Transcription
THE ROLE OF PARPi IN PROSTATE CANCER:EXPERTS KNOWLEDGE SHAREAUGUST 2020Dr. Neal D. Shore(Chair)Prof. Andrew J.ArmstrongProf. Emmanuel S.AntonarakisCarolina UrologicResearch CenterDuke UniversitySchool of MedicineJohns HopkinsMedicine2
FUNDINGPlease note:The views expressed within this presentation are the personal opinions of the experts. They do notnecessarily represent the views of the expert’s academic institution.AstraZeneca has provided a sponsorship grant towards this independent programme.3
EXPERTS KNOWLEDGE SHARETHE OBJECTIVE OF THIS MEETING IS TO DISCUSS THE TOPIC‘THE ROLE OF PARPi IN PROSTATE CANCER’ Your opportunity to discuss and share learnings on a challenging topic within the area ofDDR and prostate cancer A chance to hear the views of our Experts and allow them to answer the questions that areimportant to you Review and discuss Patient Case Studies, using the questions that you have sent in advanceof this eveningDDR, DNA damage response; PARPi, poly ADP ribose polymerase inhibitor(s)4
EDUCATIONAL OBJECTIVES1.Understand the MoA of PARP inhibition and its role in the treatment of prostate cancer2.Understand the prevalence of DDR mutations in prostate cancer and be able to implement thetesting strategies (specifically for somatic mutations) to predict if the prostate tumour is likelyto respond to a PARPi or other treatment3.Recognise the clinical efficacy and safety profile of PARPi for patients with prostate cancer4.Understand the place of PARP inhibition in the prostate cancer treatment pathway in the contextof other non-hormonal agents and the potential for upcoming combination therapiesMoA, mode of action5
INTRODUCTIONDr. Neal D. Shore(Chair)Carolina UrologicResearch6 Center
DISCLOSUREDr. Neal D. Shore has the following relevant financial relationships to disclose: Research/Consulting: AbbVie, Amgen, Astellas, AstraZeneca, Bayer, BMS, Clovis Oncology, Dendreon,Exact Imaging, FerGene, Ferring, Janssen, MDx Health, Merck, Myovant, Nymax, Pfizer, Sanofi, Tolmar Stock/Patents/Salary: none7
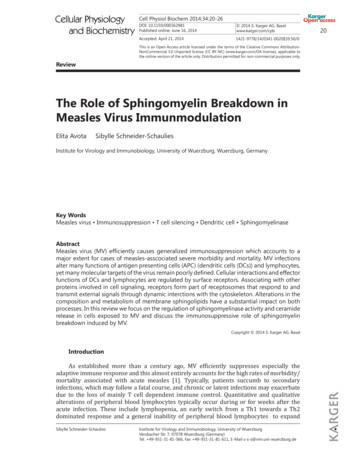
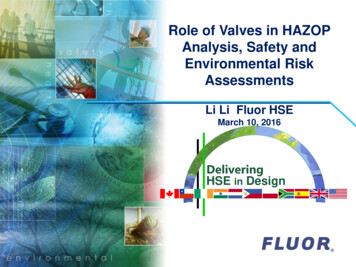
ADVANCES IN PROSTATE CANCER THERAPY:60 YEARS OF PROGRESS2010Firstimmunotherapy20052017High dose radiationreduces recurrence199419821970New surgerieshelp preservesexual functionRadioactive‘seeds’ proveneffective197020202010200020081996First drug for PCaresistant tohormone treatment1982Early roduced19601997Watchful Hormone therapy radiation improveswaitingsurvivalintroduced19901980New SoC fornewly diagnosedadvanced PCaEvidence fortargetedtherapies20122004New chemotherapyfor hormoneresistance PCaNew hormonetherapy foradvanced PCa2020Approval ofPARPi therapyfor mCRPC1966First standardchemotherapyregimenmCRPC, metastatic castrate-resistant prostate cancer; PARPi, poly ADP ribose polymerase inhibitor; PCa, prostate cancer; SoC, standard of careCancer Progress Timeline: Prostate Cancer (modified). Available from: ogress-timeline/prostate-cancer. Accessed, August 2020.Available from: tration-resistant-prostate-cancer . Accessed, August 2020.Available from: tant-prostate . Accessed, August 2020.8
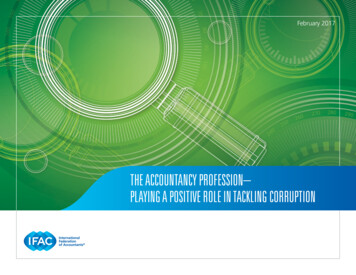
MAJOR PROGNOSTIC FEATURES OF PROSTATE CANCER 5-year survival is close to 100% in patientswith local or regional prostate cancerLoss of hormone sensitivity and metastasisrepresent two major negative prognosticevents in prostate cancerNew Cancer Diagnosis5-year OS rangeLocal or regional %mCRPC10-26%mHSPC, metastatic hormone-sensitive prostate cancer; OS, overall tecancer/statistics#: :text r.htmlMadan RA et al., https://pubmed.ncbi.nlm.nih.gov/18628467/;Carniero et al., https://pubmed.ncbi.nlm.nih.gov/27802009/Francini et al., https://pubmed.ncbi.nlm.nih.gov/30643173/Halabi et al., https://pubmed.ncbi.nlm.nih.gov/26951312/9
PROSTATE CANCER THERAPY:RAPID ADVANCES9 life-prolongingapprovals since 20102010FirstimmunotherapyDrug name2017New SoC fornewly diagnosedadvanced teEnzalutamideRadium 2232012New hormonetherapy foradvanced PCa2020Approval ofPARPi therapyfor mCRPCAR, androgen receptor;HRR, homologous recombination repair;MSI, microsatellite instabilityAll information available at: www.drugs.comApprovalDrug ClassAutologous cellularApril 2010immunotherapyJune etastatic PCa/mCRPCApril 2011 Anti-androgenmCRPCAug 2012May 2013AR inhibitorRadiopharmaceuticalPembrolizumabMay 2017Monoclonal antibodyDarolutamideApalutamideOlaparibJuly 2019Feb 2018May 2020AR inhibitorAnti-androgenPARPimCRPC, non-mCRPC, mHSPCmCRPC boneUnresectable/metastaticsolid tumours MSI highNon-mCRPCmHSPC/non-mCRPCHRR gene-mutated mCRPC10
PARPi: WHAT DO WE NEED TO KNOW? Which mutations confer sensitivity to PARPi? How common are these mutations in prostate cancer? How do we identify patients with these mutations? What is the current role of PARPi in prostate cancer?11
WHAT IS PARP INHIBITION AND HOWDO WE IDENTIFY PATIENTS?Prof. Emmanuel S. Antonarakis, MDProfessor of Oncology and UrologyJohns Hopkins University School of MedicineSidney Kimmel Comprehensive Cancer CenterBaltimore, Maryland12
DISCLOSUREProf. Emmanuel S. Antonarakis has the following relevant financial relationships to disclose: Research/Consulting: Amgen, Astellas, AstraZeneca, Bayer, BMS, Celgene, Clovis, Dendreon, Eli Lilly,ESSA, Genentech, GSK, Janssen, Johnson & Johnson, Medivation, Merck, Novartis, Qiagen, Sanofi,Tokai Stock/Patents/Salary: None13
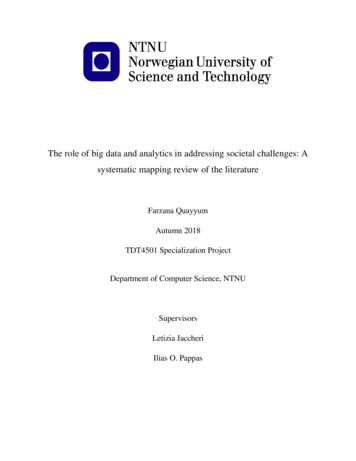
GENOMIC INSTABILITY IS A TARGETABLE HALLMARKOF CANCERHALLMARKS OF CANCERAR, androgen receptor;c-MET, c-MET tyrosine-protein kinase;HGF, hepatocyte growth factor;PARP, poly ADP ribose polymerase;VEGF, vascular endothelial growth factorHanahan D, Weinberg RA. Cell. 2011;144:646–74.14
ABERRANT DOUBLE-STRAND BREAK REPAIR: GENOMEINSTABILITYSpontaneous(Fork collapse)DSBsDSB, double-strand break15
DSB REPAIR: CELL CYCLEMG2G1SG, gap; M, mitosis; S, synthesisG016
DSB REPAIR: CELL CYCLEM“NHEJ”G2G1SG0DSBEnd joiningREPAIR“Error prone”NHEJ, non-homologous end joining17
DSB REPAIR: MEDIATED BY TWO PATHWAYS WITHDIFFERENT ERROR FREQUENCYM“HR”“NHEJ”G2G1DSBDSB resectionSG0DSBEnd joiningREPAIRStrand invasionBRCA1/53BP1No template “error prone”DNA synthesisREPAIRTemplate based “error free”53BP1, tumour suppressor p53-binding protein 1; BRCA1, breast cancer type 1 susceptibility protein; HR, homologous recombination18
DSB REPAIR: HR GENE DEFECTS REDUCE DNA REPAIROPTIONSM“HR”“NHEJ”G2G1DSBSG0DSBEnd joiningREPAIRNo template “error prone”BRCA2, breast cancer type 2 susceptibility protein19
DSB REPAIR DEFECTS:THERAPEUTIC EXPLOITATION IN CANCERM“HR”“NHEJ”G2G1DSBSDSBG0Helleday, Jackson, AshworthBryant HE, et al. Nature 2005; 434:913-917Farmer H, et al. Nature 2005; 434:917-92120
PARP INHIBITORS:THERAPEUTIC EXPLOITATION IN CANCERM“HR”“NHEJ”G2G1DSBSDSBG021
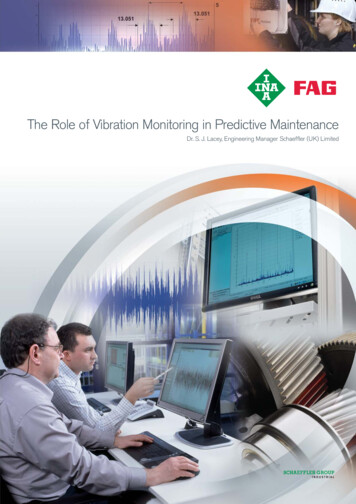
PARP INHIBITORS: ‘SYNTHETIC LETHALITY’REQUIRES BOTH REPAIR PATHWAYS TO BE BLOCKED BRCA: “copy editor”; HRR PARP: “spell check”; BERBERBERBERBERBERPARP is required for SSB repair (e.g. via BER)MOA – inhibiting SSB/BER is synthetic lethal with HRDBER, base excision repair; HRD, homologous recombination deficiency; MOA, mode of action; SSB, single-strand break22
PARP INHIBITORS:ENZYMATIC INHIBITION & PARP TRAPPINGMOA – trapping PARP is synthetic lethal with HRDDDR, DNA damage repair23
DDR MUTATIONS INMETASTATIC PROSTATE CANCERPrevalence and Screening24
CHANGING TREATMENT PATTERNS IN THE ERA OFPRECISION MEDICINETRADITIONAL MODEL OF DRUG DEVELOPMENTAAll patients receivestandard treatmentAPatientsBBClinical trialPRECISION MEDICINE MODELABPatientsMolecular/biomarkeranalysis of tumorCChoice of treatmentdependent upon biomarkerprofile of tumorDGoal: analytic validation of biomarker clinical validation of clinical utility and patient benefits with matched therapyKey contexts: prior therapy, histology, patient phenotype, comorbidities, costs, toxicitiesFröhlich H, et al. BMC Med. 2018;16(1):150; Redekop WK, Mlasi D. Value Health. 2013;16(6 Suppl):S4-9; Krzyszczyk P, et al. Technology (Singap World Sci). 2018;6:79-100.
2020 ACTIONABLE PATHWAYS, GENOTYPES AND PHENOTYPESAR-variant (e.g. AR-V7) driven CRPC:AR degraders, cofactor inhibitors, taxanes*AR-driven mCRPCInhibition of enhanced androgen synthesisAR N-term/DNABD inhibitors, PSMA targeted txGR inhibition, PARPi combinationsHRD CRPC (BRCA1/2,PALB2, others)MetastaticProstateCancerContext is critical:pattern of spread,symptoms, prior therapyPARPi based therapy,*IO combinationsmCRPCPD-1 basedimmunotherapy*CDK12 biallelic loss(tandem duplicatorgenotype) mCRPCPD-1 basedimmunotherapyMSIhi/dMMRAR Independent CRPC(NEPC, Double NegativeCRPC)Immune responsivesubsets of mCRPCDLL3 inhibition, combinationsImmunotherapyPlatinum chemotherapy*Currently approved therapies for prostate cancerCDK12, cyclin-dependent kinase 12; CRPC, castrate-resistant prostate cancer; DLL, delta-like ligand; dMMR, deficient mismatch repair; DNABD, DNA binding domain; IO, immuno-oncology; (m)CRPC, (metastatic) castrateresistant prostate cancer; MSIhi, microsatellite instability-high; NEPC, neuroendocrine prostate cancer; PALB2, partner and localizer of BRCA2; PARPi, poly ADP ribose polymerase inhibitor; PD-(L)1, programmed death (ligand)-1;PSMA, prostate-specific membrane antigen; Tx, therapyArmstrong CM, Cao AC. Asian Journal of Urology (2019) 6, 42e49; Antonarakis ES, et al. Prostate Cancer Prostatic Dis. 2016;19(3):231-41; Ponnumasy S, et al. Cancer Res. 2017;77(22):6282-98; Akora VK, et al. Cell. 2013December 5;155(6):1309-22; Vlachosergios PJ, et al. Curr Oncol Rep. 2017;19(5):32; Khemlina et al. 2015 S0305737215001462;Cheng JNCCN 2019 -p515.xml26
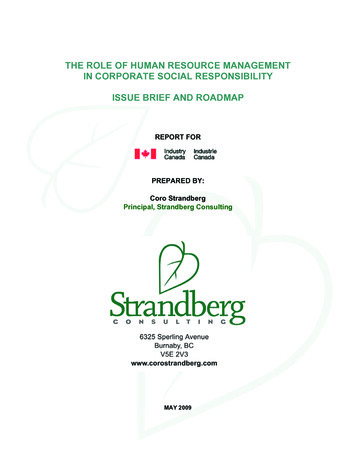
DNA REPAIR GENE ALTERATIONS (SOMATIC AND GERMLINE)ARE COMMON IN METASTATIC PROSTATE CANCER1-3GermlineSomatic 23% of mCRPCs harbor DNA repair alterations The frequency of DNA repair alterations increasesin metastatic disease vs. localized disease 12% of men with metastatic prostate cancerhave a germline DNA repair defectLOH, loss of heterozygocity1. Robinson D, et al. Cell. 2015;161:1215-28; 2. Pritchard CC, et al. N Engl J Med. 2016;375:443-53; 3. Antonakaris ES, et al. Eur Urol. 2018;74(2):218-25.27
BRCA2 CARRIERS WITH PROSTATE CANCER HAVE WORSEPROGNOSIS1,2NoncarriersaMediansurvival not reached after a median of 64-mo follow-up.CI, confidence interval; No., number; NR; not reached; y, years1. Castro E, et al. J Clin Oncol. 2013;31:1748-57; 2. Castro E, et al. Eur Urol. 2015;68:186-93.28
FAMILY HISTORY IS A REAL RISK FACTORA father or brother with prostate cancer doubles a man’srisk of prostate cancerA mother or sister with breast cancer diagnosedbefore age 50 significantly increases a woman’s risk ofbreast cancerA mother or sister with breast cancer can affect a man’srisk of prostate cancerChen et al., Prostate 2008 25/; Colditz et al., 2012 22/29
CASCADING IMPACT 12% of men withprostate cancer carryan inherited DNArepair gene mutation Full family history is important to collectduring the genetic evaluation In-person genetic counseling is the goldstandard Patients’ psychosocialneeds/preferences should dictate themode of counseling30
NCCN (V 2.2020) GUIDELINES FOR GENETIC TESTINGGermline Testing Germline genetic testing is recommended for patientswith prostate cancer and any of the following:Somatic Tumor Testing– High-risk, very high-risk, regional, or metastaticprostate cancer Recommend evaluating tumor for alterations inhomologous recombination DNA repair genes, such asBRCA1, BRCA2, ATM, PALB2, FANCA, RAD51D, CHEK2,and CDK12, in patients with metastatic prostate cancer– Ashkenazi Jewish ancestry Can be considered in men with regional prostate cancer– Family history of high-risk germline mutations(eg, BRCA1/2, Lynch mutation) Testing for microsatellite instability-high (MSI-H) ordMMR is recommended in patients with CRPC, andshould be considered in patients with regional orcastration-naïve metastatic prostate cancer– A positive family history of cancer The international Philadelphia Prostate Cancer Consensus Conference 2019 guidelinesrecommended a similar germline testing strategyGiri VN et al. J Clin Oncol. 2020;38(24):2798-2811. NCCN Guidelines for Prostate Cancer. Available tail.aspx?ebulletinid 3852. Accessed October 2020.31
HOW DO WE TEST?GermlineSomaticAcademic/In house32
CONCLUSIONS DDR mutations are a therapeutic target in metastatic prostate cancer PARPi work by the concept of “synthetic lethality” Both somatic and germline mutations related to DDR are common in metastatic prostate cancer Somatic and germline testing is recommended for all patients with metastatic prostate cancer andsome patients with high-risk regional and locally-advanced prostate cancer33
ROLE OF PARPi IN ADVANCEDPROSTATE CANCERProf. Andrew J. Armstrong, MDProfessor of Medicine, Surgery,Pharmacology and Cancer BiologyDirector of ResearchDuke Cancer Institute’s Center for Prostateand Urologic Cancers34
DISCLOSUREProf. Andrew J. Armstrong has the following relevant financial relationships to disclose: Research/Consulting: Pfizer, Janssen, Astellas, AstraZeneca, Merck, Bayer, Dendreon, BMS,Constellation, Beigene, Genentech/Roche, Clovis consulting and research support (to Duke Universityfor clinical trials/research) Stock/Patents/Salary: None35
MANY PARP INHIBITORS ARE BEING TESTED1PROPERTIES OF PARP INHIBITORS 1111OlaparibVeliparibNiraparibRucaparib1. Carney B et al.Nat Commun.2018;9:176;Talazoparib2. Available .August 2020.323.4434.5244.3380.8 Accessed,320.4MW3. Pilie PG, et al. Clin Cancer Res. 2019;25:3759-71.5 nM1.2 nM0.56 nM3.8 nM0.65 nMPARP1 IC50PARP2 IC50Trapping1Pamiparib2298.310.9 nM1 nM0.41 nM0.15 nM2.1 nM0.08 nM0.5 nM 3Pamiparib trapping potential estimated based on description as ‘potent’.IC50, half of maximal inhibitory concentration; MW, molecular weight; nM, nanomoles; PARP, poly-ADP ribose polymerase1. Carney B, et al. Nat Commun. 2018;9:176; 2. Available from: https://www.medchemexpress.com/Pamiparib.html. Accessed, August 2020.3. Pilie PG, et al. Clin Cancer Res. 2019;25:3759-71.36
ONGOING SINGLE AGENT CLINICAL TRIALS OF PARPi IN mCRPCPARPiClinical Trial No.Study overviewSettingTrial statusOlaparibNCT01682772Single arm, phase 2 trial of olaparib, predictive biomarker trialAdvanced castration resistant prostate cancerActive, not recruitingOlaparibNCT02987543Randomized phase 3 trial of olaparib vs enzalutamide orabirateronemCRPC who have failed prior treatment with a NHA withsomatic HRR mutationActive, not recruitingOlaparibNCT03047135Single arm phase 2 trial of olaparibNon-metastatic biochemically-recurrent PCa and a PSADTof 6 months and a minimum PSA of 1.0RecruitingOlaparibNCT03263650Randomized phase 2 of olaparib maintenance versusobservationAVPC 6 cycles of cabazitaxel and carboplatin ngle-arm phase 2 study of olaparib (IMANOL)mCRPC 6 cycles of docetaxel with CR/PR (RECIST 1.1) andPCWG3RecruitingTalazoparibNCT03148795Phase 2 single arm study of talazoparibmCRPC previous taxane-based chemotherapy andprogression on 1 NHAActive, not recruitingRucaparibNCT02952534Single arm phase 2 trail of rucaparib (TRITON2)mCRPC with evidence of HRR gene deficiencyActive, not recruitingRucaparibNCT02975934Phase 3 trial of rucaparib vs physician's choice of abirateroneacetate, enzalutamide, or docetaxel. (TRITON3)mCRPC with evidence of HRR gene deficiencyRecruitingRucaparibNCT03413995Single arm phase 2 trail of rucaparib (TRIUMPH)mHSPC with germline DDR gene mutationsRecruitingRucaparibNCT03533946Single arm phase 2 trail of rucaparib (ROAR)Hormone-sensitive PCa with ‘BRCAness’ gene defectsRecruitingNiraparibNCT02854436Single arm phase 2 biomarker/safety/efficacy (Galahad)mCRPC with progression taxane therapyActive, not recruitingPamiparibNCT03712930Single arm phase 2 trial of pamiparibmCRPC with HRR deficiencyActive, not recruitingHumeniuk, Zhang, Armstrong Cancer 2017; Virtanen et al., Genes 2019;10:565; https://clinicaltrials.gov/ct2/show/NCT01682772; https://clinicaltrials.gov/ct2/show/NCT02987543; tps://clinicaltrials.gov/ct2/show/NCT03263650; https://clinicaltrials.gov/ct2/show/NCT03434158; https://clinicaltrials.gov/ct2/show/NCT03148795; https://clinicaltrials.gov/ct2/show/NCT02952534; tps://clinicaltrials.gov/ct2/show/NCT03413995; https://clinicaltrials.gov/ct2/show/NCT03533946; https://clinicaltrials.gov/ct2/show/NCT02854436; https://clinicaltrials.gov/ct2/show/NCT0371293037
PROfound: STUDY DESIGN1 2:1Cohort ABRCA1, BRCA2, orATMn 245Olaparib 300 mg BIDn 162Physician’s choicen 83in Cohort A(alpha 0.05)Confirmed ORR by BICR inCohort A(alpha 0.05)rPFS by BICR in Cohort A B(alpha 0.05)ROpen-labelStatistical analysis2plan rPFS BICRPrimary endpointKey secondary endpointsKey Eligibility Criteria mCRPC with diseaseprogression on priorNHA (abiraterone orenzalutamide) Alterations in 1 ofany qualifying genewith a direct orindirect role in HRRStratification Factors Previous taxane Measureable diseaseUpon BICR progression,physician’s choice patientswere allowed to cross overto olaparibCohort BOther alterationsn 142Olaparib 300 mg BIDn 94Physician’s choicen 48Time to pain progression inCohort A(alpha 0.05)OS in Cohort OS in CohortA FinalA interim(alpha 0.01) (alpha 0.047)Primary endpoint: rPFS in cohort A (RECIST 1.1 and PCWG3 by BICR) Key secondary endpoints: rPFS (cohorts A B); confirmed radiographic ORR in cohort A; time to painprogression in cohort A; OS in cohort ABICR, blinded independent central review; BID, twice daily; HRR, homologous recombination repair; mCRPC, metastatic castration-resistant prostate cancer;NHA, new hormonal agent; ORR, objective response rate; OS, overall survival; PCWG3, Prostate Cancer Working Group 3; R, randomized; RECIST, Response Evaluation Criteria in Solid Tumours; rPFS, radiographicprogression-free survival1. de Bono J, et al. N Engl J Med. 2020;382:2091-102; 2. ESMO 2020, Presentation ID 610O.38
PROfound: PATIENT CHARACTERISTICS1Cohort ACohorts A and BCharacteristicsOlaparib(N 162)Control(N 83)Olaparib(N 256)Control(N 131)Median age at randomization, y (range)68 (47-86)67 (49-86)69 (47-91)69 (49-87)Age 65 y at randomization, n (%)108 (67)60 (72)174 (68)97 (74)Metastatic disease at initial diagnosis, n (%)Missing data38 (23)7 (4)19 (23)4 (5)66 (26)11 (4)25 (19)7 (5)105/157 (67)54/80 (67)183/251 (73)95/127 (75)8 (5)80 (49)60 (37)N/A5 (6)47 (57)24 (29)N/A8 (3)81 (32)62 (24)61 (24)5 (4)47 (36)24 (18)28 (21)Median PSA at baseline (IQR), 4.4)106.5(37.2-326.6)Measurable disease at baseline, n (%)95 (59)46 (55)149 (58)72 (55)Gleason score 8, n/total n (%)Patients with alterations in a single gene, n (%)BRCA1BRCA2ATMCDK12IQR, interquartile range; NA, not available; PSA, prostate-specific antigen; y, years1. de Bono J, et al. N Engl J Med. 2020;382:2091-102.39
PROfound: PATIENT CHARACTERISTICS1 (CONT’D)Cohort ACharacteristicMetas
EDUCATIONAL OBJECTIVES 1. Understand the MoA of PARP inhibition and its role in the treatment of prostate cancer 2. Understand the prevalence of DDR mutations in prostate cancer and be able to implement the testing strategies (specifically for somatic mutations) to predict if the prostate tumour is likely to respond to a PARPi or other tr