Transcription
ObjectivesEmotional Intelligence (EQ)& Medical EducationHow Does EQ fit into the Paradigm of theCompetencies?Bryan L. Martin, D.O., FACP, FAAAAI, FACAAIProfessor of Clinical Medicine and PediatricsProgram Director, Allergy Immunology FellowshipThe Ohio State University Define and Describe Emotional Intelligence. Apply the EQ concepts of self awareness andsocial awareness which drive our actions andinfluence the physician-patient relationship toenhance communication.communication Apply the EQ concepts of self management andrelationship management to the competenciesof communication, systems based practice,patient care and professionalism.Daniel GolemanWhat is EQ?But, What IS EQ? One of the hottest buzzwords in corporateAmerica A fuzzy notion that continues to be defined Since the 1930’s those who studied intelligencerealized that there were nonnon-intellectiveintellective abilitiesthat helped predict success. The term “Emotional Intelligence” was coined in1990 Salovey and Mayer Daniel Goleman based his 1995 book,Emotional Intelligence, on this work. One attempt toward a definition wasmade by Salovey and Mayer (1990) whodefined EI as “the ability to monitor one'sown and othersothers' feelings and emotions, todiscriminate among them and to use thisinformation to guide one's thinking andactions.” [10]1
EQ Success? “the fundamentals of EI – self awareness,self management, social awareness, andthe ability to manage relationships –translate into on-the-jobon the job success.”success. Daniel Goleman, Emotional Intelligence—Why ItCan Matter More Than IQ, pg xv.This is not new!Tao Te Ching (China 6th Century B.C.) 知人者智, 自知者明。 勝人者有力, 自勝者強。 Knowing others isintelligence, Knowing yourself istrue wisdom. Mastering others isstrength Mastering yourself istrue powerEQ new words for old wisdom?Tao Te ChingEmotional Intelligence Knowing others isintelligence, Knowing yourself is truewisdom. Mastering others isstrength Mastering yourself is truepower Social Awareness Self Awareness Social (relationship)management Self managementLao TzuFour Keys to EQ Self AwarenessSocial AwarenessSelf ManagementSSocial((relationship)) managementSelf Awareness Emotional Self-awareness– Ability to understand your emotion– Recognize impact of emotions on performance Accurate self-assessmentself assessment– Know limitations and strengths– Exhibit sense of humor about themselves– Welcome constructive criticism and feedback Self Confidence– Strong and positive sense of self worth2
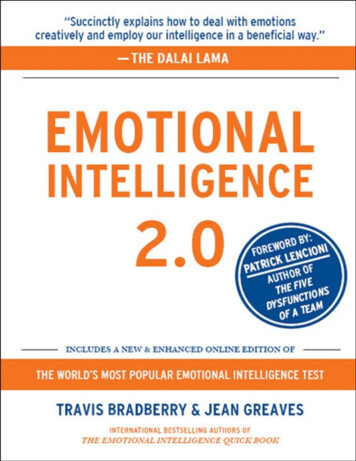
Social Awareness EmpathySelf-Management Self Control– Attuned to emotional signals– Understand other’s perspective Organizational awareness– Manage and channel impulses; stays calm Transparency– Openness to others: admit mistakes or faults Adaptabilitypy– Understand political forces, guiding valuesand unspoken rules of an organization Service Orientation– Juggle multiple demands without losing focus or energy Achievement– Drive to meet an internal standard of excellence– Foster a climate of service.– Monitor customer or client satisfaction– are available. Initiative– Seize opportunities – or create them– rather than wait Optimism– See glass half full; expect best in others.Social ManagementREGULATIONRECOGNITION InfluenceInspireDevelope OthersCommunicationChange CatalystConflict ManagementBuild BondsTeamwork and CollaborationSELFSOCIALSelf AwarenessSocial AwarenessEmotional Self AwarenessAccurate Self AssessmentSelf ConfidenceSelf ManagementSelf veOptimismEmpathyOrganizational AwarenessService OrientationRelationship ManagementInfluenceVisionary LeadershipDeveloping OthersCommunicationChange CatalystConflict ManagementBuilding BondsTeamwork and CollaborationTeaching Emotional Intelligence and Skills3
EQ can be learned “While our emotional intelligencedetermines our potential for learning thefundamentals our emotionalcompetence show how much of thatpotential we have mastered . “An underlying EI ability is necessary,though not sufficient, to manifest a givencompetency or job skill.” Goleman, EQ pg xv-xviLevels of Awareness1.2.3.4.Unconscious incompetence: ignoranceConscious incompetence: acceptanceConscious competence: skillsUnconscious competence: habitEQ and the Competencies How does EQ fit into the paradigm of thecompetencies Paradigm: The subway Paradigmg of the competenciespbringsg EQinto the formal curriculum for medicaleducation.– Old paradigm: we teach them the hardscience of medicine– New paradigm: we teach them how to becompassionate physiciansEQ meets Medical EducationCompetencies Patient Care Medical Knowledge Practice-based Learningand Improvement Interpersonal andCommunication Skills Professionalism Systems-Based Practice EQ FundamentalsSelf AwarenessSocial AwarenessSelf ManagementR l tiRelationshiphiManagement4
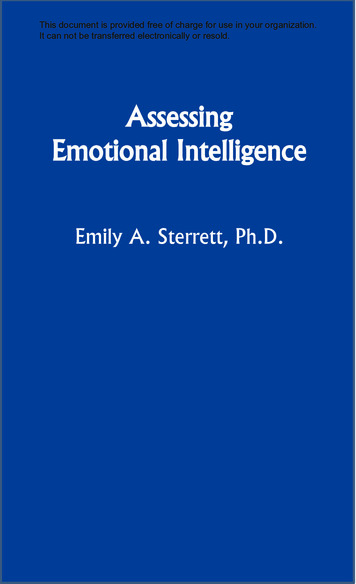
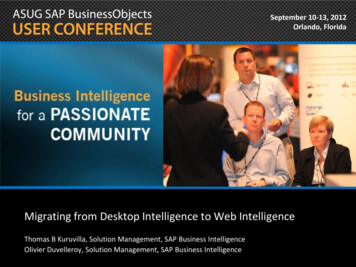
Slide courtesy of Dr. Thomas Nasca, CEO of ACGMELevel of Skills: Dreyfus modelLevel of AwarenessDreyfus LevelUnconscious incompetenceNoviceConscious incompetenceAdvanced BeginnerConscious competenceCompetentProficientExpertUnconscious competenceMasterImpact of the levels of awareness When the student is ready, the teacherappears Unconscious incompetence is a state ofinnocent ignorance: “II dondon’tt know that Idon’t know.” When asked why s/he misbehaved, achild will often answer: “I don’t know.”– This may be a true statement5
Implications of theLevels of Awareness1. Unconscious incompetence: ignorance Teach EQ basics and provide a frame forlater skills2. Conscious incompetence: acceptance Teach basic EQ skills related to thecompetencies3. Conscious competence: skills Interpersonal andCommunication Skills Residents must be able to demonstrateinterpersonal and communication skills thatresult in effective information exchange andteaming with patients, their patients families,professional associatesand p– Communicating with patients and families– Communicating with team members– Scholarly CommunicationProvide monitored experiences -- use skills4. Unconscious competence: habit Life Long learningInterpersonal andCommunication Skills Some resident physicians have significantdifficulty accurately assessing how wellthey communicate with patients Physician trainees rarely get feedbackregarding interpersonal skills. Standardized patients and facultyobservers may provide insight.Patient Care Residents must be able to provide patient carethat is compassionate, appropriate, andeffective for the treatment of health problemsand the promotion of health.– Gathering information Building relationships with patients and families– Synthesis– Partnering with patients/families Gaining trustAssessing physician’s interpersonal skills: Do patients andphysicians see eye to eye?, Am J Phys Med Rehab, 2002,Dec;81 (12)Practice-based Learning andImprovement Residents must be able to investigate andevaluate their patient care practices, appraiseand assimilate scientific evidence, and improvetheir patient care practices.––––Life-longLifelong learningEvidence based medicineQuality improvementTeaching skillsProfessionalism Residents must demonstrate professionalism,as manifested through a commitment tocarrying out professional responsibilities,adherence to ethical principles, and sensitivityt a diversetodipatientti t populationl ti– Professional behavior– Ethical principles– Cultural competence6
We Already Have TOO Much toTeach!Systems-Based Practice Residents must demonstrate an awareness ofand responsiveness to the larger context andsystem of health care and the ability toeffectively call on system resources to providephealth careoptimal––––Health care delivery systemCost effective practicePatient safety and advocacySystems causes of error Do we really have to thinkabout this touchy-feelymumbo jumbo?– Let alone Teach itit What does this have to dowith our REAL jobs – to teachmedicine (MedicalKnowledge)?AMA News: August, 2008Inappropriate Behaviorsper the Joint CommissionAMA News: Dec 1, 2008 Often manifested by Health CareProviders in Positions of PowerPhysical ThreatsVerbal OutburstsRefusing to perform assigned tasksUncooperative attitudes– Reluctance to answer questions, returncalls– Condescending language– Impatience7
Joint Commission“Culture of Safety” “Overt and passive behaviors undermineteam effectiveness and can compromisethe safety of patients.”– Patient care,, Practice-based Learningg andImprovement, Systems-Based Practice “All intimidating and disruptive behaviorsare unprofessional and should not betolerated.”Unconscious incompetence Rather than be angry or dismissive ofanother’s inability to explain theirbehavior:– Supply vocabulary for understanding anddiscussion– Model appropriate behavior– Provide practice scenarios– Professionalism, Interpersonal and CommunicationSkillsConscious Incompetence What does this have to do with me? What does the touchy feely stuff have todo with real life medical decisions? I have more important things to deal withthan this stuff! OK, I understand the concepts; but howcan I use them in my day to day life?– The student is ready! Is the Teacher?Conscious Competence This occurs when we get “buy in.” At this point:– Terms are understood– People are ready to use their skills in dailyinteractions It still requires conscious effort to useskills and may sometimes feel unnatural– Encouragement– ModelingUnconscious competence At this point the skills have become habit. There is no longer conscious thoughtregarding actions, but EQ skills havebecome unconsciousunconscious. The trick is: How do we get to this point?–?8
Men and women are notprisoners of fate, but onlyprisoners of their own minds.- Franklin D. RooseveltRemember the 4 “S’s”Self AwarenessSocial AwarenessSelf ManagementSSocial((Relationship)) ManagementTeaching moments Previous personal experience Scenarios– Verbal– Photographic– Video/movie– Standardized Patient– Observation with patients and with staffReflections Residents must be aware not only of theireffect on others, but of their internalmessaging.– Portfolios– Case Presentations In case presentation of a newly diagnosedcancer, part of the discussion can focus on howto inform the patient and family.9
For More Information www.eiconsortium.orgPrimary ReferencesQuestions? Goleman, Daniel. Emotional Intelligence: Why itcan Matter More than IQ. NY, NY, Bantam,1995. Goleman, Daniel, Richard Boyatzis and AnnieMcKee Primal Leadership: Learning to LeadMcKee.with Emotional Intelligence. Boston, MA,Harvard Business School Press, 2002. Goleman, Daniel. Social Intelligence: BeyondIQ, Beyond Emotional Intelligence. NY, NY,Bantam Dell, 2006.References Millis, SR et al, Assessing physicians’ interpersonal skills: dopatients and physicians see eye-to-eye?, Am J Phys Med Rehab,2002 Dec,81(12):946-51. Van Zanten, M et al, Using Standardized Patients to Assess theInterpersonal Skills of Physicians: Six years’ Experience With ahigh Statkes Certification Examination, Health Communication,( ) 195-205.2007 Oct,, 22 (3): Lee, Fred. If Disney Ran Your Hospital: 9½ Things You Would DoDifferently. Second River healthcare Press, Bozeman, MT, 2004. Gladwell, Malcolm. Blink: The Power of Thinking withoutThinking. NY, NY, Little Brown and Company, 2005.10
Emotional Intelligence (EQ) & Medical Education How Does EQ fit into the Paradigm of the Competencies? Bryan L. Martin, D.O., FACP, FAAAAI, FACAAI Professor of Clinical Medicine and Pediatrics Program Director, Allergy Immunology Fellowship The Ohio State University