Transcription
"THE WOMAN MUST SATISFY, THE MAN MUST BE SATISFIED"IMPACT OF DOMESTIC VIOLENCE ON WOMEN'SSEXUAL AND REPRODUCTIVE HEALTH IN ARMENIA
"THE WOMAN MUST SATISFY, THE MAN MUST BE SATISFIED"IMPACT OF DOMESTIC VIOLENCE ON WOMEN'SSEXUAL AND REPRODUCTIVE HEALTH IN ARMENIA Women’'s Support Center, 2017 Open Society Foundations-Armenia, 2017The contents of this publication are the sole responsibility of the Women'’s Support Center NGOand Open Society Foundations-Armenia. Publication of this report is supported by Open SocietyFoundations-Armenia, grant N19793. The opinions and analyses expressed in the report are thoseof the authors and do not represent opinions and positions of Open Society Foundations-Armenia.No part of this publication may be used or reproduced in any manner whatsoever without writtenpermission from the Women’'s Support Center’'s experts in the case of brief quotations for articlesand reviews.2017
CONTENT08EXECUTIVE SUMMARY29 PREGNANCY, BIRTH AND THE POSTPARTUM PERIOD10BACKGROUND29 Physical and Psychological Violence and Neglect by Intimate Partners DuringPregnancy10 INTIMATE PARTNER AND FAMILY VIOLENCE: FACTS AND FIGURES30 Specific Manifestations of Mother-in-Law Abuse During Pregnancy12 IMPACT OF ABUSE ON FAMILY PLANNING AND CONTRACEPTION/ABORTION33 Fetal and Maternal Health Complications Linked to Abuse13 IMPACT OF ABUSE ON MATERNAL, FETAL AND CHILD HEALTH OUTCOMES34 Counseling on domestic violence at prenatal visits14 IMPACT OF ABUSE ON SEXUAL HEALTH OUTCOMES35 Changes in the Level and Type of Abuse postpartum15 IMPACT OF ABUSE ON WOMEN’'S SEXUAL AND REPRODUCTIVE HEALTH INARMENIA36 Postpartum Maternal and Child Health Complications Linked to Abuse16 VIOLENCE AND THE HEALTHCARE SYSTEM IN ARMENIA18RATIONALE19METHODOLOGY38 SEXUAL HEALTH38 Nonconsensual Sexual Behavior and Associated Complications40 Shaming and Interference in Sexual Affairs by Mothers-in-Law40 Infidelity in Violent Relationships19 STUDY DESIGN AND POPULATION41 Transmission of Sexually-Transmitted Infections Linked with Abuse22 ETHICAL CONSIDERATIONS42 Spousal Communication Regarding Sexual Matters22 DATA COLLECTION AND ANALYSIS23RESULTS23 CONTRACEPTION, INDUCED ABORTION AND MISCARRIAGE23 Inability to Control Number and Spacing of Children24 Inability to Use Preferred Contraceptive MethodsWomen’'s Support CenterYerevan, 201737 Impaired Ability to Care for Children25 The Intersection of Infertility and Domestic Abuse25 Domestic Violence and Induced Abortion Practices43STRENGTHS AND LIMITATIONS45DISCUSSION AND RECOMMENDATIONS45 CONTRACEPTION, INDUCED ABORTION AND MISCARRIAGE47 PREGNANCY, BIRTH AND THE POSTPARTUM PERIOD48 SEXUAL HEALTH50CITATIONS27 Medical Complications Following Abortion Linked to AbuseThis research study was prepared by the Women'’s Support Center NGO within the context ofthe Open Society Foundations-Armenia funded project “"Addressing sexual and reproductivehealth and rights violations in Armenia.”"27 Miscarriage Experiences Connected with Abuse7
EXECUTIVE SUMMARYIn the seven years since the Women’s Support Center (WSC)opened, its staff have encountered hundreds of survivors whopresent a variety of gynecological issues, are subjected to physicalviolence during pregnancy, are forced to carry out abortions and,due to the nature of the violence they experience, are unable toaccess medical care. However, prior to this publication, no accountsor comprehensive studies had been documented on this subject.This exploratory research study was spearheaded and authored byAni Jilozian with the support of her colleagues at the WSC andvolunteers Ani Misirian, Sophia Yedigarian, Hasmik Djoulakian,Elysia Dardarian, Margaret Babayan, and Tvine Donabedian, whoassisted with the literature review, design of the study tool, as wellas transcription, translation, analysis, and review of interview data.Special thanks as well to Mary Smbatyan for her work in translatingthe final product to Armenian and Ani Asribabayan for designingthe final report.The current study aims at elucidating the unique barriers facingfemale survivors of domestic violence in Armenia in relation totheir sexual and reproductive health. The report is a culminationof several months’ work in collecting and analyzing data fromWSC beneficiaries. A short summary of the report’s key findings ispresented below.8Survivors of intimate partner and family violence who participatedin the study were often unable to have their preferred number ofchildren or birth spacing, and the majority did not use any form ofcontraception, despite the fact that several expressed the desire.The violence led many to have little to no decision-making powerwith respect to choosing contraception, especially in assertingcondom use. The majority of the survivors had abortions, someof which were forced or pressured by intimate partners and familymembers. Medical services for abortion complications were oftennot accessible to survivors. Some of the survivors experiencedmiscarriages due to the abuse, and a high proportion were atrisk of miscarriage throughout pregnancy due to physical andpsychological harm as well as the inability to access medical helpas a result of the abuse.Based on the findings, the authors developed severalrecommendations geared toward civil society, government, andgeneral and specialized service providers working in the field ofviolence, which are presented at the end of this report. As Armeniafinds itself at a critical crossroads, with a standalone domesticviolence law soon to be adopted, it is our hope that state authoritiesand other stakeholders will utilize the study recommendations toimprove domestic violence service provision. Additionally, we hopethe study will pave the way for future large-scale studies on thisimportant topic and the strengthening of multisectoral mechanismsto ensure that survivors are adequately supported, can properlyaccess health services, and lead abuse-free lives.The majority of survivors were physically abused by intimate partnersduring their pregnancies. All were subjected to psychological abuseduring pregnancy by partners and, in half of the cases, by mothersin-law. The women reported symptoms of depression, anxiety,and suicidal ideation. Mothers-in-law forced women to carry outheavy labor, refused to meet their basic needs, and would not allowthem to access health services during pregnancy. The abuse ledsurvivors to delay their first prenatal visit by several months or notpresent for routine prenatal counseling sessions. The intervieweeswere often unable to choose a desired medical provider or consultprivately with physicians. A variety of maternal, fetal, and newbornhealth complications arose as a result of the abuse and inability toseek medical care. Health providers failed to counsel survivors whoexhibited symptoms of abuse on domestic violence and survivors,in turn, were reticent in reaching out for support from medicalproviders.9
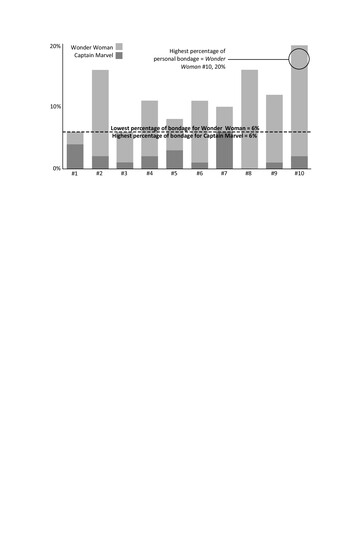
BACKGROUNDINTIMATE PARTNER AND FAMILY VIOLENCE:FACTS AND FIGURESIntimate partner violence (IPV) is any kind of abuse by someonewithin an intimate relationship, manifesting as acts of physical orsexual violence, emotional abuse, and controlling behaviors.1 IPVcan occur in all socioeconomic, religious, and cultural groups, yetthe victims are usually women, and the most common forms of IPVare carried out by male intimate partners or ex-partners.2 Globally,the prevalence of IPV is staggering. A 2013 WHO multi-countrystudy that researched the prevalence of IPV among more than24,000 women in 10 countries found that women are subjected todifferent kinds of violence: almost one third (30%) of all women whohave been in a relationship have experienced IPV, and in some partsof the world, up to 38% of women have been abused by an intimatepartner.324,000WOMENIN10COUNTRIESARE SUBJECTEDTO VIOLENCE1030%OF WOMENEXPERIENCE IPVThe prevalence of IPV in Armenia is also noteworthy. In a 2016 surveypublished by the UNFPA, 45.9% of surveyed women were victims ofpsychological violence and/or emotional abuse, 21.3% were victimsof economic abuse, and 12.5% were victims of physical abuse.4 Thedata regarding sexual violence as perpetrated and reported bymen indicates that 14.6% of women had been victims of sexualviolence.5 These numbers are even higher in other studies, suchas one conducted by the Proactive Society for the Organization forSecurity and Co-operation in Europe, which found that 59.6% ofrespondents had experienced IPV over the course of their lives.6IN ARMENIAAccording to 2016 UNFPA data45.9%OF WOMEN EXPERIENCE PSYCHOLOGICAL VIOLENCE21.3%OF WOMEN EXPERIENCE ECONOMIC ABUSE14.6%OF WOMEN EXPERIENCE SEXUAL VIOLENCE12.5%OF WOMEN EXPERIENCE PHYSICAL ABUSEViolence is a cyclical occurrence in intimate relationships, withabusers’ behavior often changing drastically over time. Victims of IPVare often perceived as unable to leave their abusers because theyare passive victims. In reality, these women often adopt strategiesto ensure maximum safety for themselves and their children.7 Thisis often done in ways that can limit the type or length of abuseand limit the abuse seen or inflicted upon their children. Womenchoose not to leave their violent partners for a number of reasons,the majority of which are: belief that the partner will change andestablish a loving relationship again; fear of retaliation, as leaving isthe most dangerous time for a woman; lack of economic support,as women often do not work as a result of the abuse; concern fortheir children, as without financial means they will be unable toproperly care for them; and lack of support from their family andfriends in cultures where it is traditionally unacceptable to leaveone’s husband, even for reasons of abuse.8Family violence is also prevalent on a global scale, and includeschild abuse and neglect, elder abuse, violence based on “honor” ortradition, and forced marriage. In the Armenian context, mothersin-law in particular have often been found to be abusive towardtheir daughters-in-law. One 2007 survey carried out with over 1,000women found that, of the women who reported abuse, nearly onethird (28%) reported that they were psychologically abused, roughlyone in five (19%) moderately physically abused, and over one in ten(13%) severely physically abused by their mothers-in-law.9IN ARMENIA, AMONG WOMEN WHOARE ABUSED, MOTHERS-IN-LAW AREREPORTED TO CARRY OUT:28% OF PSYCHOLOGICAL VIOLENCE19% OF MODERATE PHYSICAL VIOLENCE13% OF SEVERE PHYSICAL VIOLENCEIntimate partner and family violence impacts women’s health,resulting in reproductive illnesses, psychological distress, fertilityproblems, and a range of other sexual and reproductive healthproblems. We offer a review of the existing data below.11
IMPACT OF ABUSE ON FAMILY PLANNING ANDCONTRACEPTION / ABORTIONReproductive control, a type of IPV, can leave women powerlesswith regards to controlling their fertility, accessing reproductivehealth services, using contraceptives, and accessing abortion.Women experience reproductive control throughout all stages oftheir sexual relationships, with one type of control rarely isolatedfrom the others.10 In a study based in the United States, 35% ofwomen who reported physical or sexual violence also reportedreproductive control.11A review of medical records of clinics from United States-basedfamily planning clinics revealed that women who reported sexualor physical violence in the past year were over 6 times as likely tochange contraceptive methods or use emergency contraception,and nearly 10 times more likely to not use contraception at all.12In another study, women who experienced both physical andemotional violence disclosed that they were significantly morelikely to lessen contraceptive use as compared to women who hadnot experienced any abuse.13 This corroborates with data on birthspacing, with one analysis of several countries in sub-Saharan Africarevealing that the presence of IPV resulted in shortened interbirthintervals among the nearly 50,000 women surveyed.1412The co-occurrence of IPV and family violence often affects women’sreproductive health and decision-making. One study based in ruralCôte d’Ivoire found that the likelihood of reporting lifetime in-lawabuse increased greatly with the presence of male-perpetrated IPV,and those who experienced in-law abuse were nearly 7 times morelikely to report reproductive control.15 Apart from physical violence,in-law abuse may result in the restricted ability to obtain health care;affect women’s decisions around the number of children—andthe number of sons—they have; and influence and even directlyinterfere with women’s use of contraception.16Reproductive control, or lack thereof, can manifest in other ways.For instance, significant links have been found between pregnancycoercion and birth control sabotage.17 Contraceptive sabotage cantake many forms, including destroying pills or rendering condomsineffective, as well as verbal coercion not to use birth control.18 Onestudy of women in the United States found that, of those reportingbirth control sabotage, 79% also reported partner violence and56% reported pregnancy coercion; co-occurrence of these twophenomena did not differ between physical and sexual IPV.19Communication in relationships also suffers as a result of abuse. In ananalysis of data collected from the medical records of 2,000 women,survivors were found to be less likely to communicate informationabout contraception to abusive partners and more likely to have sexwithout a condom.20 In another study, 21% of respondents reportednot disclosing their birth control or emergency contraceptive useto their abusive partners, and 55% of abused women reportedrarely or never using condoms, of which half reported the reasonbeing refusal on behalf of their abusive partner when asked to usecondoms.21Whether a woman had ever experienced reproductive coercion issignificantly related to fear of asking a partner to use a condomand fear of refusing sex with a partner.22 Studies have shown thatwomen who experience IPV are sometimes forced to weigh theirfear of contracting STIs with their fear of facing abuse by their violentpartners.23 One study in the United States revealed that women inviolent relationships who asked their partner to use a condom were8 times more likely to report being threatened and 14 times morelikely to be beaten.24As a result of poor contraceptive utilization and birth controlsabotage, IPV has been linked as well to unintended pregnancy. Ananalysis of WHO’s multi-country study found that rates of unwantedpregnancy among survivors ranged from 13-68%, with the proportionof unintended pregnancy attributed to IPV at 15%.25 One UnitedStates-based study found that the odds of unintended pregnancyincrease twofold when the consequences of pregnancy coercion andpartner violence were combined.26Each year, out of 80 million unintended pregnancies, at least halfresult in induced abortion, and half of these induced abortions occurin unsafe conditions.27 The 2013 WHO multi-country data suggeststhat women who have been physically or sexually assaulted bytheir partners are more than twice as likely to have an abortion.28Moreover, women in violent relationships report feeling coercedinto having an abortion and are 3 times more likely to conceal theirabortion, for fear of further violence.29In addition to impacting the use of contraception and abortion,intimate partner and family violence is also associated with miscarriage,infertility, and subfertility. There is evidence that increased stress inabusive environments may influence infertility rates.30 It is thoughtthat IPV causes permanent and irreversible health damage, suchas pelvic inflammatory disease-induced secondary infertility, thusaffecting survivors’ ability to have any more children.31 Furthermore,emerging evidence indicates that infertility and subfertility couldbe both justifications for and outcomes of violence.32 In one studycarried out in rural Côte d’Ivoire, women who did not have childrenwere subjected to abuse and reproductive control by husbands’families, which included threats of encouraging divorce, refusal tomeet basic needs, and emboldening abusive husbands to physicallyabuse their wives if they did not become pregnant.32IMPACT OF ABUSE ON MATERNAL, FETAL AND CHILDHEALTH OUTCOMESAccording to a 2005 multi-country WHO study, over 5% of everpregnant women had been physically abused during at least onepregnancy in 11 of the 15 settings surveyed, and between onequarter and one half of women abused in pregnancy reported beingkicked or punched in the abdomen. Research has shown that abuseoften worsens in pregnancy, with one study revealing that roughlyhalf of respondents who had reported sexual or physical abuse alsoreported that the frequency of abuse increased after becomingpregnant.Pregnant women who are abused endure a number of dangerouscomplications and have adverse pregnancy outcomes. The presenceof violence in pregnancy is associated with maternal mortality, prenatalbleeding, fetal fractures, chorioamnionitis, and maternal infections,as well as anaemia, premature rupture of the membranes, andgestational hypertension. In an analysis of Cameroon DemographicHealth Survey data, it was found that women who had experiencedany form of spousal violence had a 50% increased risk of any typeof fetal loss (i.e. miscarriage or stillbirth) during a single or repeatedepisode as compared to nonabused women. In a longitudinal study,about half of the roughly 25% of women who reported having amiscarriage disclosed that it was due to abuse, and women were28 times more likely to report having an abuse-induced miscarriagewhen a pregnancy was the result of the abuser refusing birth control.3913
There is much data on the association between IPV and preterm birthand low birth weight.40,41,42,43 In one study, women who experiencedphysical violence were 3 times more likely to have preterm deliveryand 4 times as likely to experience low birth weight, citing placentaldamage, poor health, and restricted access to medical care amongthe possible factors involved.44 Women affected by IPV are alsomore likely to experience growth restriction in utero and small sizefor gestational age due to various health complications and STIs.45Several studies have also found that past or recent IPV — beforeor during a pregnancy — may result in premature cessation ofbreastfeeding, which could affect infant health.46IPV also results in negative mental health outcomes, with posttraumatic stress disorder being the most prevalent adverse mentalhealth outcome of IPV and twice as likely to manifest in womenwho have been abused as opposed to non-abused women.47 In theaforementioned 2005 multi-country WHO study, abused womenshowed higher levels of emotional distress as compared with nonabused women, reporting that they cried easily, were unable toenjoy life, and had suicidal ideation and/or attempted suicide.48 Inone study carried out in the US, women had a 50% higher chance ofreporting postpartum depression if they had experienced sexual IPVas compared with non-abused women.49 Importantly, psychologicaldistress often manifests in somatic symptoms. In a study lookingat Mexican women 27-72 hours postpartum, hypertensive diseasewas found to be a significant maternal health problem amongsurvivors who were abused during their pregnancies, most of whomexperienced psychological abuse alone.5014Family violence also leads survivors to experience adverse pregnancyoutcomes. A study of South Asians in the US presents testimoniesfrom women who describe the violence they endured from theirmothers-in-law, including domestic servitude and heavy labor evenduring pregnancy.51 Another examining the impact that mothersin-law had on maternal health in Mali found that abusive mothersin-law controlled how often women had antenatal care visits, whenand where visits and the delivery took place, and whether womenreceived postnatal care.52 This is important, as access to medicalcare in pregnancy and violence are intricately linked, with findingsthat women exposed to violence receive less prenatal care.53,54 Inone study, survivors living in rural Timor-Leste were 3 times lesslikely than women who did not report abuse to have made lessthan 4 antenatal care visits.55IMPACT OF ABUSE ON SEXUAL HEALTH OUTCOMESExposure to IPV is an important contributor to sexual risk andadverse sexual health outcomes. Women who experience IPVare at greater risk of STIs, vaginal bleeding, vaginal infection,fibroids, decreased sexual desire, genital irritation, pain duringintercourse, pelvic pain, and urinary tract infections.56 Similarly,women who endure forced sex in a relationship experience moregynecological issues, such as urinary problems, decreased sexualdesire, and abdominal pain and cramping.57 There is compellingand consistent evidence that physical IPV has an effect on women’ssexual dysfunction, specifically in relation to chronic pelvic pain, aswell as sexual satisfaction and lack of sexual pleasure.58IPV has been found to be positively associated with increasedpartner-related sexual risks, such as partner nonmonogamy,condom nonuse, and partners’ increased risk of having an STI.59 Ina study examining the Indian context, partner infidelity was foundto be more common among abusive husbands, who were also atgreater risk of contracting STIs and transmitting them to theirwives due to higher levels of exhibited extramarital risk behavior(i.e. unprotected extramarital sex and sex with commercial sexworkers).60IPV greatly increases the risk of acquiring STIs, like HIV. In someregions of the world, survivors of IPV are 1.5 times more likely toacquire HIV, as compared with women who have not experiencedIPV.61 In an analysis of data from a recent Demographic and HealthSurvey in Kenya, married women who were victims of physicalviolence were twice as likely to test positively for HIV as comparedwith women who did not experience violence of this kind.62 Thisputs women at a greater risk of experiencing adverse mental healtheffects. According to one study, women who had ever experiencedIPV as adults and who were HIV positive were 7 times more likelyto have depression, 12.5 times more likely to have ever attemptedsuicide, and 5 times more likely to have experienced anxiety ascompared with their non-HIV positive counterparts who had notbeen victims of IPV.63 Women who experience IPV may be at agreater risk of contracting HIV due to the inability to negotiatesafe sex practices such as condom use, frequency of intercourse,and types of sexual acts, and they may be less likely to disclosehaving HIV and to seek out testing and/or treatment for HIV dueto fear of their partner’s reaction.64IMPACT OF ABUSE ON WOMEN’S SEXUAL ANDREPRODUCTIVE HEALTH IN ARMENIAAttitudes in Armenia relating to sexual and reproductive healthand rights are telling. According to the 2015 Gender BarometerStudy, while 73% of respondents agreed that it is very important forArmenian men to have a fulfilling and romantic sexual life, only 60%of respondents believed the same about Armenian women.65 Of therespondents, 86.6% completely agreed that a girl should remain avirgin until marriage, and 77.8% completely agreed that a woman’smost important mission is to have a child.66 In the aforementioned2016 survey study, 27.7% of men agreed that there are times when awoman deserves to be beaten, with 55.4% of respondents agreeingthat it is okay for a man to hit a woman if she cheats on him.67Particularly disconcerting is the 7.6% of men in the UNFPA studyreporting to have coerced or forced a woman or girl to have sexwith them at one point in their lives, with two thirds reporting thatthe forced sex was with their female intimate partner. Concerningas well is the fact that nearly two thirds (63.9%) of male respondentsin the study reported not having used a condom the last time theyhad sex, with 30% of them also reporting that their most recentsexual encounter was with someone other than their partner.68These statistics reflect behaviors and attitudes reinforced bythe legal landscape surrounding IPV in Armenia; perpetrators’sentences are often reduced, as court discussants often usealleged infidelity as a reason to justify violence against womenand sometimes even imply that further punishment should havebeen dealt to the woman.6915
ACCORDING TO 2016 UNFPA DATAof men report having coerced/forced a woman7.6% or girl to have sex with themof men report having their most recent sexual30% encounter with someone other than their partner63.9% of men report not having used a condom in theirmost recent sexual encounterIn Armenia, contraceptive utilization remains low and abortionis common, which is in large part due to poor awareness ofcontraception as well as low availability, accessibility, andaffordability of effective contraceptive methods.70 Armenia hasone of the world’s highest skewed sex ratios at birth, with 114males born per 100 females as of 2012 data.71 Son preference isrelated to the belief that sons continue the family lineage, receiveinheritance, and care for aging parents.72 It is also due to therelative value prescribed to men over women and the valorizationof masculinity.73 Though not all sex-selective abortion carried outin Armenia is coercive, for many the choice is between aborting afemale fetus or keeping it and being further abused by intimatepartners and/or in-laws as a result.7416Among the few studies carried out in this field, significant links havebeen made between IPV and poor reproductive health indicators inArmenia. A nationwide study carried out by the National StatisticalService and UNFPA Armenia found that stillbirths were 5 timesmore common among Armenian women exposed to physicalviolence than those not exposed to abuse.75 With regards tosexual health, the same survey found that the women were 2 ormore times likely to report symptoms of venereal disease if theywere subjected to violence.76VIOLENCE AND THE HEALTHCARE SYSTEM IN ARMENIAPhysicians can play a critically important role in interrupting thecycle of IPV. The authors of a review of 74 international studies onthe associations between IPV and termination of pregnancy arguethat physicians who administer abortions should also providequestionnaires, counseling, and intervention strategies to womenwho may be experiencing IPV.77 Due to the combined harmfuleffects of IPV and a history of adverse pregnancy outcomes onwomen’s pregnancies, researchers have also recommended thathealth centers provide “screening for violence to all pregnantwomen with a history of previous adverse pregnancy outcomes,”not just those who display physical and mental indications of IPV.78themselves name “fear of their partner’s retaliation, shame,humiliation, denial, and a belief that health care professionalscannot do much to help them” as reasons they do not disclosetheir abuse.81 Although more conclusive data is needed, the studyhighlights the systematic disengagement of medical professionalsfrom situations, which clearly indicate IPV. More training andknowledge about referral options and a demonstrated institutionalinvestment in women’s overall health, which IPV greatly affects,would allow doctors to feel more equipped to assist womenenduring IPV and reach out to advocacy organizations.82Carrying out such screenings and interventions is difficult in anycontext, and Armenian health centers are no exception. Researchon the knowledge, attitudes, and practices of healthcare providersin Armenia who encounter abused women shows that the greatestdeterrent to physician support and intervention is the lack ofinformation and skills about how to assist women exposed to IPV.79Most of the general practitioners, gynecologists, and physicians whoparticipated in the aforementioned study believed the extent of ahealthcare provider’s role was talking to women and giving advice;however, only about half of the participants were comfortablequestioning patients they suspected may be exposed to IPV abouttheir possible abuse.80Healthcare professionals list “lack of trust, fear from the husband/partner, woman’s wish to disclose, inappropriateness of askingquestions, [and] presence of the husband/relatives of husband,”among the barriers to helping abused women, while women17
METHODOLOGYSTUDY DESIGN AND POPULATIONRATIONALEThe present study aims to elucidate the sexual and reproductivehealth issues present among survivors of domestic violence inArmenia and their decision-making capacities. It also examines theunique barriers and issues that prevent domestic violence survivorsfrom accessing health services, including gaps in the preparednessand response of health care professionals. Robust literatureon Armenia-specific sexual and reproductive health outcomesassociated with IPV data does not yet exist. For instance, there is notyet enough research on the social factors that influence Armenianwomen who have abortions, and developing effective interventionstrategies around family planning and unsafe or illegal abortionshinges on understanding those factors.83 This gap in research isfurther reason for this exploratory study, which presents the rangeof reasons why research around the effects of intimate partner andfamily violence on Armenian women’s sexual and reproductivehealth is critical.18The research project is a qualitative analysis employing individual,in-depth interviews. Interviews were chosen over other qualitativemethods due to the sensitivity of the subject matter. An exploratoryqualitative research methodology was chosen over quantitativemethods, given the lack of research examining how abusiverelationships play a critical role in shaping women’s decision-makingaround and experiences with family planning, contraception,induced abortion, miscarriage, pregnancy, and various forms ofsexual abuse and discrimination in the Armenian context.The sample population was determined using conveniencew
"THE WOMAN MUST SATISFY, THE MAN MUST BE SATISFIED" IMPACT OF DOMESTIC VIOLENCE ON WOMEN'S SEXUAL AND REPRODUCTIVE HEALTH IN ARMENIA "THE WOMAN MUST SATISFY, THE MAN MUST BE SATISFIED" . Transmission of Sexually-Transmitted Infections Linked wi