Transcription
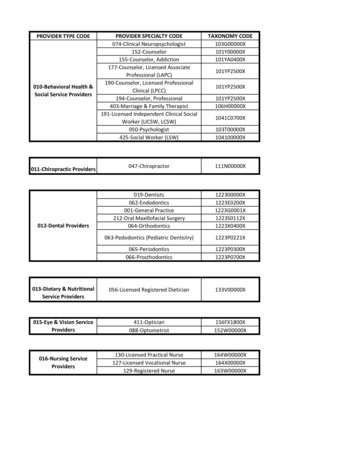
OverviewIHCP Billing Provider Application and Maintenance Formwww.indianamedicaid.comDear Prospective Provider:Thank you for your interest in the Indiana Health Coverage Programs (IHCP). This IHCP provider application iscustomized to meet the needs of groups and clinics. It is important to complete each field in the application to preventthe form from being returned for correction. Ensure that the appropriate person(s) have signed your forms.If you are currently enrolled and you need to make multiple changes to your current provider profile, this form can beused for that purpose. If you have a specific change request, refer to the provider maintenance forms. For example,use the IHCP Address Maintenance Form to change an address or the Electronic Funds Transfer (EFT) form to make achange to your direct deposit account with the IHCP.Who uses this Application?Sole practitioners and business entities that do not have rendering providers linked to their business and areone of the following provider classifications: Providers that do not have members linked to their service locations are classified as Billing Providers. Providers that are both a billing and rendering provider are classified as dual providers. The dualclassification describes providers that are enrolled both as a billing and rendering provider.Provider Types that Qualify:Provider TypeProvider TypeProvider TypeProvider Type09 Advanced Practice Nurse15 Chiropractor20 Audiologist28 Laboratory11 Mental Health Provider17 Physical Therapist21 Care Coordinator31 Physician13 Public Health Agency18 Optometrist22 Hearing Aid Dealer14 Podiatrist19 Optician27 DentistProvider Type and Specialty:Refer to the Provider Type and Specialty Matrix available on the IHCP Web site ices/pdf/TR473-IHCPProviderTypeSpecialtyMatrix.pdf todetermine the document requirements for your provider type and specialty. Based on your provider type, thematrix informs you about whether you qualify to be a billing provider. Enter your type and specialtyinformation in Fields 39-41 of Schedule A – Provider Information. Enter taxonomies in Field 42. You maysubmit as many as 15 taxonomies per National Provider Identifier (NPI). If you need more space than what isprovided in Field 42, you may attach a separate sheet listing additional taxonomies and their associated NPI.The Provider Type and Specialty Matrix lists the required documents for your type and specialty.Billing Provider’s Responsibility:Billing providers are responsible for submitting claims to the IHCP by any submission means, including paper,electronic, or the Web interChange for reimbursement.Information About the Forms:The IHCP Provider Application Packet is divided into the following sections for completion.IHCP Billing Provider Application and Maintenance Form, OverviewVersion 2.0, April 2009 Page 1 of 28 EDS Provider Enrollment UnitP.O. Box 7263Indianapolis, IN 46207-7263
Schedule A – Provider Information - This section collects information related to the prospectiveprovider including name, address information, provider type, and provider specialty. Complete all fields. National Provider Identifier (NPI) Number. With the implementation of the NPI, it isextremely important that you provide your service location ZIP 4 (all nine digits) when youcomplete forms to enroll or add a new a service location. If one of your service locationsmoves, again the new ZIP 4 code (all nine digits) is important. The Zip 4 helps the IHCP toidentify each service location you enroll.Schedule B – Organization Structure - This section collects information about the provider’s business.In addition, Providers may also indicate participation in additional programs. The following programs arelisted in Schedule B: HealthWatch is a preventative health care program offered to Medicaid-eligible members younger than21 years of age. Physicians or nurse practitioners who are enrolled as Medicaid providers are qualified toperform HealthWatch screenings. Reimbursement for HealthWatch services is higher than equivalentservices billed using standard CPT codes. HealthWatch screenings must be completed in accordance withrecommendations set forth in the HealthWatch Provider Manual Periodicity Schedule. Check the boxlabeled yes to receive the HealthWatch Provider Manual. The 590 Program is a State medical assistance program providing reimbursement for medicallynecessary covered medical services provided off site to individuals who reside in State institutions. Thefollowing provider types cannot be 590 providers: transportation, hospice, home health, DME, and longterm care facilities. There are no out-of-state 590 providers. The Medical Review Program provides determination of an applicant’s eligibility for Medicaid underthe disability category. The provider completes a medical assessment of an applicant and submits therequired forms to the Office of Family Resources. The MRT issues a favorable or unfavorable eligibilitydecision based on medical evidence that supports whether the applicant has a significant impairment.Once the documentation has been filed, the provider may submit claims to EDS for payment of certainexamination and reports. Services should not be performed unless the applicant has presented the preMedicaid eligibility form. To participate solely in the Medical Review Program, the provider should checkthe Medical Review Program ONLY. Providers that choose not to participate in the IHCP Programs andhave been requested to submit medical records, should check MRT Medical Records. Pre-Admission Screening and Resident Review (PASRR) – All Diagnostic and Evaluation Teams must Schedules C.1-C.4be contracted and approved by the Division of Disability, Rehabilitative Services (DDARS) and Bureau ofDevelopmental Disability Services (BDDS). Community Mental Health Centers must be contracted andapproved by the Division of Mental Health and Addiction (DMHA) Consent to Release Social Security Numbers. The top of Schedule C.1 contains a section thatdescribes the purpose for release of social security numbers and to whom a Social Security number may bereleased. Schedules C.1, C.2, and C.3 contain signature fields to acknowledge consent for each individualnamed in the Schedules. Disclosure of Social Security Numbers is voluntary. Refusal to provide asocial security number will result in rejection of this application.Disclosure Information - Schedule C.1. This section collects information required by federal regulationthat details information about those entities or individuals with five percent direct or indirect ownership inthe prospective provider’s business and the degree of relationship for each individual. Ownership and Control, Subcontractor Relationships - Schedule C.2. - List the Name, Title, FEIN, andBusiness Address of any person or entity that has an ownership or controlling interest in any subcontractorin which the provider entity has direct or indirect ownership of five percent or more. Managing Individuals - Schedule C.3. List all managing individuals as defined on Schedule C.3. Relationships and Background Information - Schedule C.4. Documents family relationshipsinvolved in the provider entity and provider background information. The disclosure of social securitynumbers is used only for the purpose of determining whether persons and entities named in the applicationare federally excluded parties. Refusal to provide a social security number will result in rejection of thisapplication. Profile Maintenance Signature Page. This page is completed and signed when an additional servicelocation is enrolled, or the form is used to make several changes to the billing provider’s service locationprofile. Provider Agreement – The IHCP Provider Agreement must be completed and signed. The ProviderAgreement is the first document in this packet following the IHCP Pharmacy Provider Application.IHCP Billing Provider Application and Maintenance Form, OverviewVersion 2.0, April 2009 Page 2 of 28 EDS Provider Enrollment UnitP.O. Box 7263Indianapolis, IN 46207-7263
Federal W-9 Form – The W-9 form must be completed and signed. Addenda – Additional forms are available from the IHCP Web site at www.indianamedicaid.com. The Electronic Funds Transfer Addendum is included in this packet. Submission of this form allowsproviders to obtain payment by direct deposit. Submit the Claim Certification Statement for Signature on File Addendum that is included in this packet.Processing this document allows adjudication of paper claims without a hand written signature on eachform. (Providers that submit claims on the UB form must complete the above named addendum.) Submit the Change of Ownership Addendum if you are the purchaser of an actively-enrolled provider.Additionally, a copy of the purchase or sales agreement must be included.Mailing Instructions:Please retain a copy of the completed application packet for your records. Enclose the signed ProviderAgreement and copies of all required documentation as listed on the provider application checklist, and mailthe entire packet to the following address:EDS – Provider EnrollmentP.O. Box 7263Indianapolis, IN 46207-7263Application Processing:When the Provider Enrollment Unit receives, reviews, and processes a provider application, the provider willreceive notification. If the application is incomplete or the required supporting documentation is not present,the entire application packet is returned. An instructional letter stating the reason(s) the enrollment requestwas not completed is included with the packet. If the IHCP denies the application, the provider receivesnotification explaining the denial reason. Please allow at least 30 business days for mailing and processingbefore checking the status of the submitted provider application.Refer to the IHCP Web site at www.indianamedicaid.com for additional information or contact the Provider EnrollmentHelpline at 1-877-707-5750 for assistance in completing IHCP provider application.Application Checklist:The following checklist is designed to assist providers and the IHCP in completing and verifying that information isincluded in this packet.ForProviderUse OnlyDid you remember to For IHCPUse OnlyComplete all IHCP Provider Application Schedules (A, B, and C). Complete every sectionof Schedule C.Provide all nine digits of the Service Location ZIP Code (ZIP 4)Complete and sign the IHCP Provider AgreementComplete and sign the current Federal W-9 form for tax identification purposesInclude copies of license(s), certificates, and permits for your provider specialtiesInclude a copy of your Medicare Assignment Letter, if applicable(Out-of-state billing providers must submit proof of participation in Medicare or theirState’s Medicaid Program)Complete the Change of Ownership Addendum, if applicableInclude all other elected addendaOut-of-State Billing Providers must show proof of participation in Medicare or theMedicaid Program with the state where the service location residesIHCP Billing Provider Application and Maintenance Form, OverviewVersion 2.0, April 2009 Page 3 of 28 EDS Provider Enrollment UnitP.O. Box 7263Indianapolis, IN 46207-7263
Schedule AIHCP Billing Provider Application and Maintenance Formwww.indianamedicaid.comProvider Information1. Request Type:New EnrollmentAdditional Service Location2. National Provider Identifier:3. ZIP 4: (Nine digits required)5. IHCP Provider Number and Alpha Suffix: (If currently enrolled)6. Application Completion Date:Update4. Taxonomies:7. Requested Enrollment Effective Date:8. Change of Ownership?YesNo(If Yes, complete the Change of Ownership Addendum)Billing Provider Office Location Name and AddressThe billing provider office location name and address is for the site where members obtain services and is either owned orrented by the billing provider. This location maintains supporting documentation related to the claim. The billing provider officelocation name must be the Doing Business As (DBA) name registered with the Secretary of State, except for informalassociations (Sole Proprietorship and General Partnerships). Providers, who provide services at a “place of service site,” such asa hospital or nursing facility, should enter their home/business office as their billing provider office location address and not theplace of service address. The address must be a physical location. A post office box is not a valid billing provideroffice location address.9. DBA Name:10. Indiana County:11. Telephone:12. Street Address:15. ZIP 4: (Nine digits required)13. City:14. State:16. Is claim documentation kept at this location?17. Are services provided in Indiana?YesNoYesNoLegal Name and Home Office AddressThe home office is considered to be the legal entity maintaining ownership of the above billing provider office location. The legalname must be the current name on tax, corporation, and other legal documents. The legal name and business name, aswell as the address, must match what is on the W-9.18. Legal Name:19. Street Address:20. City:21. State:22. ZIP 4: (Nine digits required)23. Telephone:IHCP Billing Provider Application and Maintenance Form, Schedule AVersion 2.0, April 200924. Tax ID Number: Page 4 of 28 EDS Provider Enrollment UnitP.O. Box 7263Indianapolis, IN 46207-7263
Mailing Name and AddressThe mailing address is the location where the IHCP sends provider bulletins, newsletters, manuals, and general correspondence.A post office box is acceptable for a mailing address.26. Telephone:25. Name:27. Street Address:28. City:30. ZIP 4: (Nine digits required)29. State:Pay To Name and AddressThe pay to address is the location where the IHCP sends checks, remittance advices, and general claims payment information. Ifthis is a billing agent’s address, please provide the name, address, and phone number of the billing agent. The name listedbelow as the Payee Name will appear as the payee on all checks. A post office box is acceptable for this address. Billing agentsmust furnish proof of authorization to be the billing agent for provider.31. Payee Name:32. Billing Agent Name:33. Telephone:34. Street Address:35. City:37. ZIP 4: (Nine digits required)36. State:Contact NameThe contact person is the person who answers questions about the information provided in this form.39. Telephone:38. Contact Name:40. Contact E-mail:41. Would you like a link to the Web interChange application sent to your E-mail address?YesNo42. Are you willing to receive IHCP bulletins and newsletters via E-mail or the Web?YesNoProvider Specialty InformationRefer to the Provider Type and Specialty Matrix on the IHCP Web site to determine the appropriate provider type, specialtycodes, and enrollment requirements for this application. Only one provider type code is permitted per application. Submit aseparate application for each additional provider type.43. Provider Type (two digit code):44. Primary Specialty (three digit code):45. Additional Specialties:46. Taxonomies (Enter a maximum of three taxonomies that apply only to this service location):CLIA CertificationDocument your Clinical Laboratory Improvement Amendment (CLIA) Certificate information in this section. CLIA numbers areassigned to one specific service location unless CMS exemption status is met.47. CLIA Number:48. Certification Type:49. Effective Date:50. Expiration Date:Note: A copy of the certificate must be attached to the application. Failure to attach a copy of the certificate willresult in no CLIA number entered on the provider profile, which could cause claim denials.IHCP Billing Provider Application and Maintenance Form, Schedule AVersion 2.0, April 2009 Page 5 of 28 EDS Provider Enrollment UnitP.O. Box 7263Indianapolis, IN 46207-7263
Schedule BIHCP Billing Provider Application and Maintenance Formwww.indianamedicaid.comOrganizational Structure1. Provider Entity Legally Organized and Structured As (Check only one):For Profit CorporationNot For Profit CorporationPartnershipGovernment OwnedLimited Liability CompanyOther, please specify* If yes, submit a copy of the state registration papers (405 IAC 1-19.1b). If no, and yourbusiness name is different from your name, please submit a copy of the Assumed BusinessName form on file with the State.2. Registered with Secretary of State*:YesNo3. Date Business Started:4b. If answered Yes in 4a, Incorporation Date:4a. Entity Incorporated:Yes5. Chain Affiliated **YesSole Proprietorship (individual)Limited Liability Partnership (LLP)No** If yes, the information about the company or organization must be included in thedisclosure information.No6. Operated by Management Company or Leased (Whole or Part) by Another Organization*** :YesNo***If yes, the information about the companyor organization must be included in thedisclosure information.Previous IHCP Enrollment Information7a. Are you currently, or have you ever been enrolled as an IHCP provider?Yes7b. IHCP Provider Number(s):NoOther IHCP Program ParticipationProviders may elect to participate in additional programs. The application overview provides detailed information about each ofthe programs listed in this section.9a. Participate in the 590 Program:8. Participate in the HealthWatch Program:YesNoYes10a. Participate in the Medical Review Program:YesNo9b. Participate in the PASRR Program:YesNo10b. Participation:NoMRT - Copying Medical Records onlyMedicare ParticipationPlease provide the appropriate Medicare identification numbers.Out-of-state providers must submit proof of participation in Medicare and their state’s Medicaid program. See the Type andSpecialty Matrix for specific document requirements.11. Medicare Number:12. Issuing State:13. Durable Medical Equipment, Prosthetics, Orthotics, and Supplies (DMEPOS) Number:14. Address for Location Where the Medicare Number is Assigned:Notes: A copy of the Medicare number assignment letter (or a Medicare Remittance Notice with correct Medicarenumber) is recommended to ensure accuracy of Medicare number assignment.Patient Population Information15. Percentage of your patient population with the following payment sources:15a. Medicaid:15b. Self-Pay:15c. Medicare:15d. TPL:(The percentages for 15a, b, c, and d should total 100%.)IHCP Billing Provider Application and Maintenance Form, Schedule BVersion 2.0, April 2009 Page 6 of 28 EDS Provider Enrollment UnitP.O. Box 7263Indianapolis, IN 46207-7263
Schedule CIHCP Billing Provider Application and Maintenance Formwww.indianamedicaid.comC.1 – Disclosure Information – Ownership and Control, Provider EntityInstructions: Please complete all four sections of Schedule C – Ownership and Control, Provider Entity; Ownershipand Control, Subcontractor Relationships; Managing Individuals; and Relationships and Background Information.Disclosure of Social Security Numbers: Disclosure of social security numbers is used for the purpose of determiningwhether persons and entities named in an application are federally excluded parties and to verify licensure. The IHCP ProviderApplication and Profile Maintenance Form's C Schedules are used to collect information required by State and federalregulations. The regulations detail information about those entities or individuals with five percent direct or indirect ownership inthe prospective provider’s business and the degree of relationship for each individual. Disclosure of Social Security Numbers isvoluntary. Refusal to provide a social security number will result in rejection of this application.*Consent To Release Social Security Numbers: All persons whose names are written in boxes marked 1a ofSchedules C1, C2, and C3 are asked to place their signature in box 1b. A signature in box 1b shall indicate that the signatoryagrees to the following statement regarding the disclosure of his or her social security number:My signature in box 1b in Schedule C1, C2, or C3 indicates that I give my express consent to the Office of MedicaidP
If the IHCP denies the application, the provider receives notification explaining the denial reason. Please allow at least 30 business days for mailing and processing before checking the status of the submitted provider application. Refer to the IHCP Web site at www.indianamedicaid.com for additional information or contact the Provider EnrollmentFile Size: 1MB