Transcription
DSM-5:Classification, Criteria, and Use
PurposeThis course is for clinicians who are alreadyfamiliar with DSM-IV-TR, its content, and itsuse. This presentation is solely to facilitatetransition from DSM-IV-TR to DSM-5 and isnot intended to be a basic course on DSM-5.Copyright 2013. American Psychiatric Association.
DSMI: 1952 influenced byMenninger’s WW II classificationscheme called Medical 203 for theArmy. ICD 6 had just beenpublished. 106 mental disorders DSM II: 1968 still withpsychodynamic influence
DSMII Seventh Printing: 1974Removed Homosexuality as adisease (though retained sexualorientation disturbance) DSM III: 1980 Influenced by RDCused at Wash U and NYSPI, theMultiaxial system appeared
DSMIII R: 1987 Reorganizedcategories and introduced PMDDand Ego Dystonic Homosexuality DSM IV: 1994 and DSM IV TR 2000Asperger Disorder makes thegrade! DSM 5: no more roman numerals
ADAMHA-WHO Collaboration (1980-94) 14 international Task Forces examinedapproaches of national “schools” ofpsychiatry Copenhagen Conference, April 1982: 150participants from 47 countries Resulted in joint WHO/ADAMHA/APA effortto develop DSM-IV and ICD-10; CIDI, SCAN,and IPDE. ICF was next phaseCopyright 2013. American Psychiatric Association.
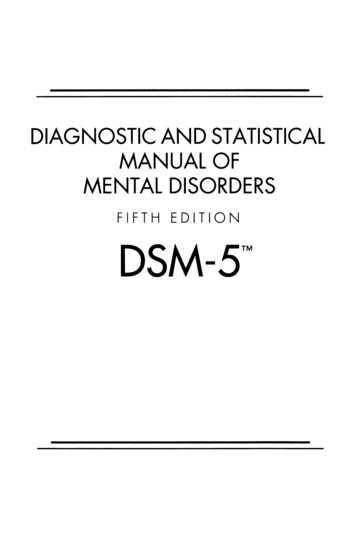
DSM-IPresumedetiologyDSM-5New ntal, culture,impairment thresholds,living ualizationExplicit criteria(emphasis on reliabilityrather than validity)DSM–IVRequires clinicallysignificant distressor impairmentDSM-III-RCriteria broadenedMost hierarchiesdroppedCopyright 2013. American Psychiatric Association.
DSM-III-R:Hierarchical arrangementpartially abandoned, but DSM-IV:Strict separation betweendisorders continues DSM-5:?Copyright 2013. American Psychiatric Association.
Perceived Shortcomings in DSM-IV High rates of comorbidity High use of –NOS category Treatment non-specificity Inability to find a laboratory markers/tests DSM is starting to hinder researchprogressCopyright 2013. American Psychiatric Association.
New Developments Pressures to improve “validity” Move toward an “etiologically based” classification Are there data in these areas that can be helpful indeveloping/changing/refining diagnoses? Cognitive or behavioral science Family studies and molecular genetics Neuroscience—NIMH RDoC Program Functional and structural imagingRequires a ShiftNeo-Kraepelinian to ?Copyright 2013. American Psychiatric Association.
Strategies for Improving DSM Incorporate research into the revisionand evolution of the classification Move beyond a process of clinicalconsensus and build diagnoses on afoundation of empirical findings fromscientific disciplines Seek multidisciplinary, internationalscientific participation in the task ofplanning the DSM-5 revisionCopyright 2013. American Psychiatric Association.
Copyright 2013. American Psychiatric Association.
13 Conferences (2003-08)10 monographs published Dimensional Models of Personality DisordersDiagnostic Issues in Substance Use DisordersDiagnostic Issues in DementiaDimensional Approaches in Diagnostic ClassificationStress-Induced and Fear Circuitry DisordersSomatic Presentations of Mental DisordersDeconstructing PsychosisDepression and GADObsessive-Compulsive Behavior Spectrum DisordersPublic Health Aspects of Psychiatric DiagnosisMore than 200 journal articles publishedCopyright 2013. American Psychiatric Association.
Copyright 2013. American Psychiatric Association.
DSM-5 DevelopmentDSM-5 Task Force(appointed 2006-2007) Work group chairs Health professionals from stakeholder groupsDSM-5 Work Groups(appointed 2007-2008) Members work in specific diagnostic areas(e.g., Mood Disorders, Anxiety Disorder, etc.) Advisors for work groupsFor more information, visit www.dsm5.orgCopyright 2013. American Psychiatric Association.
ADHD & Disruptive Behavior Disorders (David Shaffer, M.D.)Anxiety, Obsessive-Compulsive Spectrum, Posttraumatic, andDissociative Disorders (Katharine Phillips, M.D.)Disorders in Childhood and Adolescence (Daniel Pine, M.D.)Eating Disorders (Timothy Walsh, M.D.)Mood Disorders (Jan Fawcett, M.D.)Neurocognitive Disorders (Dan Blazer, M.D.; Ron Petersen, M.D. [CoChair]; Dilip Jeste, M.D. [Chair Emeritus])Neurodevelopmental Disorders (Susan Swedo, M.D.)Personality and Personality Disorders (Andrew Skodol, M.D.)Psychotic Disorders (William Carpenter, M.D.) Sexual and Gender Identity Disorders (Kenneth Zucker, Ph.D.)Sleep-Wake Disorders (Charles Reynolds, M.D.)Somatic Distress Disorders (Joel Dimsdale, M.D.) Substance-Related Disorders (Charles OʼBrien, M.D., Ph.D.) Copyright 2013. American Psychiatric Association.
Cross-Cutting Study Groups and Chairs Diagnostic Spectra (Steven Hyman, M.D.) Life Span Developmental Approach Study Group(Susan K. Schultz, M.D.) Gender and Cross-Cultural Study Group(Kimberly Yonkers, M.D.) Psychiatric/General Medical Interface Study Group(Lawson Wulsin, M.D.) Impairment and Disability Assessment(Jane S. Paulsen, Ph.D.) Diagnostic Assessment Instruments(Jack D. Burke, Jr., M.D., M.P.H.)Copyright 2013. American Psychiatric Association.
Definition of a Mental DisorderDSM-5:A mental disorder is a syndrome characterized by clinicallysignificant disturbance in an individualʼs cognition, emotionregulation, or behavior that reflects a dysfunction in thepsychological, biological, or developmental processesunderlying mental functioning. Mental disorders are usuallyassociated with significant distress or disability in social,occupational, or other important activities. An expectable orculturally approved response to a common stressor or loss,such as the death of a loved one, is not a mental disorder.Socially deviant behavior (e.g., political, religious, or sexual)and conflicts that are primarily between the individual andsociety are not mental disorders unless the deviance or conflictresults from a dysfunction in the individual, as described above.Reprinted with permission from the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition,(Copyright 2013). American Psychiatric Association.
Definition of a Mental Disorder The diagnosis of a mental disordershould have clinical utility: it should helpclinicians to determine prognosis,treatment plans, and potential treatmentoutcomes for their patients. However, thediagnosis of a mental disorder is notequivalent to a need for treatment.Copyright 2013. American Psychiatric Association.
Definition of a Mental Disorder Approaches to validating diagnosticcriteria for discrete categorical mentaldisorders have included the followingtypes of evidence: antecedent validators (similar genetic markers,family traits, temperament, and environmentalexposure);concurrent validators (similar neural substrates,biomarkers, emotional and cognitive processing,and symptom similarity);and predictive validators (similar clinical courseand treatment response).Copyright 2013. American Psychiatric Association.
Definition of a Mental Disorder Available evidence shows that thesevalidators cross existing diagnosticboundaries but tend to congregate morefrequently within and across adjacentDSM-5 chapter groups.Until incontrovertible etiological orpathophysiological mechanisms areidentified to fully validate specificdisorders or disorder spectra, the mostimportant standard for the DSM-5disorder criteria will be their clinical utility.Copyright 2013. American Psychiatric Association.
DSM-5 Structure SectionI: DSM-5 Basics Section II: Essential Elements: DiagnosticCriteria and Codes Section III: Emerging Measures andModels Appendix IndexCopyright 2013. American Psychiatric Association.
25“According the architects of DSM-5, theintroduction of dimensions is their mostimportance advance” --Abraham Nussbaum, MDquoting Darrel Regier (Int J Methods Psychiatr Res, 2007)25
26 WHYDIMENSIONS? * (per Nussbaum, A. . 2013)Prior versions of DSM could not always distinguish normalityfrom pathology and one mental disorder from another.By introducing dimensions we can:1. Acknowledge psychiatric symptoms that are not partdiaganostic criteria of patientʼs primary psychiatric disorder(e.g. panic attacks in pt with MDD)2. measure the magnitude of a symptom (whether part of theprimary disorder or not)3. track progress of treatment4. screen for mental disorders in particular patient popluations(e.g. anxiety among adolescent patients)
BriefDSM-5 developmental history Guidance on use of the manual Definition of a mental disorder Cautionary forensic statement Brief DSM-5 classification summaryCopyright 2013. American Psychiatric Association.
A. Neurodevelopmental DisordersB. Schizophrenia Spectrum and Other PsychoticDisordersC. Bipolar and Related DisordersD. Depressive DisordersE. Anxiety DisordersF. Obsessive-Compulsive and Related DisordersG. Trauma- and Stressor-Related DisordersH. Dissociative DisordersCopyright 2013. American Psychiatric Association.
J. Somatic Symptom and Related DisordersK. Feeding and Eating DisordersL. Elimination DisordersM. Sleep-Wake DisordersN. Sexual DysfunctionsP. Gender DysphoriaCopyright 2013. American Psychiatric Association.
Q. Disruptive, Impulse-Control, and Conduct DisordersR. Substance-Related and Addictive DisordersS. Neurocognitive DisordersT. Personality DisordersU. Paraphilic DisordersV. Other DisordersMedication-Induced Movement Disorders and OtherAdverse Effects of MedicationOther Conditions That May Be a Focus of ClinicalAttentionCopyright 2013. American Psychiatric Association.
Section III: Purpose SectionIII serves as a designated location,separate from diagnostic criteria, text, andclinical codes, for items that appear to haveinitial support in terms of clinical use butrequire further research before beingofficially recommended as part of the mainbody of the manual This separation clearly conveys to readers that thecontent may be clinically useful and warrants review,but is not a part of an official diagnosis of a mentaldisorder and cannot be used as suchCopyright 2013. American Psychiatric Association.
Section III: Content SectionIII: Emerging Measures and Models Assessment CulturalMeasuresFormulation AlternativeDSM-5 Model for Personality Conditionsfor Further StudyDisordersCopyright 2013. American Psychiatric Association.
Section III: Content Section III, Conditions for Further Study Attenuated Psychosis Syndrome Depressive Episodes With Short Duration Hypomania Persistent Complex Bereavement Disorder Caffeine Use Disorder Internet Gaming Disorder Neurobehavioral Disorder Due to Prenatal AlcoholExposure Suicidal Behavior Disorder Non-suicidal Self-InjuryCopyright 2013. American Psychiatric Association.
Assess patient characteristics not necessarilyincluded in diagnostic criteria but of highrelevance to prognosis, treatment planning andoutcome for most patientsIn DSM-5, these include: Level 1 and Level 2 Cross-Cutting Symptomassessments Diagnosis-specific Severity ratings Disability assessmentMay be patient, informant, or clinician completed,depending on the measureCopyright 2013. American Psychiatric Association.
Referred to as “cross-cutting” because it callsattention to symptoms relevant to most, if notall, psychiatric disorders (e.g., mood, anxiety,sleep disturbance, substance use, suicide) Self-administeredby patient 13 symptom domains for adults 12 symptoms domains for children 11 , parentsof children 6 Brief—1-3 questions per symptom domain Screen for important symptoms, not for specificdiagnoses (i.e., “cross-cutting”)Copyright 2013. American Psychiatric Association.
Copyright 2013. American Psychiatric Association.
38Level 1 Cross-Cutting Symptom MeasuresDSM-5 Self-Rated Level 1 Cross-Cutting Symptom Measure—Adult (also availablein print book)DSM-5 Parent/Guardian-Rated Level 1 Cross-Cutting Symptom Measure—ChildAge 6–17 (also available in print book)DSM-5 Self-Rated Level 1 Cross-Cutting Symptom Measure—Child Age 11–17Form)Level 2 Cross-Cutting Symptom MeasuresFor AdultsLEVEL 2—Depression—Adult (PROMIS Emotional Distress— Depression—ShortLEVEL 2—Anger—Adult (PROMIS Emotional Distress-Anger-Short Form)LEVEL 2—Mania—Adult (Altman Self-Rating Mania Scale [ASRM])LEVEL 2—Anxiety—Adult (PROMIS Emotional Distress—Anxiety— Short Form)LEVEL 2—Somatic Symptom—Adult (Patient Health Questionnaire 15 SomaticSymptomSeverity Scale [PHQ-15])LEVEL 2—Sleep Disturbance—Adult (PROMIS—Sleep Disturbance—ShortForm)LEVEL 2—Repetitive Thoughts and Behaviors—Adult (Adapted from the FloridaObsessive-Compulsive Inventory [FOCI] Severity Scale [Part B])LEVEL 2—Substance Use—Adult (Adapted from the NIDA-ModifiedASSIST)For Parents of Children Ages 6–17 (Same as adult but also inattention 38 andirritability measures)
Copyright 2013. American Psychiatric Association.
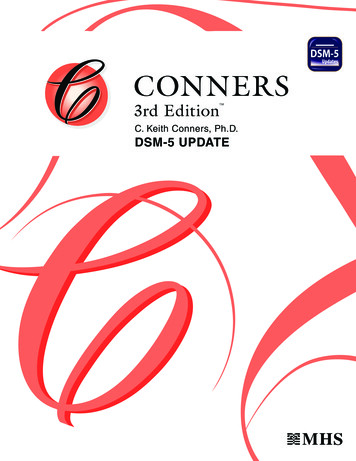
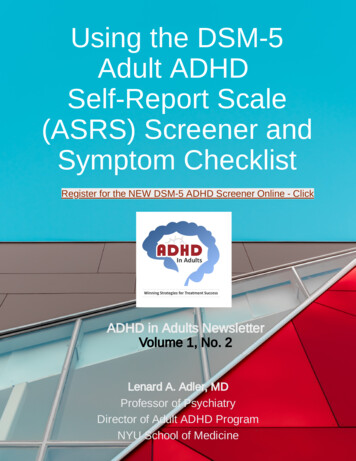
Completed when the corresponding Level 1item is endorsed at the level of “mild” orgreater (for most but not all items, i.e.,psychosis and inattention) Gives a more detailed assessment of thesymptom domain Largely based on pre-existing, well-validatedmeasures, including the SNAP-IV(inattention); NIDA-modified ASSIST(substance use); and PROMIS forms(anger, sleep disturbance, emotional distress)Copyright 2013. American Psychiatric Association.
Please respond to each item by choosing one option per question.Not at allIn the past SEVEN (7) DAYS.My sleep was restless.A little bitSomewhatQuite abitVerymuch 3 4 5 1 2I was satisfied with my sleep. 5 4My sleep was refreshing. 5 4 3 2 1I had difficulty falling asleep. 1 2 3 4 5NeverRarelyOftenAlwaysI had trouble staying asleep. 1 2Sometimes 3 4 5I had trouble sleeping. 1 2 3 4 5I got enough sleep. 5 4 3 2 1In the past SEVEN (7) DAYS My sleep quality was.Very PoorPoorFairGoodVery good 5 4 3 2 1In the past SEVEN (7) DAYS. 3 2 1
For documenting the severity of a specificdisorder using, for example, the frequencyand intensity of its component symptoms Can be administered to individuals with: Adiagnosis meeting full criteria An “other specified” diagnosis, esp. a clinicallysignificant syndrome that does not meetdiagnostic threshold Some clinician-rated, some patient-ratedCopyright 2013. American Psychiatric Association.
43 Disorder-SpecificSeverity MeasuresFor AdultsSeverity Measure for Depression—Adult (Patient Health Questionnaire[PHQ-9])Severity Measure for Separation Anxiety Disorder—AdultSeverity Measure for Specific Phobia—AdultSeverity Measure for Social Anxiety Disorder (Social Phobia)—AdultSeverity Measure for Panic Disorder—AdultSeverity Measure for Agoraphobia—AdultSeverity Measure for Generalized Anxiety Disorder—AdultSeverity of Posttraumatic Stress Symptoms—Adult (National StressfulEvents Survey PTSD Short Scale [NSESS])Severity of Acute Stress Symptoms—Adult (National Stressful EventsSurvey Acute Stress Disorder Short Scale [NSESS])Severity of Dissociative Symptoms—Adult (Brief DissociativeExperiences Scale [DES-B]) 43
essionorAvoli(on) ImpairedCogni(onDepression Mania 0 NotPresent1 Equivocal2 Present,butmild3 Presentandmoderate4 PresentandsevereCopyright 2013. American Psychiatric Association.
Appendix: Content Separate from Section III will be an Appendix,which will includeHighlights of Changes From DSM-IV to DSM-5 Glossary of Technical Terms Glossary of Cultural Concepts of Distress Alphabetical Listing of DSM-5 Diagnoses and Codes(ICD-9-CM and ICD-10-CM) Numerical Listing of DSM-5 Diagnoses and Codes(ICD-9-CM) Numerical Listing of DSM-5 Diagnoses and Codes(ICD-10-CM) DSM-5 Advisors and Other Contributors Copyright 2013. American Psychiatric Association.
ew,Eliminated,andCombinedDisorders(netdifference - ‐15)SpecificMentalDisorders* *NOSDSM- ‐IVDSM- ‐5172157(DSM-IV) and Other Specified/Unspecified (DSM-5) conditions are countedseparately.Copyright 2013. American Psychiatric Association.
NewandEliminatedDisordersinDSM- ‐5NewDisorders(netdifference orderPremenstrualDysphoricDisorder(DSM- ‐IVappendix)HoardingDisorderExcoria(on(Skin- order(splitfromReac:veA achmentDisorder)BingeEa(ngDisorder(DSM- - ‐RelatedSleepDisorder)Sleep- ‐RelatedHypoven(la(on(splitfromBreathing- somniaNOS)CaffeineWithdrawal(DSM- alCondi:ons)15. MildNeurocogni(veDisorder(DSM- nDisorderPolysubstance- ‐RelatedDisorderCopyright 2013. American Psychiatric Association.
CombinedSpecificDisordersinDSM- ‐5(netdifference - ,ChildhoodDisintegra:veDisorder,&Re ʼsdisorder—PDD- ReadingDisorder,MathDisorder,&DisorderofWri ntalDisorder)10. Non- ingDisorder&SleepTerrorDisorder)Copyright 2013. American Psychiatric Association.
CombinedSpecificDisordersinDSM- ‐5(Con(nued)(netdifference - ‐28)11.Genito- caineWithdrawal)22.Substance/Medica(on- ‐InducedDisorders(aggregateofMood( 1),Anxiety( 1),andNeurocogni:ve(- ‐3))Copyright 2013. American Psychiatric Association.
fference 24)NOS(DSM- ‐IV)andOtherSpecified/Unspecified(DSM- ‐5)DSM- ‐IVDSM- SM- sinDSM- specificmentaldisorders.Copyright 2013. American Psychiatric Association.
TheMultiaxial diagnosis is nolonger used In place of Axis I to V, thediagnoses are listed withpsychiatric and medical combined. The convention has been to list theprimary diagnosis for the visit first.
FormerAxis II is placed on this listin no special order Some felt Axis II disorders wereseen as less significant and couldnever be “Primary” Though Axis III is gone, It isimportant to list medical diagnoses
Autism Spectrum Disorder (ASD)(Neurodevelopmental Disorders) ASD replaces DSM-IVʼs autistic disorder,Aspergerʼs disorder, childhood disintegrationdisorder, and pervasive developmentaldisorder not otherwise specified Rationale: Clinicians had been applying the DSM-IVcriteria for these disorders inconsistently andincorrectly; subsequently, reliability data to supporttheir continued separation was very poor. Specifiers can be used to describe variants of ASD(e.g., the former diagnosis of Aspergerʼs can now bediagnosed as autism spectrum disorder, withoutintellectual impairment and without structurallanguage impairment).Copyright 2013. American Psychiatric Association.
AutismSpectrum Disorder associatedwith Rett Syndrome, Level 2Communication Supports, Level 3Behavior supports, With IntellectualImpairment, With Language Impairment(Phrase speech) OR: Autism Spectrum Disorder Level 1behavior supports without intellectual orlanguage impairments
Intellectual Disability (IntellectualDevelopmental Disorder) Mental retardation was renamed intellectualdisability (intellectual developmental disorder) Rationale: The term intellectual disability reflects thewording adopted into U.S. law in 2010 (Rosaʼs Law), inuse in professional journals, and endorsed by certainpatient advocacy groups. The term intellectualdevelopmental disorder is consistent with languageproposed for ICD-11.Greater emphasis on adaptive functioning deficitsrather than IQ scores alone Rationale: Standardized IQ test scores were overemphasized as the determining factor of abilities in DSMIV. Consideration of functioning provides a morecomprehensive assessment of the individual.Copyright 2013. American Psychiatric Association.
Intellectual disability (intellectual developmental disorder) is a disorderwith onset during the developmental period that includes bothintellectual and adaptive functioning deficits in conceptual, social, andpractical domains. The following three criteria must be met:A.Deficits in intellectual functions, such as reasoning, problem solving,planning, abstract thinking, judgment, academic learning, and learningfrom experience, confirmed by both clinical assessment andindividualized, standardized intelligence testing.B.Deficits in adaptive functioning that result in failure to meetdevelopmental and socio-cultural standards for personal independenceand social responsibility. Without ongoing support, the adaptive deficitslimit functioning in one or more activities of daily life, such ascommunication, social participation, and independent living, acrossmultiple environments, such as home, school, work, and community.C.Onset of intellectual and adaptive deficits during the developmentalperiod.Reprinted with permission from the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition,(Copyright 2013). American Psychiatric Association.
Specific Learning Disorder Now presented as a single disorder with codedspecifiers for specific deficits in reading, writing,and mathematics Rationale: There was widespread concern amongclinicians and researchers that clinical reality did notsupport DSM-IVʼs three independent learningdisorders. This is particularly important given thatmost children with specific learning disorder manifestdeficits in more than one area. By reclassifying these as a single disorder, separatespecifiers can be used to code the level of deficitspresent in each of the three areas for any person.Copyright 2013. American Psychiatric Association.
Attention-Deficit/Hyperactivity Disorder Age of onset was raised from 7 years to 12years Rationale: Numerous large-scale studies indicate that,in many cases, onset is not identified until after age 7years, when challenged by school requirements.Recall of onset is more accurate at 12 years.The symptom threshold for adults age 17 yearsand older was reduced to five Rationale: The reduction in symptom threshold was foradults only and was made based on longitudinal studiesshowing that patients tend to have fewer symptoms inadulthood than in childhood. This should result in aminimal increase in the prevalence of adult ADHD.Copyright 2013. American Psychiatric Association.
Schizophrenia(Schizophrenia Spectrum and Other Psychotic Disorders) Elimination of special treatment of bizarredelusions and “special” hallucinations inCriterion A (characteristic symptoms) Rationale: This was removed due to the poor reliabilityin distinguishing bizarre from non-bizarre delusions.At least one of two required symptoms to meetCriterion A must be delusions, hallucinations, ordisorganized speech Rationale: This will improve reliability and preventindividuals with only negative symptoms and catatoniafrom being diagnosed with schizophrenia.Copyright 2013. American Psychiatric Association.
Schizophrenia (contʼd) Deletionof specific subtypes Rationale:DSM-IVʼs subtypes were shownto have very poor reliability and validity. Theyalso failed to differentiate from one anotherbased on treatment response and course.Copyright 2013. American Psychiatric Association.
Schizoaffective Disorder Now based on the lifetime (rather thanepisodic) duration of illness in which the moodand psychotic symptoms described in CriterionA occur Rationale: The criteria in DSM-IV have demonstratedpoor reliability and clinical utility, in part because thelanguage in DSM-IV regarding the duration of illnessis ambiguous. This revision is consistent with thelanguage in schizophrenia and in mood episodes,which explicitly describe a longitudinal rather thanepisodic course. Similarly applying a longitudinalcourse to schizoaffective disorder will aid in itsdifferential diagnosis from these related disorders.Copyright 2013. American Psychiatric Association.
Catatonia Now exists as a specifier forneurodevelopmental, psychotic, mood andother mental disorders; as well as for othermedical disorders (catatonia due to anothermedical condition) Rationale:As represented in DSM-IV, catatonia wasunder-recognized, particularly in psychiatricdisorders other than schizophrenia and psychoticmood disorders and in other medical disorders. Itwas also apparent that inclusion of catatonia as aspecific condition that can apply more broadly acrossthe manual may help address gaps in the treatmentof catatonia.Copyright 2013. American Psychiatric Association.
Mania and Hypomania(Bipolar and Related Disorders) Inclusionof increased energy/activity as aCriterion A symptom of mania andhypomania Rationale:This will make explicit therequirement of increased energy/activity inorder to diagnose bipolar I or II disorder (whichis not required under DSM-IV) and will improvethe specificity of the diagnosis.Copyright 2013. American Psychiatric Association.
Mania and Hypomaniaepisode” is replaced with a “withmixed features” specifier for manic,hypomanic, and major depressiveepisodes “Mixed Rationale:DSM-IV criteria excluded fromdiagnosis the sizeable population ofindividuals with subthreshold mixed stateswho did not meet full criteria for majordepression and mania, and thus were lesslikely to receive treatment.Copyright 2013. American Psychiatric Association.
Mania and Hypomaniaanxious distress” also added as aspecifier for bipolar (and depressive)disorders “With Rationale:The co-occurrence of anxiety withdepression is one of the most commonly seencomorbidities in clinical populations. Additionof this specifier will allow clinicians to indicatethe presence of anxiety symptoms that are notreflected in the core criteria for depressionand mania but nonetheless may bemeaningful for treatment planning.Copyright 2013. American Psychiatric Association.
Bereavement Exclusion(Depressive Disorders) Eliminated(MDE)from major depressive episode Rationale:In some individuals, major loss –including but not limited to loss of a loved one –can lead to MDE or exacerbate pre-existingdepression. Individuals experiencing bothconditions can benefit from treatment but areexcluded from diagnosis under DSM-IV. Further,the 2-month timeframe required by DSM-IVsuggests an arbitrary time course tobereavement that is inaccurate. Lifting theexclusion alleviates both of these problems.Copyright 2013. American Psychiatric Association.
Disruptive Mood Dysregulation Disorder(DMDD) Newly added to DSM-5 Rationale: This addresses the disturbing increase inpediatric bipolar diagnoses over the past two decades,which is due in large part to the incorrectcharacterization of non-episodic irritability as a hallmarksymptom of mania. DMDD provides a diagnosis forchildren with extreme behavioral dyscontrol butpersistent, rather than episodic, irritability and reducesthe likelihood of such children being inappropriatelyprescribed antipsychotic medication. These criteria donot allow a dual diagnosis with oppositional-defiantdisorder (ODD) or intermittent explosive disorder (IED),but it can be diagnosed with conduct disorder (CD).Children who meet criteria for DMDD and ODD wouldbe diagnosed with DMDD only.Copyright 2013. American Psychiatric Association.
Atleast age 6 Onset by age 10 1 year of symptoms 3 temper outbursts per week Mood between temper outbursts isangry/irritable most of the time
Anxiety Disorders Separationof DSM-IV Anxiety Disorderschapter into four distinct chapters Rationale:Data from neuroscience,neuroimaging, and genetic studies suggestdifferences in the heritability, risk, course, andtreatment response among fear-based anxietydisorders (e.g., phobias); disorders ofobsessions or compulsions (e.g., OCD);trauma-related anxiety disorders (e.g., PTSD);and dissociative disorders. Thus, four anxietyrelated classifications are present in DSM-5,instead of two chapters in DSM-IV.Copyright 2013. American Psychiatric Association.
Panic Attacks Specifier Nowa specifier for any mental disorder Rationale:Panic attacks can predict the onsetseverity and course of mental disorders,including anxiety disorders, bipolar disorder,dep
DSM-5 Development DSM-5 Task Force (appointed 2006-2007) Work group chairs Health professionals from stakeholder groups DSM-5 Work Groups (appointed 2007-2008) Members work in specific diagnostic areas (e.g., Mood Disorders, Anxiety Disorder, etc.) Advisors