Transcription
Accolade IIFemoral Hip Stem Design rationale
Accolade II femoral hip stem Design rationaleDesigned to fit more patients,designed to fit your approach.2
Accolade II femoral hip stem Design rationaleAddressing modern demandswith novel technology.The global THA population is evolving to includea younger1, more active2, and more demanding3patient. Many femoral stem designs on the markettoday predate the emergence of this novel demand.Subsequently, an opportunity to enhance theconventional femoral stem design exists.Conventional tapered wedge femoral stems haveachieved popularity due to their simplicity andexcellent clinical results4,5. Despite these results,literature indicates that there are still unmetclinical needs6,7,8. Incidence of subsidence6, distalonly implant engagement7, and peri-prostheticfracture8 suggest a clinical need for an improvedimplant fit for this novel patient population.Stryker, along with key industry leaders, embarkedto develop a novel femoral stem. This designwould build from the sound principles of taperedwedge philosophy to meet the unique needs ofthe current patient population. At the heart ofthis development was a unique technology calledStryker Orthopaedic Modeling and Analytics,or SOMA. As a system that enables populationbased design, SOMA has powerful functionalitywith which to design, model, and analyze novelorthopaedic devices.Stryker utilized SOMA technology to design anovel stem building upon the conventional taperedwedge femoral design, incorporating uniquefeatures to allow for an enhanced implant fit intoday’s patient population9. By establishing anincreased canal fit and fill9, Accolade II has beenshown to allow for improved stability10, decreasedintraoperative femoral fractures11, as well asexcellent survivorship and functional outcomes12,13,ultimately leading to satisfied patients13,14.3
Accolade II femoral hip stem Design rationaleSOMA technologyUtilizing the proprietary SOMA technology, Stryker was able to complete one of the largest proximalfemoral bone morphology studies ever undertaken13. An illustrated look at the process bywhich SOMA technology is employed in implant design is described below.4CT acquisitionSegmentationAnalysisThe SOMA database continues toaquire new CT scans, and currentlycontains over 16,500 bones14Once acquired, all bones aresegmented into inner andouter corticesUsing SOMA tools, bonemorphology can be studied in ahighly accurate and reproduciblemanner.Design inputValidationThe results of these studies, such as thepopulation Canal Flare Index, can beutilized in implant designThe resulting implant design canthen be validated using SOMA fittingtools.
Accolade II femoral hip stem Design rationaleThree key SOMA-designed featuresBone morphology data allowed Stryker an unprecedented look at femoral anatomy, andassisted in the design of a novel femoral stem. The SOMA input* was instrumental in theestablishment of three key design features of Accolade II:Unique size-specific medial curvatureincreasing proximal conformity to improve primarystability14,15Enhanced proximal-distal proportions16shown to mimic canal anatomy to avoid distal onlyengagement and achieve cortical fit8,16Optimized stem lengthenables muscle-sparing approaches withoutsacrificing stability15,17*SOMA-design of Accolade II based on 556 CT scans.5
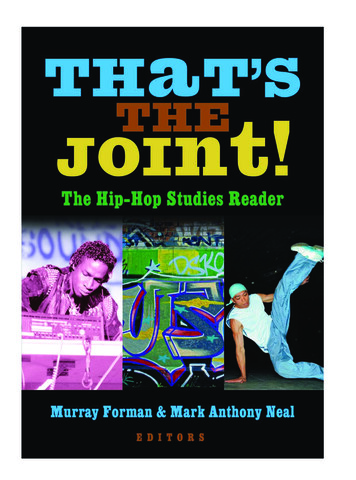
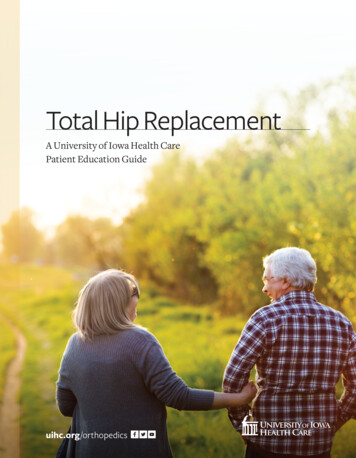
Accolade II femoral hip stem Design rationaleUnique size-specific medial curvatureInitial stability is critical to long-term implantperformance6. Early subsidence and micromotionhas been established as a strong indicator for implantfailure6. Initial stability may be increased by creatinga higher conformity between the implant and thefemoral cortices, leading to a larger areaof contact19.Analyzing the SOMA morphology study data*, it wasobserved that a constant medial curvature may notallow for a conforming canal fit throughout varyingfemoral sizes.This population-based input influenced Stryker toincorporate the market’s first size-specific medialcurvature into Accolade II. This feature was designedto enable a more conforming proximal cortical fit15,which has been shown to allow for improved implantstability19.Using femurs from the SOMA database*, fit patterns of Accolade II can be comparedto conventional tapered wedge designs. The three examples below illustrate howAccolade II achieves a more conforming canal fit throughout varying bone sizes.Small femurAccolade II6Large femurMedium femurConventionaltapered wedgeAccolade IIConventionaltapered wedgeAccolade IIConventionaltapered wedge
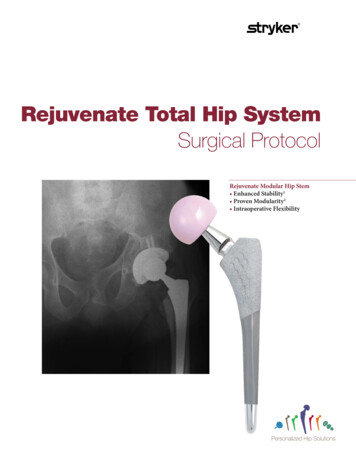
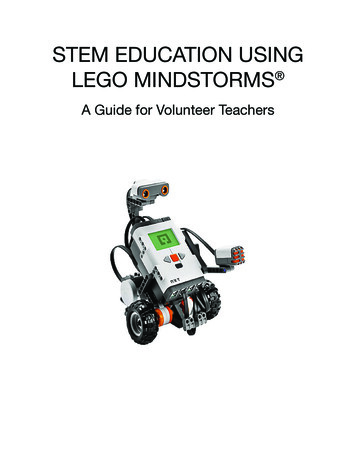
Accolade II femoral hip stem Design rationaleEnhanced proximal-distal proportionsDistal-only engaged femoral stems can experience stress shielding19and consequently may lead to elevated failure rates due to looseningand migration9. In order to better mimic the femoral anatomy andavoid distal-only engagement, a more anatomic implant growth rateis needed.Utilizing the SOMA femoral morphology study*, a moreanthropomorphic proximal-distal stem growth rate was identified.This rate led to enhanced implant proportions13, as the distalgeometry of Accolade II increases in size less than the proximalgeometry. These proportions enable Accolade II to achieve asignificantly better canal fit and fill,9 and Accolade II has shown adecreased incidence of distal-only engagement9.Comparing implant fitIn the graph above, the proximal (P) and distal (D) measurements of a population of 556 femurs were plotted (blackdots) against the corresponding stem diameters of Accolade II (gold) and a conventional tapered wedge design (grey).Accolade II achieved more fully-conforming and proximal-only fit types compared to the conventional design, whilesubsequently reducing distal-only fit by 14%.167
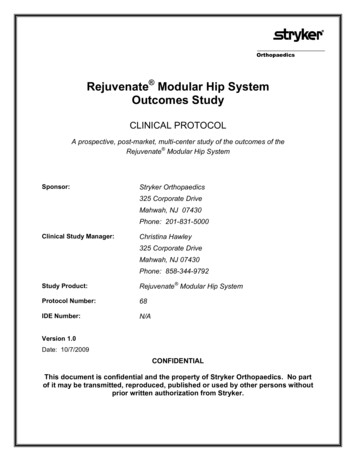
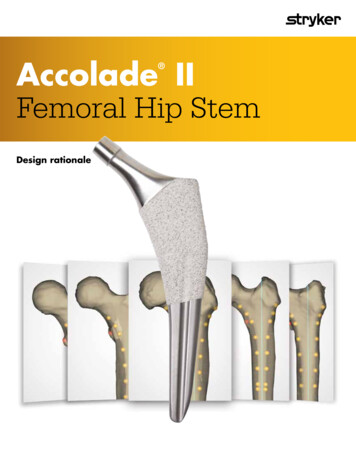
Accolade II femoral hip stem Design rationaleOptimized stem lengthPopularity of muscle-sparing approaches and bone conserving fundamentals have led to a trend inshortening of stem length20. However, there exists a complex relationship between stem length andimplant stability20. Shortening stem length without geometry optimization has been shownto increase the potential for micromotion20, which is a strong indicator for implant failure6.Accolade II utilized the SOMA database* and stability analyses to establish an optimized length foreach stem size which not only accommodates muscle-sparing approaches20, but demonstratedimproved initial stability10.“simply shortening a standard tapered wedge designmay reduce the primary stability”17Mean % of HA coated stem surfacethat experienced micromotion 50μm1750%48.6% 12%44.6% 14%40.0% 12%35%Shortened tapered wedge stemConventional tapered wedge stemAccolade II8
Accolade II femoral hip stem Design rationaleDesigned to fit your approachMuscle-sparing surgical approaches continue to gain popularity,due to the potential patient benefits of faster recovery21,22, lesspain21,22 and greater satisfaction23.Stryker’s portfolio of muscle-sparing techniques features moderninstrumentation and dynamic Medical Education programs tosupport the Direct Anterior Approach and theDirect Superior Approach.The new Direct Superior Approach was designed for surgeons whoprefer the fundamentals and familiarity of the posterior approach,but seek to provide the next evolution in muscle-sparing THAsurgical techniques for their patients.Stryker has developed a training platform to help surgeons duringthe learning curve of a new surgical approach, Stryker’s TrainingAcademy.For access to Stryker’s Training Academy, contactyour local Stryker sales representative.9
Accolade II femoral hip stem Design rationaleClinical performance“Significantly better overall canal fit”9than conventional tapered wedge designover400,000implanted worldwide24over16,500bones*survivorshipfor Accolade II pursuantto a 3.5-year mean study12in SOMA database14less than0.1mmsubsidence pursuant to2-year RSA study101099.2%5xless intraoperativefracturesobserved compared toconventional tapered wedge11
Accolade II femoral hip stem Design rationale11
Accolade II Implant catalog numbersPart 4011Neck angle132 127 References:1. National Center for Health Statistics. Health, United States, 2010: With Special Feature on Death andDying, pgs. 17 & 60.2. Kurtz S, Lau E, Ong K, Zhao K, Kelly MP, Bozic KJ. Future Young Patient Demand for Primary andRevision Joint Replacement. CORR 2009; 467:2606-2612.3. Haddad F. A Positive End to 2016. Bone Joint J. 2016;98-B:1569–70.4. Casper D, Kim G, Restrepo C, Parvizi J, Rothman R. Primary Total Hip Arthroplasty With anUncemented Femoral Component. The Journal of Arthroplasty. Vol 26, Issue 6, 2011; 838-841.5. McLaughlin JR, Lee KR. Total hip arthroplasty with an uncemented femoral component. J Bone JointSurg 2008; 90:1290.6. Paul van der Voort, Bart G Pijls, Marc J Nieuwenhuijse, Jorrit Jasper, Marta Fiocco, Josepha W MPlevier, Saskia Middeldorp, Edward R Valstar & Rob G H H Nelissen (2015) Early subsidence of shapeclosed hip arthroplasty stems is associated with late revision, Acta Orthopaedica, 86:5, 575-585, DOI:10.3109/17453674.2015.1043832.7. Cooper J, et al. Distal Fixation of Proximally Coated Tapered Stems May Predispose to a Failure ofOsteointegration. Journal of Arthroplasty. 2011. 10.1016/j.arth.2011.04.003.8. Abdel MP, et al. Epidemiology of periprosthetic fracture of the femur in 32 644 primary total hiparthroplasties. Bone Joint J 2016;98-B:461–7.9. Issa, K. et al. Radiographic Fit and Fill Analysis of a New Second-Generation Proximally CoatedCementlessStem Compared to its Predicate Design. Journal of Arthroplasty (2013). http://dx.doi.org/10.1016/j.arth.2013.04.029.10. Collopy, D. et al. A Prospective Roentgen Stereophotogrammetric Analysis (RSA) Study of the StrykerAccolade II Cementless Hipo Stem to 2 Years Post-Surgery. Abstracts from 2016 Annual AOAMeeiting–Cairns, QLD, October 9-13, 2016.11. Bono, J. et al. Total Hip Intraoperative Femur Fracture: Does a Tapered Wedge Design with a SizeSpecific Medial Curvature Reduce the Incidence of Intraoperative Femur Fracture? Presentation at47thAnnual EOA Meeting -New Orleans, LA, October 19-22, 2016.12. Pierce T. et al. Second-Generation Versus First-Generation CementlessTapered Wedge Femoral Stems.Orthopedics. 2015 38(9): 550-554.13. Kolisek, F. et al. Outcomes of Second-Generation Tapered Wedge Design. SurgTechnolInt. 2016 Apr4;XXVIII. pii: sti28/702.14. Stryker Internal presentation ‘Global Bone Morphology Study –Proximal Femur’. November 10, 2016.15. Narzikul, BS. et al. Alteration in Geometry of Femoral Stem Results in Better Fit and Fill: Comparisonof Accolade I vs. Accolade II. Presentation at 47thAnnual EOA Meeting -New Orleans, LA, October19-22, 2016.16. Wuestemann T, Bastian A, Parvizi J, Nessler J, Kolisek F. A novel tapered hip stem design optimizedfor femoral fit in a wide array of bone types. 2011 EFFORT.17. Boucher, F. et al. Preclinical Finite Element Analysis of a Novel Tapered Wedge Stem Optimized forStability at a Reduced Length. 2011 EFORT Poster Presentation.18. Lovell T, HozackW, KreuzerS, Merritt P, NoglerM, PuriL, Wuestemann T, Bastian A. Influence of StemLength on the Insertion Path in THR. 2009 ORS Poster #2040.19. Khanuja H, et al. Current Concepts Review: Cementless Femoral Fixation in Total Hip Arthroplasty. JBone Joint Surg Am. 2011;93:500-9.20. Faizan A, et al, Development and Verification of a Cementless Novel TaperedWedge Stem for Total HipArthroplasty, J Arthroplasty (2014), http://dx.doi.org/10.1016/j.arth.2014.09.023.21. Restrepo C, Parvizi J, Eslam Pour A, et al. Prospective Randomized Study of Two Surgical Approachesfor Total Hip Arthroplasty. The Journal of Arhtroplasty 2010; 25: 671-670.22. Vail T, Mariani E, Bourne M, Berger R, Meneghini M. Approaches in Primary Total Hip Arthroplasty. JBone Joint Surgery 2009; 91:10.23. M.W. Zawadsky et al./ Early Outcome Comparison Between the Direct Anterior Approach and theMini-Incision Posterior Approach for Primary Total Hip Arthroplasty: 150 Consecutive Cases, TheJournal of Arthroplasty 29 (2014) 1256-126.24. Internal Sales Data (2017).*SOMA-design of Accolade II based on 556 CT scans.325 Corporate DriveMahwah, NJ 07430t: 201.831.5000www.stryker.comA surgeon must always rely on his or her own professional clinical judgment when deciding whether to use a particular product when treating a particular patient. Stryker does notdispense medical advice and recommends that surgeons be trained in the use of any particular product before using it in surgery.The information presented is intended to demonstrate the breadth of Stryker’s product offerings. A surgeon must always refer to the package insert, product label and/or instructionsfor use before using any of Stryker’s products. Products may not be available in all markets because product availability is subject to the regulatory and/or medical practices inindividual markets. Please contact your sales representative if you have questions about the availability of any of Stryker’s products in your area. Stryker Corporation or its divisionsor other corporate affiliated entities own, use or have applied for the following trademarks or service marks: Accolade, SOMA, Stryker. All other trademarks are trademarks of theirrespective owners or holders.ACCII-PG-3 Rev-1 22894Copyright 2020 Stryker.
allow for a conforming canal fit throughout varying femoral sizes. This population-based input influenced Stryker to incorporate the market’s first size-specific medial curvature into Accolade II. This feature was designed to enable a more conforming proximal cortical fit15, which