a summary of the final groupsynthesis and discussion of ways forwardto develop interventions and to publish anddisseminate research.8
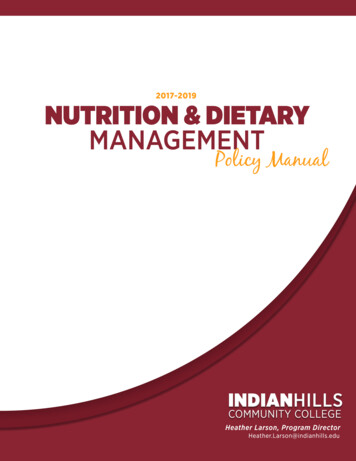
Advancing Global Nutrition for Adolescent and Family Health: Innovations in Research and Training2 Child and adolescent health andnutrition interventions2.1 ANEMIA INTERVENTIONS TOIMPROVE ADOLESCENT HEALTHIn his presentation, Chris Sudfeld, AssistantProfessor at the Harvard T.H. Chan Schoolof Public Health (U.S.), provided a briefintroduction to key concepts in adolescentnutrition before focusing on the prevalenceand treatment of anemia in adolescents.2.1.1 Introduction to adolescentnutritionSudfeld opened by presenting Figure 21, whichdepicts the life cycle approach to nutrition. Itillustrates the effects across the cycle fromlow birth weight to adult noncommunicablediseases. He noted that there has beenmuch research focused on the first fiveyears of life—that is, babies with low birthweight and associated risks of mortality andimpaired mental health—as well as in thepregnancy space and the impact on childmortality. However, he drew attention to thecomponent of the cycle related to adolescentnutrition and its effects on adolescents whobecome pregnant, including the impacton cognitive development. Iron deficiencyis also associated with fatigue and loss ofproductivity, he added.Figure 1. Nutrition through the life cycleNote: LBW low birth weightSource: Sudfeld, Presentation at Advancing Global Nutrition for Adolescent and Family Health:Innovations in Research and Training 201811 Figure source: Ahmed et al Ann Nutr Metab 20129
To set the stage, Sudfeld presented some ofthe data on the prevalence of underweightand overweight males and females accordingto the ARISE survey in five sites in Africa (seeTable 21). He noted that undernutrition wasmore common in most of the communitiessampled, but there is a transition underwaytoward greater proportions of overweightpeople. However, Ghana is an outlier inwhich the proportion of overweight femalesis three times as large as the proportion ofunderweight females.Table 1. Proportions of overweight and underweight males and females (ARISE survey preliminary data)SiteSex% Underweight (95% CI)% Overweight (95%CI)Harar, EthiopiaMale24.4 (20.8, 28.4)7.4 (5.4, 10.1)Female18.1 (15.1, 21.5)8.9 (6.8, 11.6)Male6.6 (4.8, 9.1)8.0 (5.9, 10.6)Female7.3 (5.2, 10.2)8.0 (5.8, 11.1)10.3 (7.2, 14.5)7.8 (5.2, 11.6)Female5.2 (3.3, 8.2)14.0 (10.7, 18.0)Male26.0 (21.6, 30.9)3.0 (1.5, 5.4)Female12.2 (9.3, 15.7)7.8 (5.6, 10.8)Male15.5 (12.7, 18.8)4.0 (2.6, 6.0)Female12.8 (10.5, 15.6)6.1 (4.5, 8.1)Kersa, EthiopiaNingo Prampram, Ghana MaleIbadan, NigeriaDodoma, TanzaniaSource: Sudfeld, Presentation at Advancing Global Nutrition for Adolescent and Family Health:Innovations in Research and Training 2018.2.1.2 Anemia in adolescentsMuch of Sudfeld’s presentation focusedon anemia in adolescents. He reportedthat around 1.6 billion people worldwideare anemic, or around 23% of the globalpopulation.2 However, adolescent girls aredrastically overrepresented in this population.The prevalence of anemia among adolescentsvaries widely in different regions of the world.2 Stevens et al Lancet Glob Health 201310It affects around half of non-pregnant adultwomen (aged 15-49 years) in south Asia(47%) and in central and west Africa (48%),both of which are very large populations. Theprevalence of anemia is lower in Latin America(18%-19%) and in East Africa (28%). Evenwithin the ARISE sites, there is a gradient inthe amount of anemia seen.
Advancing Global Nutrition for Adolescent and Family Health: Innovations in Research and TrainingBox 2. Critical transitions in adolescenceSudfeld remarked that adolescence is a time of critical transitions, which is illustratedby changes in the top-ranking causes of death among adolescents by gender andage group worldwide. For males aged 10-14 years, the top three causes of death areroad injury, drowning, and lower respiratory infection; for females in the same agegroup, the top three causes are lower respiratory infections, diarrheal diseases, andmeningitis. This indicates that younger adolescents (especially females) tend to beaffected by communicable diseases, but there is a dramatic shift in causes of deathfor adolescents aged 15-19 years. For females, the most common causes of death arematernal/pregnancy-related conditions, self-harm, and road injury and for males, themost common causes are road injury, self-harm, and interpersonal violence. Sudfeldnoted that across both genders, mental health (self-harm) emerges as the secondmost common cause of death among older adolescents that is not ranked in the topfive causes of death for either gender among the younger adolescents. This reflectsthe transition in the risks faced by adolescents as they grow older and underscoresthe need for targeted interventions that are tailored to specific age groups and gendergroups. The same intervention will probably not have the same impact or require thesame type of messaging to reach these different groups. He added that interventionswill likely need to be country- and setting-specific to achieve the greatest impact. Thesedecisions are critical in designing and implementing interventions targeting adolescentsin the domain of sexual and reproductive health.Source: Sudfeld, Presentation at Advancing Global Nutrition for Adolescent and FamilyHealth: Innovations in Research and Training 2018.Anemia is a reduction in the number of redblood cells or in the quality or quantity ofhemoglobin. It has many possible causes,ranging from genetic hemoglobin disordersto infectious diseases to nutrition. Sudfeldfocused on iron deficiency, which is anutritional cause of anemia in most settings.3Adolescent girls are at particular risk foranemia due to menstrual blood losses, rapidgrowth with expansion of the red cell mass,and increased tissue iron requirementsthat make them particularly vulnerableto iron deficiency compared to their malecounterparts. The foremost effect of anemiais fatigue, followed by reduced productivity(by an estimated 30%) and reduced cognitiveperformance. The effects of anemia place ahuge economic burden on societies aroundthe world. A study in Bangladesh estimatedthe economic cost of anemia to be 7.9% ofGDP due to the loss of productivity.4 Anemiaamong adolescents can also contributesignificantly to disability-adjusted life years(DALYs). Productivity loss due to irondeficiency anemia is the leading cause ofDALYs among adolescent females aged 10-14years (1161 DALYs per 100,000) and 15-19years (836 per 100,000).5 Anemia can alsobe a cause of death (see Box 21) as well asa barrier for staying in school because of itscognitive effects.Sudfeld provided an overview of the nutritionrelated components of the World HealthOrganization’s Global Accelerated Action for3 Other causes related to nutrition include folic acid deficiency, vitamin B12 deficiency, vitamin A deficiency, and protein-energymalfunction.4 Christian P 2005; UN/SCN 20045 Followed by lower respiratory infections, diarrheal diseases, anxiety disorders, and meningitis in those aged 10-14 years and followed bydepressive disorders, maternal conditions, self-harm, and anxiety disorders among those aged 15-19 years.11
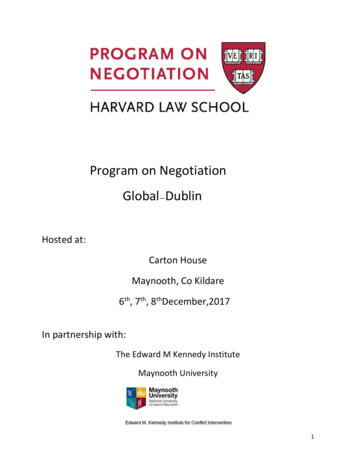
the Health of Adolescents6 (see Figure 2). Itcontains 27 interventions to be implementedbased on the prevalence of the risk factors in aparticular community. WHO does not indicatewhat constitutes high risk or what requiresintervention, so countries themselves decidewhich interventions to implement based ontheir own data. He noted that the guidanceis very broad and the method and deliveryof interventions is not very clear. Within thefocus area of noncommunicable diseases,nutrition, and physical activity, for example, itis unclear which noncommunicable diseasesare being referred to, how to prevent them,or how to detect them. The same appliesto the recommendation regarding anemia:prevention, detection and management ofanemia, especially in adolescent girls.Figure 2. Global Accelerated Action for the Health of Adolescents interventions by focusareaSource: Sudfeld, Presentation at Advancing Global Nutrition for Adolescent and Family Health:Innovations in Research and Training 201876 World Health Organization 2017b7 Figure source: World Health Organization 2017b12
Advancing Global Nutrition for Adolescent and Family Health: Innovations in Research and Training2.1.3 WHO recommendations on ironsupplementationWHO recommendations on ironsupplementation span three differentguideline documents, said Sudfeld. The threerecommendations include: Daily iron supplementation in adultwomen and adolescent girls when anemiaprevalence is 40%8 Intermittent iron supplementation in adultwomen and adolescent girls when anemiaprevalence is 20%9 Intermittent iron supplementationin school-age children when anemiaprevalence is 20%102.1.3.1 Daily iron supplementationin adult women and adolescent girlsThis WHO guideline suggests daily ironsupplementation (30-60 mg elemental irontablets) for three consecutive months in a yearfor menstruating non-pregnant adult womenand adolescent girls when the prevalenceof anemia is greater than 40%.11 Sudfeldnoted that this applies to some settings inIndia, but in East Africa, most settings (otherthan rural communities) will likely not havea prevalence above the 40% threshold. Theguideline does not suggest how to deliver thesupplementation or which three months of theyear it should be given.According to this guideline, WHO has fourresearch priorities in this area. The first isto determine the optimal dose, schedule,and duration of iron supplementation; theeffect of different doses and duration ofiron supplementation on different severity,prevalence or causes of anemia in all WHOregions. Another stated priority is to examinethe effect of adding other micronutrientsto the iron supplement on hemoglobinconcentrations and the prevalence ofanemia. He noted that even if every womanin this group is supplemented, there areremaining causes of anemia that need tobe addressed (e.g., hook worm infection orvitamin B12 deficiency). He said that a studyadding the micronutrient B12 to the ironsupplement and comparing it to the effectof iron supplementation alone could haveeither a large or a null effect, depending onthe prevalence of B12 deficiency in the studygroup. The third priority is implementationresearch on effective behavior-changestrategies for sustained adherence anddelivery mechanisms. He emphasized thatthis supplementation is being given tohealthy, young, non-pregnant girls. Ensuringuptake by a community—particularly for anintervention like iron, which is associated withpregnancy—can be a particular challenge.Supplementation also has side effectsincluding nausea, vomiting, and black stoolthat can cause concern in the communityabout the effect of the medication on theseadolescent girls. WHO’s fourth statedresearch priority is cost, cost–benefit, andthe feasibility analysis of the distribution ofiron supplementation to be taken daily orintermittently among menstruating adultwomen and adolescent girls. He added thatnew distribution mechanisms will likely berequired, for example, through schools andcommunity health workers in parallel to reachin- and out-of-school adolescents.2.1.3.2 Intermittent ironsupplementation in adult women andadolescent girlsThe second WHO guideline concernsintermittent iron and folic acidsupplementation for all menstruatingadolescent young girls and adult womenin settings where anemia rates are greaterthan 20%. Sudfeld noted that that ironsupplementation can increase the risk ofmalaria and its severity. Therefore, in ARISEsettings in Africa in malaria-endemic areas,for example, the provision of iron and folic acidsupplements should be made in conjunction8 World Health Organization 20169 World Health Organization 2011a10 World Health Organization 2011b11 For settings without prevalence data, the guidelines suggest considering proxies for high risk of anemia.13
with adequate measures to prevent, diagnose,and treat malaria. This guideline has its ownset of research priorities that are not directlyaligned. The first priority is to researchthe benefits of intermittent iron on work,productivity, and pregnancy outcomes. Henoted that they have not looked at how theseweekly interventions may affect schooling foradolescent girls. Other priorities include themost effective and safe weekly dose of ironand folic acid to improve folate status andprevent neural tube defects, the effects ofadding other vitamins and minerals on anemiaand other outcomes, and the optimal timeinterval between periods of supplementation.A period of 3 months on and 3 months offis relatively challenging to implement, saidSudfeld.2.1.3.3 Intermittent ironsupplementation in school-agechildrenThe guidelines suggest schemes forintermittent iron supplementation inpreschool and school-age children whenanemia prevalence is greater than 20%.Three months of weekly supplementation arerecommended, followed by three months ofno supplementation and restarting the cycle.The recommended supplements are 25 mgof elemental iron (drops/syrups) per week forpreschool-age children (24-59 months) and45 mg of elemental iron (tablets/capsules)per week for school-age children (5-12years). If feasible, supplementation couldbe given throughout the school year. Again,the guidelines do not provide any specificinformation about when the supplementsshould be administered or why, added Sudfeld.2.1.4 WIFS intervention in IndiaTo illustrate some of the challenges related toweekly iron and folic acid supplementation,Sudfeld described the WIFS interventionimplemented in India. The goal was to reducethe prevalence and severity of anemia inthe adolescent population by targetingtwo groups: school-going adolescent girlsand boys as well as adolescent girls whowere not in school. Together, the two targetgroups were estimated to represent 108million adolescents in India. The interventioncomprised weekly blue 100 mg elementaliron and 500µg folic acid, deworming withalbendazole every 6 months, screening andreferral for anemia, and general nutrition andhealth counseling. He noted that the dose ofiron was much larger than the recommendeddose and probably not optimal for youngpeople or pregnant women. For the firstgroup (school going) the iron was given inschools. For adolescent girls not in school,the iron was given through Anganwadicenters.12 The Ministry of Health providedthe medications. Implementation may notbe universal across all communities becauseof a range of barriers, including issues withparents and the occasional side effects ofiron supplementation. Black stool, nausea,giddiness, heartburn and vomiting have beenoften highlighted by the India media and havecontributed to poor uptake of WIFS in somecommunities.13Sudfeld concluded by suggesting that lessonslearned from the Indian experience could betransferred to settings in Africa for adolescentanemia, although some components willdiffer. He suggested looking at the optimaldose and timing of WIFS and/or daily ironsupplementation depending on anemiaprevalence, given the various approachessuggested in the WHO guidelines. He alsorecommended considering whether a schoolcommunity model would work in ARISEsettings by linking the school and communityto deliver the interventions to in-school andout-of-school adolescents. The deliverymechanisms will likely be different for thesetwo groups of adolescents, he added, whichfurther complicates matters.12 Anganwadi centers are a part of the Indian public healthcare system established to combat child hunger and malnutrition; the centersprovide basic health care in Indian villages.13 Malhotra et al The National medical journal of India 2015; Sarada et al International Journal of Medical Science and Public Health 201614
Advancing Global Nutrition for Adolescent and Family Health: Innovations in Research and Training2.1.5 DiscussionLindsay Jaacks, assistant professor at theHarvard T.H. Chan School of Public Health(U.S.), asked if the teachers observe thechildren taking the blue tablets. AnamitraBarik of the Society for Health andDemographic Surveillance (West Benghal,India) clarified that the recommendation isthat tablets should be taken in school, butmany schools lack drinking water and thechildren often prefer to take the tablet home.Sudfeld noted that children may throw awaythe tablet on their way home. He suggestedconsidering ways to improve this interventionas well as translating lessons learned fromthe India experience to create beneficialinterventions in other settings.Salmaan Keshav
Advancing Global Nutrition for Adolescent and Family Health: Innovations in Research and Training ISBN-10: 1-944302-12-3 ISBN-13: 978-1-944302-12-2 IN COLLABORATION WITH Nutrition