Transcription
Chicago Senior SmilesThe Retirement Research FoundationChicago Community Oral Health ForumHeartland Health Outreach8/15/2011
ContentsAcknowledgements . 3Introduction . 3Chicago Senior Smiles . 6Methodology . 6Sites Demographics . 14The Englewood Community . 15Rogers Park Community . 16Humboldt Park Community . 16Results . 16Access and Utilization of Dental Care . 17Self-Reported Oral Health Status. 18Oral Health Prevention . 18In Mouth Screening. 19Discussion . 20Recommendations . 22Financial Report . 24Appendix . 25Screening Form . 25Senior Site Information . 26Data Table: Chicago Senior Smiles Basic Screening Survey, 2011 . 292
ACKNOWLEDGEMENTSThe Chicago Community Oral Health Forum would like to thank the RetirementResearch Foundation for their support of the Chicago Senior Smiles Project, the OthoS. A. Sprague Memorial Institute for their ongoing operational support, the UIC Collegeof Dentistry, and Heartland Health Outreach for housing this important oral public healtheffort.INTRODUCTIONDuring the past several decades, the percentage of older adults retaining theirnatural teeth has steadily increased resulting in improved oral function and quality oflife. Mainly as a result of fluoridated water and advances in dental treatmenttechniques, the average number of teeth in people 65 and older has increased to 19.With longer life expectancy and tooth retention, older adults remain at risk for dentalcaries (cavities) and periodontal (gum) disease that often leads not only to tooth loss butexacerbation of many systemic chronic diseases. Cultural practices, lack of financesand lack of priority to maintain natural teeth contribute to choosing tooth removal overtooth saving procedures. Having missing teeth, oral pain from untreated dental diseaseand wearing ill-fitting dentures can also affect proper nutrient intake needed to supportoptimal systemic health. People with poor masticatory function modify their diets,avoiding fresh fruits and vegetables in favor of soft, easily chewed foods that aretypically high in simple carbohydrates and low in proteins.Many medications taken by the elderly also affect their oral health. Over 400commonly used prescription and over-the-counter drugs cause xerostomia (dry mouth)3
and increase the risk for oral disease. Additionally, impaired mobility and disabilitiesexperienced by many older adults may make brushing and flossing difficult orimpossible. In vulnerable populations such easily preventable and treatable oral healthproblems can spiral out of control.Oral and pharyngeal cancers, that primarily affect adults over age 55 years resultin significant morbidity, disfigurement and substantial health care cost.Oral andpharyngeal cancers occur more frequently than leukemia, Hodgkin’s disease, andcancers of the brain, cervix, ovary, liver, pancreas, bone, thyroid gland, testes, andstomach combined. Unfortunately, diagnosis for oral and pharyngeal cancer is mostoften made in late stages and the over-all five-year survival rate for these cancers isonly 53 percent.Chicago seniors face many barriers to obtaining needed oral healthcare includinglimited motor functions, use of mobility aides, lack of transportation, limited affordableaccess points in their community and the general cost of care. Older adults lose theirdental insurance when they retire and many live on fixed income necessitating out-ofpocket payment for oral healthcare. Most seniors are covered by Medicare, but it onlycovers an extremely limited dental services related to treatment of specific medicalconditions.Medicaid dental coverage for adults in Illinois is limited to restorative,dentures and emergency care or pain relief and many independently living seniors donot qualify for the Medicaid program.To help adults maintain healthy teeth for life, community-based strategies shouldfocus on preventing and reducing oral disease and promoting oral health as an integralpart of overall health.Community-based strategies should: increase public and4
professional awareness of good oral health through the lifecycle as well as decreasingrisk factors and promoting healthy behaviors; expand partnerships to organizationsfocused on aging issues; monitor oral health status of older adults; ensure access toclinical services; and involve all health professionals in improving the oral health statusof the aging population.Existing key data on oral health among Illinois’ elderly populationOver 15 percent (1.9 million) of the population (12.8 million) are 60 years of ageand older (U.S. 2000 census).Nineteen percent of adults 65 years old and older no longer have any naturalteeth and 30 percent of those who still have some teeth, have lost 6 or more.(IDPH, BRFSS 2006)Only 29 percent of adults 65 years of age and older report having dentalinsurance coverage. (IDPH, BRFSS 2003)The five-year oral and pharyngeal cancer incidence rate in Illinois is 16.1 amongmales (per 100,000 males) and 6.1 among females (per 100,000 females).(Illinois Cancer Registry 1995-2000)Only 36 percent of the oral and pharyngeal cancers are diagnosed in the earlystages. (Illinois Cancer Registry 1995-2000)The Senior Smiles (Basic Screening Survey or BSS) is oral health surveillanceand health promotion/disease prevention project, data are collected through voluntaryoral health screening for seniors 60 years old and older. Studies such as the ChicagoBSS reported here are vital to discern emerging trends in disease status, treatmentneeds of a populations and health and disparities research. They add to the compilation5
of data, are used to move services and research forward, are crucial in identifying goalsthat close health disparity gaps.Chicago Senior SmilesThe Chicago Senior Smiles project goal was to conduct an oral healthsurveillance and health promotion/disease prevention project at selected Chicago sitesserving elders for the purpose of:identifying unmet oral health needsestablishing oral health promotion/disease prevention prioritiesdeveloping recommendations to address unmet needs based on nterdisciplinarypartnershipsdesignedtoimprove oral health outcomes and reduce oral disease disparities amongtargeted vulnerable eldersThe project will expand oral health surveillance of Chicago elders receivingservices at community-based sites and determine future programmatic directions. TheChicago Senior Smiles will help to increase community support, to inform policydecisions and to implement oral health promotion/disease prevention interventions thatmeet the unique needs of older adults.METHODOLOGYUpon knowledge of funding for the project, a workgroup was formed whichconsisted of CCOHF staff and other consulting patients. The members of the seniorworkgroup are as follows:6
Kimberly Bartolomucci, CoordinatorAnne Clancy, RDH, MBA (Provider)Mona Van Kanegan, DDS, MS (Provider)Sangeeta Wadhawan, BDS, MPH (Epidemiologist)Alejandra Valencia, DDS, MS, MPH (Researcher, fluent in Spanish)Julie Janssen, RDH, MA (Acting Dental Director, Illinois Department of PublicHealth, Oral Health Division; coordination with state IDPH data collectionefforts).The above group met in person and/or through monthly (and more frequently inplanning phase and during active data collection) conference calls to update onprogress and coordination of the project. Once the statewide data is available, we willreconvene with expanded statewide group to compare data, compile the results anddevelop local and statewide strategies to address the issues identified through datacollection.The Chicago Community Oral Health Forum identified three neighborhoods topilot their research: Englewood, Humboldt Park, and Rogers Park. Within the threeneighborhoods, thirty-three sites serving Senior Citizens were randomly chosen andasked to voluntarily participate in our screening and education project. Oral healthsurvey, in mouth screening and education program was conducted at selected sitesincluding independent senior living, assisted living, and institutionalized elders inspecific targeted communities of Chicago.7
Heartland Alliance Research Review Committee approval was obtained prior toscheduling screenings of the seniors. The Illinois Department of Public Health’s Smilesover Time screening forms (see Appendix) were utilized so that the collected Chicagodata can compared with statewide data. Screeners and interviewers were trained andcalibrated before the initiation of data collection. Light and disposable mirrors were usedfor the “in mouth” screening. Data was entered into SPSS database for analysis.Detailed Activities of the Chicago Senior Smiles1. Establish an administrative structure to support and guide the project.a. The Chicago Community Oral Health Forum (CCOHF) contracted an oralhealth epidemiologist through the Illinois Oral Health Coalition, IFLOSSupon learning of award funding.b. Within the first three months, a workgroup was established to identify sitesfor senior screenings, identify key stakeholders and begin stages ofInstitutional Research Review Board (IRB) Approval for research. Sincemuch of the work CCOHF is done in partnership with the University ofIllinois at Chicago College of Dentistry, an initial IRB application wassubmitted to UIC. However, since CCOHF is a program of HeartlandHealth Outreach, not UIC, the IRB declined to approve our research. TheResearch Review protocol was then submitted to Heartland Alliance’sResearch Review Committee (RRC).The research approval processdelayed our project by nearly eight months. We began data collectionimmediately upon RRC approval was. This process took much longer that8
anticipated and we experienced loss of interest in some of our partnersites because of delayed start. Consent to participate was received from10 sites, and screening of 125 older adults occurred between April andJuly 2011.c. During the time RRC was reviewing our application, the epidemiologistcompiled a listing of senior housing sites in our three target communities,and initiated work with the City of Chicago Department of Aging. Weaimed to obtain their full collaboration as many Chicago area seniors useCity of Chicago resources and congregate at Cit of Chicago sites. Thedevelopment of the collaboration with the Department on Aging was verychallenging and resulted in the project proceeding without theircollaborative efforts.d. For the Senior Smiles project, we used the existing Illinois Department ofPublic Health’s screening tool for seniors so that Chicago data can becompared with statewide data.Our research associate and projectcoordinator locally managed the collected data and used the SPSSsoftware for analysis.2. Identify community-based sites serving older adults ( 60 years old) to participatein the oral health survey project and health promotion/disease preventionintervention.a. Attached in the Appendix is a list of selected sites representing our threetarget neighborhoods, their site name, address, number of residents andtheir participation status.Each site director was sent an informational9
packet, called a minimum of two times, and visited at least once by ourproject coordinator. We had a very difficult time with some sites allowingus to come in, even with explanation, offers of give-a-ways, andeducational programs.b. Each site that agreed to host our screenings was given flyers and sign-upsheets. Even though the events were promoted, participation by seniorsvaried greatly and was challenging.3. Administer oral health survey to identify unmet needs and design appropriateinterventions for targeted elders.a. By the conclusion of our data collection window, CCOHF staff and trainedvolunteers were able to conduct 125 surveys at selected sites utilizing theapproved survey instrument in one-on-one/face-to-face interview fashion.Our licensed provider staff were able to perform the in mouth screeningand provide individualized prevention education to seniors. Additionally,staff was able to help navigate many seniors to obtain needed dentalservices.For example, every senior that was in need a referral (did nothave a dentist and was identified treatment needs) were given the name,phone number and address of a resource in the closest proximityavailable. CommunityHealth, a free, non-profit clinic for the uninsured wasone of the main referral sites, as well as the UIC College of Dentistry.Because our data collection was unidentified data, we do not have theability to follow-up with those screened to ensure they received care.10
b. Approximately 25 non-English speaking individuals were surveyed,screened and educated in their primary language, Spanish.Most ofthese participants resided Humboldt Park community.4. Conduct data analysis and prepare report for wide distribution to Chicagostakeholders.a. Survey results, analyzed data, and written report summarizing ,prioritysettings,andprevention/treatment needs/gaps is included in the body of this report.b. CCOHF will disseminate Senior Smiles data report and recommendationsto key oral health stakeholders through The Burden of Oral Disease inChicago (document pending).c. CCOHF will present this data at a scheduled Oral Health Summit (ChicagoJanuary 27, 2012).d. CCOHF staff will reconvene senior work group and staff from the IllinoisDepartment of Public Health Oral Health Division to look at local andstatewide data from this project.The charge to the group will be 1)compare data (local, state and other) compile results, and consult withexperts in elder care to understand needs and challenges;2) outlinestrategies that will be needed to address multiple challenges to optimaloral health in seniors and 3) identify easily implemented ideas withminimal resources that will yield improvements to the current system andhealth status.11
5. Implement appropriate oral health promotion/disease prevention interventions forseniors participating in program.a. Each participant screened was provided individualized oral hygieneinstruction/counseling and toothbrushes/dental floss as well as anydentifrice aide needed, on an individualized basis.b. At each participating site, we distributed linguistically/culturally rticipating sites serving seniors.information/materialstoProper brushing frequency andtechnique were re-enforced with patients, particularly with seniors thatreported or had evidence of xerostomia (dry mouth). It was not in thescope of the project to provide direct services including dental prophylaxis.c. All participants were screened for oral cancer. Seniors that reported orsuspected to be current users of tobacco products (smoked andsmokeless), were provided with information on decreasing their risk fororal cancer and dental diseases. None of the screened seniors receiveda provisional or screening diagnosis of oral or pharyngeal cancer. Fiveseniors screen were found to have other types of oral lesions and werereferred to UIC College of Dentistry for thorough evaluation and follow-upcare.In Mouth ScreeningThe following criteria were used for the in mouth screening:12
1. Oral hygiene Excellent Little or no plaque, tissue is healthy in appearance with noinflammation present Good Small amounts of plaque and slight inflammation of tissue Fair Heavy amounts of plaque with severe inflammation of the tissue,calculus is present Poor Material alba with no signs or indications that teeth are beingcleaned. Gross amounts of inflammation are present with bleeding Not applicable No teeth present2. Untreated decayUntreated decay was detected when a screener can readily observe two things –A loss of at least ½ mm of tooth structure at the enamel surface (for reference,the ball at the tip of a World Health Organization (WHO) periodontal probe is ½mm in diameter) and brown to dark-brown coloration of the walls of the lesion.3. Treatment Urgency: Code 0 No obvious Problem. (No problems observed) Code 1 Early dental care is needed. (Cavitated lesion withoutaccompanying signs or symptoms, suspicious white or red soft tissueareas)13
Code 2 Immediate dental care is needed.(Signs or symptoms thatinclude pain, infection, or swelling)Those participants with no obvious dental problems observed were givena code “0”, meaning that they should receive routine dental check-ups asrecommended.The screener may, however, override a Code “0” andassign a Code “1” if there was some reason it was felt that the participantneeds to see a dentist sooner than their next routine checkup.4. Referral Yes the screener recommends that the participant should be seen by adentist for a comprehensive dental examSITES DEMOGRAPHICSIllinois is the fifth-most populous state of the United States of America. As of2008, Illinois has an estimated population of 12.9 million. Chicago is the largest city inthe state and the third most populous city in the United States, with its 2009 estimatedpopulation of 2.8 million. As per 2008 estimates Chicago is home to 22% of the totalstate population.Chicago has a diverse population mix. One-third of the population is Hispanicand one-third is African-American. Fourteen percent of the population is 60 years ofage or over and almost one-third of the population is under 19 years of age.14
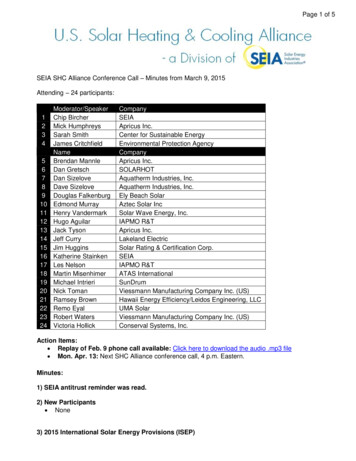
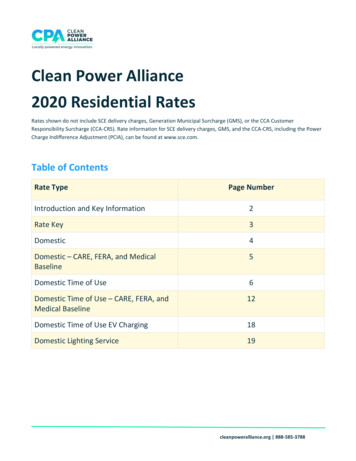
Figure 1. Chicago Community AreasRogers Park (1)Humboldt Park (23)Englewood (68)The Englewood CommunityThe city of Chicago is divided in 77 communities (see fig.1). Englewood is listedas community area “68”, a total population of 40,222 with 98% of its residents identifiedas African Americans, and 0.4% as Caucasian. Englewood has been identified as oneof the poorest areas of Chicago with 44% of
including independent senior living, assisted living, and institutionalized elders in . Heartland Alliance Research Review Committee approval was obtained prior to scheduling screenings of the seniors. The Illinois Department of Public Health’s Smiles over Time screening forms (