Transcription
Effective Case Management Models:Which Should You Use?Tuesday, April 15th, 2014Toni G. Cesta, Ph.D., RN, FAANPartner and ConsultantCase Management Concepts, LLCDallas, TexasBeverly Cunningham, MS, RNVice President ResourceManagementMedical City Dallas Hospital andPartner and ConsultantCase Management Concepts., LLCDallas, TexasThe information provided in AHC Media Webinars does not, and is not intended to constitute medical or legal advice.Opinions, references and links provided by our speakers are provided for your convenience and do not represent ourendorsement of such opinions, products or services.
FACULTYToni G. Cesta, Ph.D., RN,FAAN is Partner and HealthCare Consultant in CaseManagement Concepts, LLC, aconsulting company whichassists institutions indesigning, implementing andevaluating acute care and community case managementmodels, new documentation systems, and other strategiesfor improving care and reducing cost. The author of eightbooks, and a frequently sought after speaker, lecturer andconsultant, Dr. Cesta is considered one of the primarythought leaders in the field of case management. Dr. Cestawrites a monthly column called “Case Management Insider”in the Hospital Case Management journal in which sheshares insights and information on current issues and trendsin case management. Prior to her current work as a casemanagement consultant, Dr. Cesta was Senior VicePresident – Operational Efficiency and CapacityManagement at Lutheran Medical Center in Brooklyn, NewYork.Bev Cunningham, RN, MS is VicePresident, Resource Management atMedical City Dallas Hospital. Herareas of responsibility include CaseManagement, Health InformationManagement, Clinical DocumentationIntegrity, Patient Access and TransplantFinancial Services. Bev is a well‐knownspeaker in the Case Management field.Involved in the development of casemanagement for over twenty five years, her areas of expertiseinclude denials management, patient flow and the role of theCase Manager and Social Worker in the Case Managementprocess. She has served as a Commissioner on the Commissionfor Case Management Certification. Bev is also a partner andconsultant in Case Management Concepts, a company thatprovides support to hospitals regarding effective CaseManagement model development and evaluation. Bev'spublications include a chapter in CMSA's Core Curriculum forCase Management Certification and most recently, co‐author ofthe book, Core Skills for Hospital Case Management. She is alsoon the advisory board for Hospital Case Management.2
LEARNING OBJECTIVES1.2.3.4.Discuss the foundations of case managementpractice.Review the critical functions of an effective casemanagement department model.Explain new and revised case managementstandards, regulations, and laws put forth byCMS, TJC and the federal government.Evaluate case management protocols andpenalties.
CASE MANAGEMENT STEERINGCOMMITTEEThey can help you by being allies in thechange process!!!! AdministrationNursing/Patient Care ServicesPhysician LeadershipDirector of Case ManagementDirector of Social WorkEmergency Department LeadershipFinance LeadershipPatient FlowOthers as needed4
MODEL DESIGN Determine your case management modelReview roles and functions of other membersof the interdisciplinary care team Social Work Physicians Staff Nurses (discharge planning, etc.) Ancillary Services Interdisciplinary patient care roundsCase management clerical support5
PICKING THE MODEL THAT WILLBE RIGHT FOR YOURORGANIZATIONCOMPARISON OFTWO MODEL DESIGNS6
INTEGRATED MODELALL FUNCTIONS PERFORMED BY A SINGLECASE MANAGER. INTEGRATES PREVIOUSLYDISCONNECTED FUNCTIONS.7
DEPARTMENTAL FUNCTIONS in theINTEGRATED MODELCase Management Roles: Patient flow or coordination and facilitationof care Utilization management Discharge / Transitional planning Variance tracking Quality management8
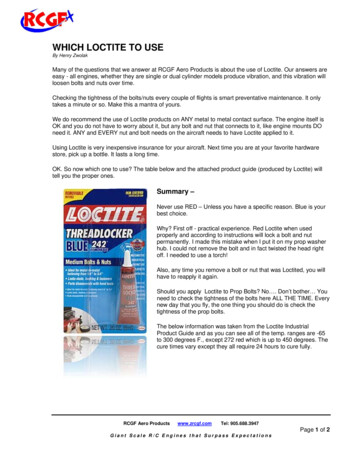
INTEGRATED MODELCASEMANAGERSOCIALWORKERCORE MEASURESCDI9
A LOOK AT THEINTEGRATED MODEL –SHARING DISCHARGE PLANNINGNURSECASEMANAGER –CLINICALDISCHARGEPLANNINGSOCIALWORKER –PSYCHOSOCIALDISCHARGEPLANNINGDISCHARGE PLANNINGSPECIALIST10
GOALS OF ACCESS POINT CASEMANAGEMENT Manage and control the types ofpatients approved for admissionProvide for alternative care whenneeded and appropriateEnsure hospital reimbursement11
ADMITTING DEPARTMENT CASEMANAGEMENT Provides gatekeeping function for: Planned admissions Urgent admissions Direct admissions Transfers12
EMERGENCY DEPT CASE MANAGERROLE FUNCTIONS:1.2.3.4.GatekeepingCoordination / facilitation of careUtilization / resource managementTransitional planning13
DETERMINING CASELOADS INTHE INTEGRATED MODEL Best practice ratio for case manager tobeds Medicine / Surgery 1:15 ICU 1:20 Maternal Child / Pediatrics 1:20 Best practice ratio for social worker 1:17 active casesToni Cesta, 200814
RATIOS Physician advisor review 10 casesper dayDocumentation improvement specialist 10 new charts per day 15 existing charts per dayToni Cesta, 200815
Collaborative Practice /Triad ModelSEPARATES THE CLINICALAND “BUSINESS”FUNCTIONS OF CASEMANAGEMENT INTOSEPARATE ROLES ANDPARTNERS ACTIVELY WITHSOCIAL WORK TO ACHIEVERESULTS16
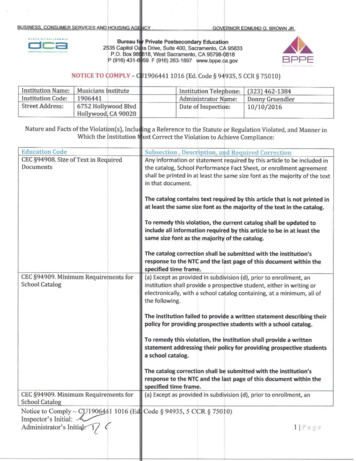
DEPARTMENTAL STRUCTURECOLLABORATIVE PRACTICE MODELCase ManagerBusinessManagerSocial Worker17
DEPARTMENTAL STRUCTURECOLLABORATIVE PRACTICE MODELCase ManagerRisk ScreeningAssessment & PlanningCoordination of CareResource UtilizationUtilization/DRGOutcome ManagementSocial WorkerManager18
DEPARTMENTAL STRUCTURECOLLABORATIVE PRACTICE MODELCase ManagerLeveraged work vs.routine tasksStewardshipClinical focusService line orientationBusinessManagerSocial Worker19
DEPARTMENTAL STRUCTURECOLLABORATIVE PRACTICE MODELBusiness ManagerMedical Necessity ScreeningAuthorization/CertificationObservation Status ComplianceClinical Documentation ImprovementDenials ManagementSocial WorkerCase Manager20
DEPARTMENTAL STRUCTURECOLLABORATIVE PRACTICE MODELBusiness Manager Primarily works the “business”side of case management Intense review of documentation Liaison between team membersand payers / regulatoryentitiesSocialWorkerCase Manager21
DEPARTMENTAL STRUCTURECOLLABORATIVE PRACTICE MODELSocial WorkerScreeningAssessment & PlanningBrief Therapeutic InterventionContinuum of Care PlanningCase ManagerSocial WorkerCrisis Intervention22
DEPARTMENTAL STRUCTURECOLLABORATIVE PRACTICE MODELSocial Worker Allows focus on core social workissues vs. routine tasks Assist with discharge planningfor select patients Clear criteria for SW referralsCase ManagerUR(substance abuse, legal, crisis,etc.)23
STAFFING RATIOS IN THECOLLABORATIVE MODEL Case manager 15 - 23Business specialist 20 - 40Social worker 1:17 (30 - 40 % of allpatients are active cases)Sue Erickson, 200824
Key Difference Between These CaseManagement ModelsINTEGRATION OF UTILIZATION MANAGEMENTINTO THE CASE MANAGER ROLE VS. SEPARATEUM / DRG SPECIALIST ROLE25
ADVANTAGES OF EACH MODELINTEGRATEDMODEL Everything underone umbrella Reducedduplication,fragmentation andredundancyCOLLABORATIVE MODEL Consolidates businessfunctions of casemanagement into onerole – builds expertise Case managers notconsumed with routinepayer functions26
ADVANTAGES OF EACH MODELINTEGRATED MODEL Data collected oncefor multiple purposes Case manager indirect communicationwith third partypayers, post-acuteproviders and vendors– they know the case!COLLABORATIVE MODEL Case managers havetike to focus on moreleveraged functions Expanded focus onclinical documentationimprovement andresource utilization27
ADVANTAGES OF EACH MODELINTEGRATEDMODEL Onestop shopping May be more costeffective may requireless staff Physician and otherstaff only have tocommunicate with oneperson on all casemanagement issuesCOLLABORATIVEMODEL Separatestwo timedependent functions Decreases competingpriorities and workerfrustration Creates holistic jobs thatoptimize skills and talents ofdifferent disciplines28
DIS-ADVANTAGES OF EACH MODELINTEGRATEDMODEL Bundleshighly timedependent functions(discharge planningand utilization review)– can be frustrating forstaff to manage If not done well canmorph into ‘task-y’model in which DP UR CMCOLLABORATIVEMODEL Requiresintensivecommunication betweentriad members (forexample: run the list) Creates someduplication such as Business manager andcase manager bothreviewing chart Assessing patient29
DIS-ADVANTAGES OF EACH MODELINTEGRATED MODEL Detail work ofutilization review mayappeal to some staffmore than otheraspects of casemanagement Will not work ifstaffing is notadequate (entireinfrastructure willcrumble)COLLABORATIVE MODEL Works best if alldisciplines report tosame administrator May be more costly andrequire more staff Will not work if staffingis not adequate30
HOW ARE THESE CASEMANAGEMENT MODELS ALIKE?THEY BUILD ON THE INTERRELATIONSHIP OF DISCIPLINES TOENHANCE CASE MANAGEMENTOUTCOMESTHEY REQUIRE STRONG SOCIAL WORKINVOLVEMENT31
HOW ARE THESE CASEMANAGEMENT MODELS ALIKE?TO BE SUCCESSFUL BOTH THESE MODELS REQUIRE: ADEQUATE STAFFINGBALANCED WORKLOAD SKILLED STAFFSTRONG LEADERSHIP32
ROLES, FUNCTIONS ANDCASELOADS ARE INTERRELATEDThe more role functions you give a hospital casemanager, the fewer patients she can handle.Obvious?Maybe .33
ADDITIONAL ROLES TO ENHANCETHE EFFICIENCY OF THEDEPARTMENT
Manages the most complex dischargeplanning issuesAllows the staff to manage more routinepatientsInterfaces with legal, guardianship,undocumented, uninsured issuesDISCHARGE PLANNINGSPECIALIST
Identifies high risk patients with frequentadmissions / readmissions / emergencydepartment visitsAssesses causes of readmissionsInterfaces with community agencies andprimary care physiciansWorks with community case manager ifavailableTRANSITIONS CASE MANAGER
Reviews records for clarity andcompleteness of documentationInterfaces with physicians, NPs and PAswhen additional documentation is neededWorks with case manager to ensure thatclinical documentation matches the levelof care orderedCan also identify missing core measuredocumentationCLINICAL DOCUMENTATIONSPECIALIST
DESIGN ELEMENTS IMPACTINGCASE LOADSModel Design Integrated vs. collaborative OtherRoles and Functions Coordination / facilitation of care Utilization and resource management Discharge and transitional planning Variance identification Quality management Clinical documentation improvement38
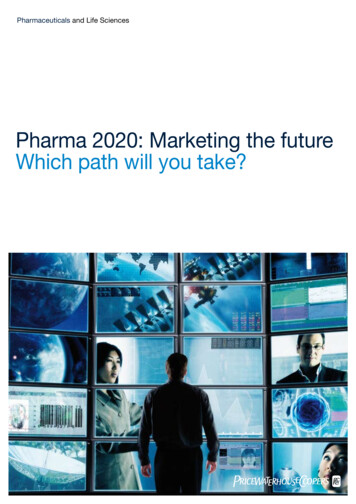
CAUTION: WORKLOAD AND CASE LOADMUST BALANCEIncreased workload Decreased caseloadWORKLOADCASELOAD39
PATIENT ASSIGNMENT MODELS UNIT-BASEDDISEASE BASEDPRODUCT LINEPHYSICIAN ALIGNEDHIGH-RISK CRITERIA PAYERCOMPLEXITYLOS/COSTCLINICALHYBRID40
PAYER MIX Check your third party payer splitMore managed care more reviewsMore Medicare more complex dischargeplanningMore Medicaid more psychosocial issues41
INTENSITY OF SERVICE What kind of services do you provide?Are you a community hospital or a tertiaryhospital?Do you transfer patients in or out?Does intensity of service effect coordinationof care and length of42
COMPLEXITY OF PATIENTS Define complexity for your patientpopulation? Medical / Surgical Psychosocial Financial43
LENGTH OF STAY This can be a double-edged swordShorter length of stay faster turnoverLonger length of stay more complexdischarge planning44
USE OF TECHNOLOGYCase management software can makeyour department more efficient byeliminating clerical type paperwork Census reports Daily assignments Retrospective data entry Faxing/XeroxingTHIS WILL FREE PROFESSIONAL STAFF UPTO SPEND MORE TIME WITH PATIENTS!45
STAFFING ANALYSIS PROCESS Start with the baseline staffing ratiosbased on your modelUse the indicators presented todetermine whether you need toincrease or decrease the baselineRemember to consider the clinicalareas you are staffing as each mayhave unique needsRevisit staffing ratios annually46
KEEP FLEXING Re-evaluateBe open to needed changes as you moveforward , nothing is in stoneBring issues back to steering committeeMake changes as neededBe flexible47
AND REMEMBER“FAILING TO PLAN IS PLANNING TO FAIL”(Fortune Cookie)48
This presentation is intended solely to provide general information anddoes not constitute legal advice. Attendance at the presentation or laterreview of these printed materials does not create an attorney‐clientrelationship with the presenter(s). You should not take any action basedupon any information in this presentation without first consulting legalcounsel familiar with your particular circumstances.
Bev and ToniTHANKS!50
Case management software can make your department more efficient by eliminating clerical type paperwork Census reports Daily assignments Retrospective data entry Faxing/Xeroxing THIS WILL FREE PROFESSIONAL STAFF UP TO SPE