Transcription
Alongside the development of national and international guidelines forthe management of rheumatic disorders, there has been a huge growthin the availability of new therapies. This book summarises diagnosis andpatient management based around the latest guidelines and expandedtreatment options, including the scientific rationale upon which thesetreatments are based.To aid understanding, the book: features real case histories to illustrate the range of clinicalpresentations and how these can be managed covers all common rheumatic disorders, from rheumatoidarthritis through crystal arthropathies to fibromyalgia andchronic pain conditions includes a dedicated chapter on paediatric rheumatology provides advice on physiotherapy, including links torecommended video demonstrationsThe book is written for clinicians, nurses and physiotherapists working inmusculoskeletal medicine, in addition to GPs, and doctors preparing forthe Specialist Certificate Examination in rheumatology.Also availableISBN 978-1-911-510-64-29 781911 510642Rheumatology cover 234x153 11.5mm.indd All PagesSofat, Rutter-Locher & Oakleywww.scionpublishing.comRheumatology: a case-based approach to managementRheumatology: a case-based approach to managementRheumatologya case-basedapproach tomanagementNidhi Sofat,Zoe Rutter-Locher& Helen Oakley29/01/2021 13:04
Rheumatologya case-basedapproach tomanagementRheumatology A CBA to Management.indb 11/19/2021 5:30:52 PM
Rheumatology A CBA to Management.indb 21/19/2021 5:30:52 PM
RheumatologyNidhi SofatBSc, MBBS, PhD, PGCert, FHEA, FRCPProfessor of Rheumatology, St George’s,University of LondonSt George’s University Hospitals NHS Trusta case-basedapproach tomanagementZoe Rutter-LocherBSc, MBBS, MRCP, PGCert, MScRheumatology Trainee RegistrarGuy’s and St Thomas’ NHS TrustHelen OakleyBSc, MCSPAdvanced Physiotherapy PractitionerPhysiotherapy Department, St George’s University Hospitals NHS TrustRheumatology A CBA to Management.indb 31/19/2021 5:30:52 PM
Scion Publishing Ltd, 2021ISBN 9781911510642First published 2021All rights reserved. No part of this book may be reproduced or transmitted, in any formor by any means, without permission.A CIP catalogue record for this book is available from the British Library.Scion Publishing LimitedThe Old Hayloft, Vantage Business Park, Bloxham Road, Banbury OX16 9UX, UKwww.scionpublishing.comImportant Note from the PublisherThe information contained within this book was obtained by Scion Publishing Ltd fromsources believed by us to be reliable. However, while every effort has been made to ensureits accuracy, no responsibility for loss or injury whatsoever occasioned to any person actingor refraining from action as a result of information contained herein can be accepted by theauthors or publishers.Readers are reminded that medicine is a constantly evolving science and while the authorsand publishers have ensured that all dosages, applications and practices are based oncurrent indications, there may be specific practices which differ between communities. Youshould always follow the guidelines laid down by the manufacturers of specific productsand the relevant authorities in the country in which you are practising.Although every effort has been made to ensure that all owners of copyright materialhave been acknowledged in this publication, we would be pleased to acknowledge insubsequent reprints or editions any omissions brought to our attention.Registered names, trademarks, etc. used in this book, even when not marked as such, arenot to be considered unprotected by law.Typeset by Medlar Publishing Solutions Pvt Ltd, IndiaCover design by Andrew Magee DesignPrinted in the UKLast digit is the print number: 10 9 8 7 6 5 4 3 2 1Rheumatology A CBA to Management.indb 41/19/2021 5:30:52 PM
ContentsPreface . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . viiAbbreviations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . ix1. Rheumatoid arthritis . . . . . . . . . . . . . . . . . . . . . . . 12. Connective tissue disease . . . . . . . . . . . . . . . . . . . . 253. Crystal arthropathies . . . . . . . . . . . . . . . . . . . . . . 594. Psoriatic arthritis . . . . . . . . . . . . . . . . . . . . . . . . 755. Ankylosing spondylitis . . . . . . . . . . . . . . . . . . . . . 896. Vasculitis . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1037. Osteoarthritis . . . . . . . . . . . . . . . . . . . . . . . . . . 1218. Osteoporosis . . . . . . . . . . . . . . . . . . . . . . . . . . 1379. Chronic pain disorders . . . . . . . . . . . . . . . . . . . . 15710. Soft tissue disorders . . . . . . . . . . . . . . . . . . . . . . 16911. Paediatric rheumatology . . . . . . . . . . . . . . . . . . . 183Appendix . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 193Index . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 197vRheumatology A CBA to Management.indb 51/19/2021 5:30:52 PM
Rheumatology A CBA to Management.indb 61/19/2021 5:30:52 PM
PrefaceDuring the 20 years I have spent working within Rheumatology as aClinician and Researcher, the specialty has undergone rapid changes.In many conditions this has led to earlier diagnosis and treatment ofdiseases which span this multisystem discipline of medicine.As a teacher and trainer, I was approached by medical students,doctors-in-training, nurses, pharmacists, physiotherapists andoccupational therapists, who attended my lectures at St George’s,University of London. They all expressed a desire to understandthe multidisciplinary management of patients living withrheumatological conditions through worked examples. Learnersare often overwhelmed by the diagnostic criteria for rheumaticconditions, many of which have recently undergone review.In addition, the huge growth in disease-modifying therapies,including synthetic disease-modifying antirheumatic drugs(DMARDs) and biologic drugs can seem daunting to learners newto the field.To address the unmet need of providing up-to-date summaries ofclinical diagnosis and management of the most common rheumaticconditions, I have written this book with my co-authors, ZoeRutter-Locher, a trainee in Rheumatology, and Helen Oakley, aphysiotherapist working in Musculoskeletal Medicine. Zoe’s inputhas been invaluable in identifying the questions that traineeswho are new to Rheumatology are likely to ask. Helen’s input asa physiotherapist has been crucial in explaining physiotherapy’scontribution to the multidisciplinary components of care that manypatients with rheumatic conditions require.viiRheumatology A CBA to Management.indb 71/19/2021 5:30:52 PM
P r e fac eThe book is divided into chapters which discuss each of the commonrheumatological conditions, their diagnosis, the most up-to-datediagnostic criteria and management, based on UK NICE (NationalInstitute of Health and Care Excellence) guidelines.Assessment is an important part of learning, so each chapter alsoincludes case histories discussing diagnosis and management, withdiscussion of answers provided for each case. References for NICEguidelines and further reading are also provided where appropriate.Finally, I would like to say that this book is intended to provide apractical guide and aide memoire, which can be carried on wardrounds, in clinics and GP surgeries, to provide a concise summaryof rheumatological conditions and their management.I dedicate this book to all our patients whom we are here to serve.Professor Nidhi SofatProfessor of RheumatologySt George’s, University of LondonviiiRheumatology A CBA to Management.indb 81/19/2021 5:30:52 PM
AbbreviationsA&EAccident and EmergencyACRAmerican College of RheumatologyALTalanine transaminaseANAantinuclear antibodyANCAanti-neutrophil cytoplasmic antibodyARMAArthritis and Musculoskeletal AllianceASankylosing spondylitisASASAssessment of SpondyloArthritis international SocietyASTaspartate aminotransferaseBASDAIBath Ankylosing Spondylitis Disease Activity IndexBESSBritish Elbow & Shoulder SocietyBMDbone mineral densityBMIbody mass indexBMLbone marrow lesionBNFBritish National FormularyBNPbrain natriuretic peptideBSRBritish Society of RheumatologyCBTcognitive behavioural therapyCKcreatine kinaseCMCcarpometacarpalCPGSChronic Pain Grade ScaleCPPcalcium pyrophosphateixRheumatology A CBA to Management.indb 91/19/2021 5:30:52 PM
A bbr e viationsCPPDcalcium pyrophosphate deposition diseaseCRPC-reactive proteinCRPScomplex regional pain syndromeCTcomputerised tomographyCXRchest X-rayDASDisease Activity ScoreDEXAdual energy X-ray absorptiometryDLCOdiffuse capacity of the lungs for carbon monoxideDMARDdisease-modifying antirheumatic drugdsDNAdouble-stranded DNAECGelectrocardiogramEDemergency departmenteGFRestimated glomerular filtration rateEGPAeosinophilic granulomatosis with polyangiitisELISAenzyme-linked immunosorbent assayEMGelectromyographyESRerythrocyte sedimentation rateEULAREuropean League Against RheumatismFBCfull blood countFDAFood and Drugs AdministrationFRAXfracture risk algorithmGCAgiant cell arteritisGIgastrointestinalGPgeneral practitionerGRACE indexGRAppa Composite score indexGWASgenome-wide association studiesHEp-2human epithelial type 2HGPRThypoxanthine-guanine phosphoribosyltransferaseHIVhuman immunodeficiency virusHRCThigh resolution computerised tomographyIAintra-articularxRheumatology A CBA to Management.indb 101/19/2021 5:30:52 PM
A bbr e viationsIIMidiopathic inflammatory myopathiesILDinterstitial lung diseaseIMintramuscularIVintravenousJAKJanus kinaseJIAjuvenile idiopathic arthritisLDHlactate dehydrogenaseLFTsliver function testsMALTmucosa-associated lymphoid tissueMASmacrophage activation syndromeMCPmetacarpophalangealMDTmultidisciplinary teamMGUSmultiple myeloma undetermined significanceMHCmajor histocompatibility complexMPOmyeloperoxidaseMSmultiple sclerosisMSUmonosodium urateMTPmetatarsophalangealNASSNational Axial Spondyloarthritis SocietyNICENational Institute for Health and Care ExcellenceNSAIDnon-steroidal anti-inflammatory drugNSIPnon-specific interstitial pneumoniaOAosteoarthritisPAHpulmonary arterial hypertensionPASDASPsoriatic ArthritiS Disease Activity ScorePASIPsoriasis Area and Severity IndexPETpositron emission tomographyPIPproximal interphalangealPMPpain management programmePOper os (by mouth)xiRheumatology A CBA to Management.indb 111/19/2021 5:30:52 PM
A bbr e viationsPPIproton pump inhibitorPRPplatelet-rich plasmaPRPPphosphoribosyl pyrophosphatePsApsoriatic arthritisPsARCPsoriatic Arthritis Response CriteriaPTHparathyroid hormoneRArheumatoid arthritisRANKreceptor activator of nuclear factor kappa-BRhFrheumatoid factorRS3PEremitting seronegative symmetrical synovitis withpitting oedemaSCsubcutaneousSLEsystemic lupus erythematosusSNRIserotonin–noradrenaline reuptake inhibitorSSRIselective serotonin reuptake inhibitorSTIRshort T1 inversion recoverySUAserum uric acidTBtuberculosisTCAtricyclic antidepressantTLRtoll-like receptorsTNFtumour necrosis factorTRPVtransient potential receptor vanilloidTSHthyroid-stimulating hormoneU Esurea and electrolytesUIPusual interstitial pneumoniaULTurate-lowering therapyUSultrasoundVASVisual Analog ScalexiiRheumatology A CBA to Management.indb 121/19/2021 5:30:52 PM
C H A P T E R404Psoriatic arthritis4.1IntroductionPsoriatic arthritis (PsA) is a condition with a prevalence of 10–30%of people affected by psoriasis. The prevalence of psoriasis of theskin is estimated at 2–3% in the general population. PsA can affect ayoung age range of people, with a peak onset from 30 up to 50 years.Arthritic involvement is usually preceded by psoriasis which affectsthe skin. Men tend to develop axial disease, with women developingperipheral joint involvement more frequently. Other factorsinfluencing the development of PsA include genetic susceptibilityand infection (Figure 4.1). Interestingly, some people with arthriticinvolvement may not have previously had significant cutaneousinvolvement. It is not fully understood why certain people withpsoriasis develop PsA.4.2DiagnosisSymptoms of PsA include joint stiffness, swelling, pain and fatigue.All the symptoms described can make day-to-day activities difficult,and cause pain and functional impairment. PsA can have seriouseffects on the skin and joints, resulting in a serious negative effect onpeople’s quality of life. PsA can affect people from a young age, andit can affect multiple aspects of people’s lives, including their familylife, relationships and career aspirations. The psychological impactof the condition is significant.75Rheumatology A CBA to Management.indb 751/19/2021 5:30:56 PM
C h ap t e r 4 : P so r iat ic a r t h r i t is4.2.1 Features of psoriatic arthritisJointsThere are different forms of joint involvement in psoriatic arthritis.Joint involvement can be limited to a few joints only, e.g. peripheralsmall joints of the hands, while in other cases there can be moreextensive involvement. Classically there are five different forms ofPsA involvement: Symmetric small joint involvement – this form is similar to anRA distribution Asymmetric large joint involvement – predominantly large jointsare involved in this form, e.g. knee or foot Peripheral small joint involvement – the distal interphalangealjoints are predominantly involved Axial spondyloarthritis – in this form there is mainly spinaldisease, with possible enthesitis, bone oedema and/or sacroiliitis Arthritis mutilans – this is a very severe form of the disease whichcan lead to complete destruction of the joint, with changes suchas telescoping of the fingers and severe loss of function.Psoriatic arthritis is typified by several other clinical features whichare not usually observed in other inflammatory arthritides suchas RA.More recently, it has been recommended that the diagnosis ofpsoriatic arthritis is made based on the CASPAR criteria, whichinclude the following:CASPAR criteria Inflammatory arthritic diseaseCurrent, personal or family history of psoriasisPsoriatic nail dystrophyNegative test for RhFDactylitis: current swelling of entire digit, or history of dactylitisRadiologic evidence of juxta-articular new bone formation.TendinitisInflammation of the tendons is a feature of PsA. Tendinopathies canoccur in any part of the body.76Rheumatology A CBA to Management.indb 761/19/2021 5:30:56 PM
4 . 2 : D ia g nosisEnthesitisThis is inflammation of the entheses, which is where ligaments ortendons insert into bones. The most frequent areas of enthesitisinclude the feet, the Achilles tendon, and attachments to the ribs,spine and pelvis. Over a longer period of time, ongoing enthesitiscan lead to fibrosis (or thickening of the enthesites), calcificationor ossification. Enthesitis is not usually observed in rheumatoidarthritis and osteoarthritis.DactylitisThis is commonly known as ‘sausage digits’, and is a result ofinflammation in the whole finger or toe. Dactylitis occurs whensmall joints and entheses of the surrounding tendons becomeinflamed. Dactylitis is a typical hallmark of PsA. It can involve a fewfingers or toes but is usually asymmetrical. PsA can affect differenttoes and fingers on either side.Skin and nailsPsoriatic skin changes are often typified by a scaly, maculopapularrash at the extensor surfaces of the body, e.g. elbows, hairline andumbilicus. In more severe cases, it can be increasingly widespreadand cover large areas of the body.The degree of skin involvement does not always correlate withthe extent of joint involvement. If there is severe skin disease thatrequires treatment with disease-modifying therapy, it is sometimespossible that skin and joints can be treated together with DMARDs.Nails can show features of ridging, pitting and onycholysis. Thesecan be found early and may be present in the absence of morewidespread cutaneous involvement.4.2.2 InvestigationsBlood testsPsoriatic arthritis is a seronegative arthritis, which means thatautoantibody screening is usually negative, including ANA, RhFand anti-CCP. The patient may have raised inflammatory markers,77Rheumatology A CBA to Management.indb 771/19/2021 5:30:56 PM
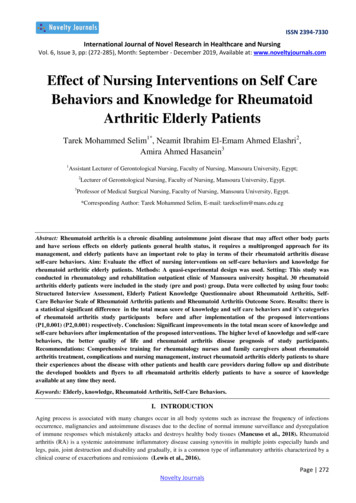
C h ap t e r 4 : P so r iat ic a r t h r i t isincluding ESR and CRP. The HLA-B27 tends to be negative in PsAand is a more prominent feature of ankylosing spondylitis.ImagingPlain radiographs may show erosions if the arthritis is establishedand there has been bone destruction. Ultrasound may be useful inabcdBone marrow oedemaSynovitisCoronal viewAxial viewFigure 4.1. Examples of radiographic changes observed in psoriaticarthritis(a) Plain radiographs of the hand showing erosions and joint space narrowingin distal interphalangeal joints, proximal interphalangeal joints andmetacarpophalangeal joints of both hands. The patient has had surgery in theleft thumb, right index and little fingers. There is also wrist involvement withfusion of the carpal bones in the left wrist and erosions in the right wrist. (b)Plain radiographs of the feet in the same patient as in part (a). There is boneloss, erosions and joint deviation as a result of long-term damage. (c) MRIscan of the knee in a patient with PsA of the knee. The T1 weighted imageshows synovitis as high signal on MRI, consistent with inflammation (greenarrow). (d) MRI scan of the knee in the same patient as in part (c). The axialview shows bone marrow oedema in the patella (green arrow).78Rheumatology A CBA to Management.indb 781/19/2021 5:30:56 PM
4 . 3 : C aus e sdemonstrating synovitis with increased power Doppler signal andearly erosions. Such changes may assist in supporting the need tocommence DMARDs. More recently, MRI has been used and canbe helpful in detecting enthesitis and also bone marrow oedema.Examples of imaging changes observed in PsA are summarised inFigure 4.1.4.3CausesRisk factors for PsA include genetics. Having a parent with psoriasistriples the chance of developing psoriasis. Figure 4.2 shows aPsoriatic skin diseaseGenetic susceptibilityEnvironmental riskfactors, e.g. infectionActivation of inflammatory pathways including cytokines systemicallyand in joint, leading to inflammation and damageDevelopment ofpsoriatic arthritis Inflammation mediated by cytokine activation, e.g. ne oedema, erosionLong-term sequelae Vascular disease Disability Social isolation Anxiety and depression Joint replacementFigure 4.2. The development of psoriatic arthritis79Rheumatology A CBA to Management.indb 791/19/2021 5:30:57 PM
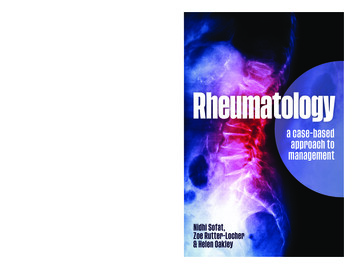
C h ap t e r 4 : P so r iat ic a r t h r i t issummary of the development of PsA. Epidemiology suggests thatthere is a strong genetic contribution in PsA. There are some geneticdifferences between people with skin and joint involvement. Codingvariants are described in TYK2 and TRAF3IP2, which are stronglyassociated with skin and joint disease. Some studies have focusedon biomarkers for PsA, showing that genomics and serologicalfactors may play a role in treatment response to TNF inhibitors.Infections such as streptococcal throat can also be associated withthe development of PsA.4.4ManagementThe treatment of PsA often involves a multidisciplinary approach,which includes treatment of the joint and skin, as well as physical,social and psychological factors.For skin, the extent of cutaneous involvement can be measured bythe Psoriasis Area and Severity Index (PASI), which is a compositescore of body surface area, erythema, induration, and scaling ofpsoriasis on different areas of the body (head, trunk, upper limbs,lower limbs). It is mainly used in clinical trials as it can takesignificant time to measure in clinic.A wide range of joints can be affected in PsA, therefore a scoringsystem needs to reflect that. In the clinic, patients are often shownmannequins to measure the extent of joint involvement when theyare assessed (Figure 4.3). The Psoriatic Arthritis Response Criteria(PsARC) score is used quite extensively in clinical settings, with thenumber of tender and swollen joints recorded and used with a rangeof scoring from 1 (mild disease) to 5 (severe disease).Recently, clinical trials are including a range of disease activityscores in psoriatic arthritis, among them the Psoriatic ArthritiSDisease Activity Score (PASDAS), the GRAppa Composite score(GRACE index) and the Composite Psoriatic Disease Activity Index(CPDAI).80Rheumatology A CBA to Management.indb 801/19/2021 5:30:57 PM
4 . 4 : M ana g e m e n tJawCollarbone jointNeckShoulderElbowSI joint (connection of pelvis to spine)WristKnuckleMiddle phalanxDistal phalanxKneeHipAnkleToesFigure 4.3. Example of mannequin used to assess joints in psoriaticarthritis4.4.1 Non-pharmacological therapiesPhysiotherapy has a role to play in strengthening joint structures andhelping to maintain function. People may also require occupationaltherapy, e.g. for hand supports and splinting, and psychologicalsupport may be needed in cases where the mental health impact ofpsoriasis and arthritis plays a part.4.4.2 Pharmacological managementA summary of the principles of pharmacological management inPsA is given in Table 4.1.81Rheumatology A CBA to Management.indb 811/19/2021 5:30:57 PM
Formulation and dosePO/SCTypically 15–25mgweeklyPOTypically 2–3g dailyPOTypically 20mg dailyafter loading dosePOUp to 400mg daily individed dosesPO/IM/IA/topicalPOUp to 30mg twice dailyIV0-, 2-, 6- then 8-weekly40mg SC every 2 atology A CBA to Management.indb 82HydroxychloroquineCorticosteroids, e.g.prednisoloneApremilastInfliximab (Remicade/Remsima biosimilar)Adalimumab (Humira)Humanised anti-TNFmonoclonal antibodyChimeric anti-TNFmonoclonal antibodyPhosphodiesterase 4(PDE4) inhibitorWorks throughmultiple pathwaysincluding increasedtranscription of antiinflammatory genesInhibition ofexpression of TNF andother cytokinesInhibition ofpyrimidine synthesisInhibition ofexpression of TNF andother cytokinesInhibition of purinesynthesisMechanism ofactionNICE TA1992nd lineNICE TA1992nd lineNICE TA4331st to 2nd line1st line1st line1st line1st line1st lineUsual level oftherapy (NICEguidelines)Hepatitis B & C, HIV, TBHepatitis B & C, HIV, TBHepatitis B & C, HIVMonitor for diabetes,hypertensionHepatitis B & C, HIVHepatitis B & C, HIVHepatitis B & C, HIVHepatitis B & C, HIVScreeningFBC, U Es, LFTsFBC, U Es, LFTsFBC, U Es, LFTsFBC, U Es, LFTsFBC, U Es, LFTsFBC, U Es, LFTsFBC, U Es, LFTsFBC, U Es, LFTsMonitoringC h ap t e r 4 : P so r iat ic a r t h r i t isTable 4.1. Pharmacological management of psoriatic arthritis as per NICE guidelines(rows with light background show drugs used 1st line; those with darker backgroundare biologic agents used as 2nd-line therapies)821/19/2021 5:30:57 PM
200mg every 2 weeks or400mg every 4 weeks50mg monthlyCertolizumabGolimumabRheumatology A CBA to Management.indb 83150mg monthly45mg every 12 weeks, or90mg every 12 weeks inthose 100kg requiringhigher dose80mg 4-weekly5mg twice nsider 100mgmonthly in those 100kgif inadequate responseat 50mg50mg SC weekly or25mg twice weeklyEtanercept (Enbrel,Benepali biosimilar)JAK inhibitorHumanisedmonoclonal antibodyto IL-17AMonoclonal antibodytargeting IL-12 andIL-23Humanisedmonoclonal antibodyto IL-17AHumanised anti-TNFmonoclonal antibodyPegylated TNFantibodyTNF fusion proteinNICE TA5432nd lineNICE TA5372nd lineNICE TA3402nd lineNICE TA4452nd lineNICE TA2202nd lineNICE TA4452nd lineNICE TA1992nd lineHepatitis B & C, HIV, TBHepatitis B & C, HIV, TBHepatitis B & C, HIV, TBHepatitis B & C, HIV, TBHepatitis B & C, HIV, TBHepatitis B & C, HIV, TBHepatitis B & C, HIV, TBMonitor forherpes zosterLipidsFBC, U Es, LFTsFBC, U Es, LFTsFBC, U Es, LFTsFBC, U Es, LFTsFBC, U Es, LFTsFBC, U Es, LFTsFBC, U Es, LFTs4 . 4 : M ana g e m e n t831/19/2021 5:30:57 PM
C h ap t e r 4 : P so r iat ic a r t h r i t isIn the initial stages, NSAIDs can be used to treat joint stiffness,swelling and pain. For flare-ups, or the injection of one joint (e.g. theknee), which may have flared, corticosteroids can be used. A typicaloral dose for a flare may be 20–40mg daily on a reducing dose.For intramuscular injections, typical doses range from 80–120mg.For intra-articular injections, doses range from 40–80mg ofDepo-Medrone or triamcinolone.Disease-modifying antirheumatic drugsIn order to prevent long-term damage to the joints and to controlskin involvement, DMARD therapies have been used, backed up byclinical trials.Oral synthetic DMARDs are considered to be the first-line agentsfor control of PsA and often also have a beneficial effect on thejoints. They include methotrexate, sulfasalazine and apremilast.In patients where oral synthetic DMARDs have been ineffectivein providing optimal disease control, biologic agents have beenlicensed and approved by NICE and are used. These includeadalimumab, certolizumab, etanercept, golimumab, infliximab,secukinumab, ustekinumab, ixekizumab and tofacitinib.4.5CasesThe following cases are based on real patients and are presented tohelp you consider how you would manage the scenarios.84Rheumatology A CBA to Management.indb 841/19/2021 5:30:57 PM
4 . 5 : C as e sCase history 4.1A 25-year-old man presented with a swollen knee. He developed the swellingwithout any trauma or injury. He developed psoriasis in his late teens but wasotherwise well. He was referred urgently to the rheumatologist. On examination, hehad a large joint effusion in his right knee. The rheumatologist aspirated the kneeto obtain 15ml of straw-coloured fluid. The fluid was sent for microscopy, cultureand sensitivity. The aspirate returned no growth or crystals. There was a mixedpopulation of white cells with neutrophils and macrophages seen.Further blood tests showed a negative ANA, rheumatoid factor and anti-CCPantibodies. His CRP was increased at 22ng/ml and the ESR was 34mm/hr.What would you prescribe for his knee pain? Naproxen 500mg bdNaproxen 500mg bd with omeprazole 20mg dailyPrednisolone 40mg orally daily for 1 weekCodeine phosphate 30mg as requiredParacetamol 1g four times dailyAn NSAID would be indicated, with a PPI, to control the inflammation. High doseprednisolone would normally be given if more than one joint was involved. The patientcould also be offered intra-articular corticosteroid if they wished. Codeine is not helpfulfor inflammatory pain in acute psoriatic arthritis. Paracetamol is unlikely to be effective.The patient improved for a few weeks but unfortunately returned 6 weeks laterwith more pain, stiffness and swelling involving both knees, with dactylitis in histoes of both feet.What would be the next treatment option? Start prednisolone and consider starting methotrexateMethotrexate aloneFurther course of NSAIDsConsider starting biologic anti-TNF therapySwitch to another type of NSAIDThe patient has developed more extensive disease and requires control of theacute episode with corticosteroids and then longer-term DMARD medication inthe form of methotrexate, which is first line. A further course of steroids is unlikelyto control recurrent episodes and the patient is likely to require more long-termDMARD therapy. The patient requires a trial of synthetic DMARDs, such asmethotrexate, before starting biologic therapy, as directed by NICE guidelines.Switching to another DMARD is unlikely to provide optimal disease control.The patient is started on a course of oral prednisolone 20mg on a reducing doseand is also counselled for methotrexate, which he starts at 15mg weekly, and folicacid 5mg weekly. His knee swelling becomes better controlled and his dactylitisalso improves. He stays on methotrexate and remains in remission, with regularreview and blood monitoring.85Rheumatology A CBA to Management.indb 851/19/2021 5:30:57 PM
C h ap t e r 4 : P so r iat ic a r t h r i t isCase history 4.2A 45-year-old man has a long-standing history of PsA. He has had surgery,including PIP joint surgeries, but is flaring. He has previously tried multiple coursesof prednisolone for joint flares and is also on methotrexate DMARD therapy 15mgweekly. He is considered for second-line biologic therapy. At his screening visit, hereports to the nurse that he has a strong family history of multiple sclerosis (MS).What agents can he be considered for, to control his psoriatic arthritis? inibThe patient would be considered high risk for developing multiple sclerosis fromTNF inhibitor therapy, which is a known risk factor for MS. Therefore, he shouldbe counselled and considered for alternative biologic therapies to anti-TNFtreatments, which include the IL-12/23 inhibitors such as ustekinumab, the IL-17Ainhibitors such as secukinumab, ixekinumab and the JAK inhibitor tofacitinib.A decision is often made together with the patient, based on providing informationabout benefits and potential side-effects, ease of use (e.g. oral versus injection)and patient preference. For example, a patient who prefers oral therapy may bebetter suited to tofacitinib rather than injection therapies such as ustekinumab,secukinumab or ixekinumab. Due to the variety of treatments available, if a patientdoes not achieve an improvement after 12 weeks of one agent, they can then beconsidered for an alternative second-line therapy.86Rheumatology A CBA to Management.indb 861/19/2021 5:30:57 PM
4 . 6 : R e f e r e nc e s4.6ReferencesGossec, L., Smolen, J.S., Ramiro, S. et al. (2016) European League AgainstRheumatism (EULAR) recommendations for the management of psoriatic arthritiswith pharmacological therap
To aid understanding, the book: features real case histories to illustrate the range of clinical presentations and how these can be managed covers all common rheumatic disorders, from rheumatoid arthritis through crystal arthropathies to fibromyalgia and chronic pain conditions includes a dedi