Transcription
BREAKING THE CYCLE OF NEGLECT:REDUCING THE ECONOMIC ANDSOCIETAL BURDEN OF PARASITICWORMS IN SUB-SAHARAN AFRICASponsored by
The world leader in global business intelligenceThe Economist Intelligence Unit (The EIU) is the research and analysis division of The Economist Group, the sister companyto The Economist newspaper. Created in 1946, we have over 70 years’ experience in helping businesses, financial firmsand governments to understand how the world is changing and how that creates opportunities to be seized and risks to bemanaged.Given that many of the issues facing the world have an international (if not global) dimension, The EIU is ideally positioned tobe commentator, interpreter and forecaster on the phenomenon of globalisation as it gathers pace and impact.EIU subscription servicesThe world’s leading organisations rely on our subscription services for data, analysis and forecasts to keep them informedabout what is happening around the world. We specialise in: Country Analysis: Access to regular, detailed country-specific economic and political forecasts, as well asassessments of the business and regulatory environments in different markets. Risk Analysis: Our risk services identify actual and potential threats around the world and help our clients understandthe implications for their organisations. Industry Analysis: Five year forecasts, analysis of key themes and news analysis for six key industries in 60 majoreconomies. These forecasts are based on the latest data and in-depth analysis of industry trends.EIU ConsultingEIU Consulting is a bespoke service designed to provide solutions specific to our customers’ needs. We specialise in these keysectors: Healthcare: Together with our two specialised consultancies, Bazian and Clearstate, The EIU helps healthcareorganisations build and maintain successful and sustainable businesses across the healthcare ecosystem. Find outmore at: eiu.com/healthcare Public Policy: Trusted by the sector’s most influential stakeholders, our global public policy practice providesevidence- based research for policy-makers and stakeholders seeking clear and measurable outcomes. Find out moreat: eiu.com/publicpolicyThe Economist Corporate NetworkThe Economist Corporate Network (ECN) is The Economist Group’s advisory service for organisational leaders seeking tobetter understand the economic and business environments of global markets. Delivering independent, thought-provokingcontent, ECN provides clients with the knowledge, insight, and interaction that support better-informed strategies anddecisions.The Network is part of The Economist Intelligence Unit and is led by experts with in-depth understanding of the geographiesand markets they oversee. The Network’s membership-based operations cover Asia-Pacific, the Middle East, and Africa.Through a distinctive blend of interactive conferences, specially designed events, C-suite discussions, member briefings, andhigh-calibre research, The Economist Corporate Network delivers a range of macro (global, regional, national, and territorial)as well as industry-focused analysis on prevailing conditions and forecast trends.Cover Image – Getty Images
Breaking the cycle of neglect: Reducing the economic andsocietal burden of parasitic worms in sub-Saharan AfricaContents2Executive summary4Introduction10 Epidemiological burden13 Strategies for NTD control22 The economic benefits of elimination26 Conclusion: the way forward33 Appendices42 Ethiopia Country Profile50 Kenya Country Profile58 Rwanda Country Profile67 Zimbabwe Country Profile The Economist Intelligence Unit Limited 20201
2Breaking the cycle of neglect: Reducing the economic andsocietal burden of parasitic worms in sub-Saharan AfricaExecutive summaryNeglected tropical diseases cause an annual loss of 17 millionhealthy life years globally, with 40% of these lost in sub-SaharanAfrica Neglected tropical diseases (NTDs) are a heterogeneous groupof mostly infectious diseases that largely affect poor individualsliving in low- and middle-income countries. The World HealthOrganisation (WHO) report that globally over 1.76bn peoplestill require interventions against NTDs. Over a quarter of thoseaffected live in sub-Saharan Africa.Schistosomiasis and soil-transmitted helminthiasis are the mostprevalent neglected tropical diseases in sub-Saharan Africa The majority (86%) of global schistosomiasis cases occur in subSaharan Africa, and 26% of soil-transmitted helminthiasis cases.The two diseases caused a loss of about 2.1m healthy life yearsin 2017. The ill health caused by these diseases hampers adults’ability to work, and could adversely impact children’s schooling.Eliminating morbidity and mortality from schistosomiasis andsoil-transmitted helminthiasis in Ethiopia, Kenya, Rwanda andZimbabwe by 2030 could boost these countries’ GDP by US 5.1bnin purchasing power parity (PPP) terms by 2040 The most recent WHO roadmap for neglected tropical diseasessets targets for the elimination of both schistosomiasis andsoil-transmitted helminthiasis as public health problems by2030. Once this is achieved, the countries will need to eliminatetransmission to stop these diseases returning. The EIU has modelled the economic impact of eliminatingmorbidity and mortality from these diseases by 2030 andpreventing their resurgence, compared with a scenario whereefforts to combat them stagnate, and cases increase withpopulation growth. We focus on four sub-Saharan Africancountries—Ethiopia, Kenya, Rwanda and Zimbabwe. Our analysis finds that this could boost productivity by US 5.1bn(PPP) between 2021 and 2040 across Ethiopia, Kenya, Rwandaand Zimbabwe. The greatest potential gains are seen in Ethiopiaat US 3.2bn, followed by Kenya (US 1.3bn), Rwanda (US 0.4bn),and Zimbabwe (US 0.3bn; all figures at PPP). The Economist Intelligence Unit Limited 2020
Breaking the cycle of neglect: Reducing the economic andsocietal burden of parasitic worms in sub-Saharan Africa In addition, eliminating the ill health associated with theseparasitic worms among school-age children in these countriescould improve their ability to learn and attend school. Ourestimates suggest that this could potentially benefit thesechildren by US 1.2bn (PPP) in extra wages between 2021 and2040 once they enter the workforce.Continued multi-sectoral action is needed to successfullyeliminate these diseases Achieving these targets will require concerted action, includingbetter disease mapping data, tailoring to the local context,integration with wider public health efforts and programmes toimprove sanitation. Progress towards the targets could be threatened, particularlyas the covid-19 pandemic heaps pressure on health systemsand economies. As countries approach elimination and casenumbers drop, it is also important to maintain momentum toensure sustainable elimination of these diseases. The Economist Intelligence Unit Limited 20203
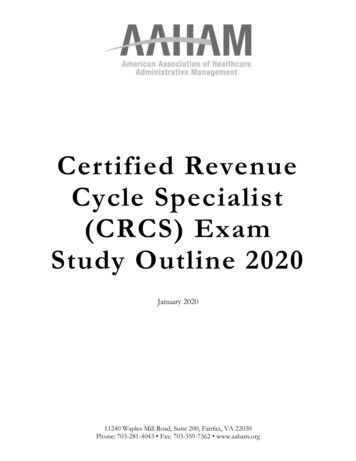
4Breaking the cycle of neglect: Reducing the economic andsocietal burden of parasitic worms in sub-Saharan AfricaIntroductionWhat are the neglected tropicaldiseases?Neglected tropical diseases (NTDs) are adiverse group of diseases, most of which arecommunicable and caused by a wide variety ofpathogens, which exist in 149 countries.1NTDs are widely known to affect populationsof lower socioeconomic status. They are themost common group of diseases among the2.7bn people worldwide who live on less thanUS 2 a day.2 NTDs are known to thrive in areasthat lack clean water and proper sanitation,which are often in rural and remote regions.3The populations who experience thesediseases most acutely are the least equippedto advocate for improvements to theirsituation. At the same time, governments havehistorically been less willing to address NTDsbecause other notable infectious diseases(such as HIV and malaria) cause more deathsand have therefore been higher on the agenda. The Economist Intelligence Unit Limited 2020If a community has a high burdenof worms, it is a marker of povertyand poor access to healthcareand [water, sanitation andhygiene]. Universal Health Care isunlikely to be in place if there arecommunities that have high wormburdens.Dr Simon Brooker, Deputy Director, NTDs atthe Bill & Melinda Gates Foundation
Breaking the cycle of neglect: Reducing the economic andsocietal burden of parasitic worms in sub-Saharan AfricaFigure 1: NTDs collocate with poverty4, 5NTD burden per thousand inhabitantsDisability-adjusted life years (DALYs), 2017 0.10.5-1.493-4.496-7.490.1-0.491.5-2.994.5-5.99 7.5No dataGDP per capitathousand US , 2017 208-9.94-5.91-1.910-19.96-7.92-3.9 1No data The Economist Intelligence Unit Limited 20205
6Breaking the cycle of neglect: Reducing the economic andsocietal burden of parasitic worms in sub-Saharan AfricaIn 2012 the WHO launched its Roadmap onAccelerating Work to Overcome the GlobalImpact of NTDs, in which it classified 17diseases as NTDs, with a further three addedto the list in 2017 (see Box 1).6The WHO’s list of NTDs reflects the diversityof this category of diseases. It includes a rangeof vector-borne diseases such as rabies anddengue, as well as parasitic worm infectionssuch as schistosomiasis, diseases causedby other pathogens, and even snakebiteenvenoming.Box 1: NTDs included in the WHO’s Roadmap grouped by typeParasitic wormsEchinococcosis / hydatidosisDracunculiasis (Guinea worm)Lymphatic itted helminthiasisTaeniasis/cysticercosisFoodborne trematodiasisOther (added 2017)Chromoblastomycosis and otherdeep mycosesScabies and other ectoparasitesSnakebite envenomingProtozoalChagas diseaseVisceral leishmaniasisCutaneous leishmaniasisHuman African trypanosomiasisBacteriaViralDengueRabies The Economist Intelligence Unit Limited 2020Buruli ulcerTrachomaLeprosyEndemic treponematoses (yaws)
Breaking the cycle of neglect: Reducing the economic andsocietal burden of parasitic worms in sub-Saharan AfricaGlobally the impact of NTDs remainsconsiderable, with the WHO estimating that atleast 1.76bn people still require interventionsto treat them.7 Data from the Global Burdenof Disease (GBD) study for 2017 suggest thatover a quarter of people with NTDs live insub-Saharan Africa.5 These diseases cause theloss of 6.7m healthy life years in sub-SaharanAfrica alone, almost 40% of the global total17m healthy life years lost (based on NTDslisted in the WHO roadmap and present in theGBD data).5NTDs are most common in tropical andsubtropical areas, where other environmentalfactors such as climate change could drasticallyincrease transmission rates.8 NTDs are linkedto socioeconomic status in two ways: theyaffect individuals of low socioeconomicstatus and they impair the socioeconomicdevelopment of affected communities.The influence of NTDs on global health ishighlighted by the inclusion of their eliminationby 2030 as part of the UN’s SustainableDevelopment Goals (Goal 3.3).There has been increased focus on NTDssince the launch of the WHO Roadmap onNeglected Tropical Diseases 2012-20, althoughthe burden of NTDs has been examinedglobally since at least 1947.9 The aim of theWHO roadmap was to achieve the eliminationof these NTDs or their reduction to a statewhere they were no longer considered a publichealth problem.Inspired by the WHO’s 2012 roadmap, theLondon Declaration on Neglected TropicalDiseases was created in order to focus oncontrol and elimination of ten selectedNTDs by 2020.10 The Declaration formalisedcommitments made by a wide variety ofpartners, including numerous NGOs, nationalgovernments, pharmaceutical companies andother entities. It included commitments fromdrug companies to donate the drugs needed tocombat NTDs. The Declaration, which reflectslongstanding and successful public-privatepartnerships to achieve the common goal ofNTD elimination, has contributed substantiallyto reducing the burden of NTDs around theworld.There has been progress since the 2012-20roadmap was published: 500m fewer peopleneed treatment for NTDs now than in 2010,and 40 countries or areas have eliminated atleast one NTD.7 However, not all of the 2020targets will be met.An updated WHO NTD Roadmap to cover2021-30, including revised targets for theindividual NTDs, is awaiting final approvalfrom the World Health Assembly.7 Renewalof the London Declaration commitments islikely to be needed to achieve the revisedtargets. The current covid-19 pandemiccould threaten progress, as it puts a strain onnational economies, health systems and thehealthcare industry, including pharmaceuticalcompanies who donate drugs. In April 2020WHO guidance recommended that, giventhe findings of pandemic community-basedsurveys, active case-finding activities and masstreatment campaigns for NTDs be postponeduntil further notice.11 The WHO updated theirguidance in July 2020 to outline a risk-benefitassessment framework which countries canuse to decide whether planned NTD activitiesshould go ahead as the pandemic evolvesand risks change. The guidance also describesgeneral precautionary measures for countriesto follow as they slowly begin to resume NTDactivities. 12 The Economist Intelligence Unit Limited 20207
8Breaking the cycle of neglect: Reducing the economic andsocietal burden of parasitic worms in sub-Saharan AfricaThe International Monetary Fund (IMF) haspredicted that global economies will contractby 4.9% in 2020, with those in sub-SaharanAfrica shrinking by 3.2%.13 The EIU predictshealthcare spending in US dollar termswill reduce by 2.9% in the Middle East andAfrica in 2020, before increasing by 3.4%in 2021.14 Although this increase in healthexpenditure may sound positive, the costof covid-19 treatments and vaccines (if andwhen they come onto the market) is likelyto put additional strain on already stretchedhealthcare budgets.NTDs in sub-Saharan AfricaThe subset of NTDs with the greatest impactin sub-Saharan Africa—in terms of populationaffected and as a key cause of disability andillness—are parasitic worm infections (seeBox 1 and Table 1). Among the parasitic worminfections, soil-transmitted helminthiasis(STH—a group of infections includinghookworm disease, ascariasis and trichuriasis)and schistosomiasis are the most widespreadNTDs across the region.15 The Economist Intelligence Unit Limited 2020Fragmented data collection has made gettingaccurate portrayals of the prevalence andtransmission trends in the region challenging.Effective prevention and control strategiesdepend on systematic surveillance, which hasbeen a problem across the African continent.16 17This report quantifies the economic impactof parasitic worm infections in sub-SaharanAfrica, as well as describing the contextand some of the challenges involved intheir elimination. The analysis focuses onthe most prevalent infections—STH andschistosomiasis—in four countries—Ethiopia,Kenya, Rwanda and Zimbabwe. Thesecountries provide a cross-section of thecountries within the region, with varyingpopulation size, size and growth of economy,healthcare spending, and political stability.
Breaking the cycle of neglect: Reducing the economic andsocietal burden of parasitic worms in sub-Saharan AfricaTable 1: Burden of the most prevalent NTDs in sub-Saharan Africa 20175(in order of estimated number of people infected).DiseaseEstimated populationinfectedEstimated % ofpopulation affected(age-standardised)Healthy life years .9mHookworm ic m0.04%0.08mLeprosy0.1m0.01%0.002mNote: DALY disability-adjusted life year The Economist Intelligence Unit Limited 20209
10Breaking the cycle of neglect: Reducing the economic andsocietal burden of parasitic worms in sub-Saharan AfricaEpidemiological burdenThis report focuses on schistosomiasis as wellas STH (hookworm disease, ascariasis andtrichuriasis) because of the significant burdenthese parasitic worms pose. Though they areboth treatable and preventable these wormscause a loss of nearly 2.1m healthy life years,primarily through causing ill health rather thandeath.5In 2017 schistosomiasis and STH affected morepeople in sub-Saharan Africa than any otherNTD, although cases of these diseases havebeen decreasing.5 The region accounts for86% of the global burden of schistosomiasiscases and 26% of STH (ranging from 15%of trichuriasis to 51% of hookworm diseasecases).Although these diseases lead to a multitudeof morbidities, their symptoms can be nonspecific and not visible, as is the case withsome other NTDs. As a result, individuals whoare infected often do not realise that they areinfected until symptoms become severe, anddoctors have difficulty diagnosing the diseasesowing to their non-specific symptoms. Thisresults in a vicious cycle that, in combinationwith poor sanitation and lack of educationabout these diseases, allows them to spread.As WHO technical director Pauline Mwinziputs it, “We have to go to great lengths togive morbidity data visibility. When you showschistosomiasis and STH patients, the majoritywill appear physically normal. Surveys have tobe implemented that show morbidity data.” The Economist Intelligence Unit Limited 2020SchistosomiasisSchistosomiasis, a chronic disease linked topoverty, is widely endemic, particularly insub-Saharan Africa.18 It is transmitted throughcontact with water that is contaminated withschistosome larvae. The two major forms ofthe disease are intestinal and urogenital, andinfected individuals pass schistosome eggs intheir faeces and/or urine. If they get into thewater system, the eggs hatch and infect watersnails, which later release schistosome larvaeinto the water, beginning the cycle again.Risk factors for the transmission of the diseaseinclude a region’s proximity to bodies of water,including irrigation and dams, as well as aperson’s occupation and socioeconomic status.19Climate change also impacts regional risk.The symptoms of chronic and advancedschistosomiasis include abdominal pain,diarrhoea, anaemia, blood in the stool,liver cirrhosis, high blood pressure in thevein leading from the intestine to the liver(portal hypertension), collection of fluidin the abdomen (ascites), pain or difficultyin urination, and bladder abnormalities.20Schistosomiasis can also cause prematuredeath.Schistosomiasis can also have negative effectson a child’s development, the outcome ofpregnancy and agricultural productivity, whichis why infection contributes to the “bottom500m” inhabitants of sub-Saharan Africacontinuing to live in poverty.19
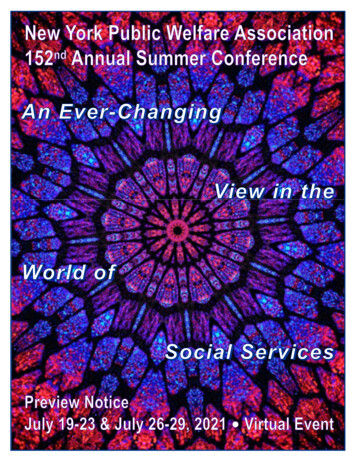
Breaking the cycle of neglect: Reducing the economic andsocietal burden of parasitic worms in sub-Saharan AfricaFigure 2: Trends in the age-standardised % prevalence of schistosomiasis and STHin sub-Saharan Africa, weSub-Saharan ed n 5200720092011 The Economist Intelligence Unit Limited 202011
12Breaking the cycle of neglect: Reducing the economic andsocietal burden of parasitic worms in sub-Saharan AfricaThe risk of infection has been decreasing since2000 owing to control efforts (see Figure 2),but estimates suggest that 123m people insub-Saharan Africa are still infected withschistosomiasis (about 86% of infectionsglobally), causing the loss of about 1.2mDALYs in 2017.5 However, underestimationof disease burden is a major problem withschistosomiasis, owing to a lack of knowledgeof the symptoms of the disease.19In terms of age breakdown in sub-SaharanAfrica, schistosomiasis is least prevalent inthe under-fives, and gradually increases withage until it peaks in the 30-49 age group.5Rates of schistosomiasis are higher in menthan women, which may reflect occupationalhazards among more male-dominated groupssuch as fishermen.Soil-transmitted helminthiasis (STH)STH in humans is most often causedby roundworms (Ascaris lumbricoides),whipworms (Trichuris trichiura) andhookworms (Necator americanus orAncylostoma duodenale). People becomeinfected when they come into contact withthe larvae of these worms through touchingsoil, human faeces or water that has beencontaminated with the parasites’ eggs.21 Onceinfected, people pass eggs in their faeces. Ifthis is allowed to contaminate soil or water,the cycle can continue. Therefore, as withschistosomiasis, STH is associated with poorsanitation.These intestinal worms can cause malnutrition,anaemia, stunting, impaired intellectual The Economist Intelligence Unit Limited 2020development and susceptibility to otherinfectious diseases such as HIV. Ascariasis isthe only STH that can lead to premature death.Over 4.5bn people around the world are atrisk of STH infection, but there is an unevendistribution of the disease globally.22 STHdisproportionately affects populations whoare typically marginalised and low-income, asevidenced by the fact that over 1bn people inresource-constrained areas of sub-SaharanAfrica, Asia and the Americas are infected withat least one helminth.22 Often individuals inthese settings can be infected by more thanone type of worm (polyparasitism), which canlead to higher rates of morbidity.22The prevalence of STH among school-agechildren in sub-Saharan Africa decreased from43.3% to 25.9% in 2017, representing a 40%reduction in this period.5 This reduction is theproduct of an increased focus on large-scaledeworming programmes, as well as an increasein socioeconomic development.15In 2017 about 235m people in sub-SaharanAfrica had STH, about 26% of the global total.5However, the region accounts for 45% of theDALYs (0.9m) associated with these diseasesglobally.There is less of an age gradient in STHprevalence in sub-Saharan Africa than forschistosomiasis. The lowest prevalence forSTH is in under-fives, but the rates are still high(16% of the age group affected). Rates thenincrease sharply in the 5-9 year old age group(27% affected) and reach a peak in the 15-24age group (with about 29% of this age groupaffected).
Breaking the cycle of neglect: Reducing the economic andsocietal burden of parasitic worms in sub-Saharan AfricaStrategies for NTD controlPolicy contextAs well as its global NTD roadmap for 2012-20,the WHO created a regional strategic plan forNTD control in Africa, setting out five targetsfor 2014-20:1. to eradicate dracunculiasis and yaws in allcountries of the region;2. to sustain elimination of leprosy andfurther reduce severe leprosy disabilities;3. monitoring the progress of controlinterventions and quantifying changes inincidence of infection and disease;4. assessing drug efficacy and promptlydetecting development of drug resistance;5. determining programme end-points (forelimination of infection);6. post-control surveillance; and3. to eliminate lymphatic filariasis,onchocerciasis, schistosomiasis andblinding trachoma;7. developing appropriate health researchpolicies and capacity building in diseaseendemic countries to provide conduciveenvironment and adequate expertise forsustained disease-control efforts.4. to control morbidity due to Buruliulcer, human African trypanosomiasis,leishmaniasis, soil-transmittedhelminthiasis and rabies in the region; andThe WHO has recently updated the 2012 NTDRoadmap to set ambitious goals for all NTDs,to be achieved in 2021-30.7 The overarchinggoals include:5. to prevent disabilities due to Buruli ulcer,leishmaniasis, leprosy, lymphatic filariasisand blinding trachoma.The regional objectives more broadly definethe strategy of NTD control. They includescaling up access to interventions and systemcapacity building; enhancing planning forresults, resource mobilisation and financialsustainability of national NTD programmes;strengthening advocacy, co-ordination andnational ownership; and enhancing monitoring,evaluation, surveillance and research.23As previously discussed, parasitic worminfections represent a significant proportionof NTDs, particularly in sub-Saharan Africa.The WHO Research Priorities for HelminthInfections identified the most importantstrategies in the reduction of parasitic worminfections worldwide in 2012: 241. updated disease prevalence maps; 90% fewer people requiringinterventions against NTDs; 75% fewer NTD-related DALYs; 100 countries having eliminated at leastone NTD; and two NTDs eradicated (dracunculiasisand yaws).The WHO has also set specific targets for eachof the NTDs. The goal for schistosomiasis iselimination of the disease as a public healthproblem in 100% of endemic countries.Similarly, the WHO targets elimination of STHas a public health problem for 96% of endemiccountries. Elimination as a public healthproblem is defined as reducing the burden ofa disease to specified levels of moderate and/or heavy-intensity infections (under 1% forschistosomiasis and under 2% for STH).2. more sensitive diagnostics; The Economist Intelligence Unit Limited 202013
14Breaking the cycle of neglect: Reducing the economic andsocietal burden of parasitic worms in sub-Saharan AfricaModelling for schistosomiasis has shownthat if treatment is stopped after achievingelimination as a public health problem there ishighly likely to be a resurgence in infections.25The same is likely to be true for otherinfectious NTDs. Therefore once elimination asa public health problem is achieved, countrieswill need to continue treatments to achieveinterruption of transmission, where newinfections would be reduced to zero, withminimal chance of reintroduction, reducing theneed for ongoing treatment.NTD control programmesIn 2003 the WHO began to shift the focusaway from specific disease treatment andinstead began focusing on the health needs ofpopulations experiencing NTDs at the highestrates.6 The two major interventions that cameout of this new way of thinking about NTDcontrol were preventive chemotherapy andintensified disease management. The five mainstrategies recommended by the WHO6 forNTD control programmes are: preventive chemotherapy; intensified disease management; vector and intermediate host control; veterinary public health at the humananimal interface; and the provision of safe water, sanitationand hygiene.Preventive chemotherapy treatmentFive NTDs can be managed usingpreventive chemotherapy treatment (PCT):schistosomiasis, STH, onchocerciasis,lymphatic filariasis and trachoma (all excepttrachoma are caused by parasitic worms). TheWHO provides recommendations for PCT forthese NTDs (see Table 2).26Most commonly this form of treatment is giventhrough mass drug administration (MDA) toat-risk individuals in endemic areas.22 MDAuses two primary methods to reach affectedcommunities: community-based distributionis carried out through static distribution pointsor delivering medicine door-to-door, whileschool-based distribution happens at schoolsand is specifically directed at school-agechildren. Both MDA methods are not relianton a diagnosis prior to delivering medicine. InMDA programmes coverage of treatment forschool-age children is often reported as themain indicator of programme success.Historically, MDA (also referred to asdeworming) programmes have not beenintegrated into the health system, but ratherrun parallel to activities of the health sector.These are vertical programmes involvingpharmaceutical companies donatingmedications to the government, with theWHO overseeing the donation programmes.Co-ordination and dissemination are organisedat the national level in order to deliver themedications to at-risk populations (most oftenschool-age children).The WHO has promoted mass dewormingprogrammes for years, but in 2017 the WHO’sGuideline Review Committee solidified theimportance of PCT by issuing a guideline The Economist Intelligence Unit Limited 2020
Breaking the cycle of neglect: Reducing the economic andsocietal burden of parasitic worms in sub-Saharan AfricaTable 2: NTDs targeted by preventive chemotherapy6DiseaseTreatmentTarget populationMinimumeffectivecoverageFrequency and duration ofinterventionLymphaticfilariasisAlbendazole withivermectin or withdiethylcarbamazinecitrateIvermectin: age 5 yearsDiethlycarbamazine: age 2 years65%Annually for at least 5 yearsOnchocerciasisIvermectin Age 5 years80%Annually for at least 10-15yearsSchistosomiasisPraziquantelSchool-age children (SAC,ages 5-14 years) and atrisk adults75%Once a year, or every two tothree years, depending oncommunity prevalence, forvariable e-SAC ( age 5 years)and SAC (age 5-14 years)75%Once or twice a year,depending on communityprevalence, for variabledurationTrachomaAzithromycin (givenas part of a SAFEstrategy) Age 6 months80%Annually, with the number ofrounds given before reviewdependent on the prevalenceof disease at last estimateMebendazolestating that “deworming improves the healthand nutrient uptake of heavily infectedchildren.”27 Givewell, an organisation thatassesses the cost-effectiveness of differenttypes of interventions funded by charitiesand donors, notes that cost-effectivenesscalculations are problematic owing toweaker evidence of impact on health andlife outcomes. However, Givewell includesdeworming for schistosomiasis and STH inits priority programme list. The organisationestimates that the cost-effectiveness ofdeworming for these two NTDs is on a parwith that of its other priority programmes suchas malaria treatment programmes, certainimmunisation campaigns and Vitamin Asupplementation.28Schistosomiasis treatmentPraziquantel is the only drug that the WHOrecommends for the treatment of bothurogenital and intestinal schistosomiasis,which many are worried could lead to drugresistance.29 Praziquantel costs around 0.08per tablet, and it is estimated that around70m children at
The Economist Intelligence Unit (The EIU) is the research and analysis division of The Economist Group, the sister company to The Economist newspaper. Created in 1946, we have over 70 years’ experience in helping businesse