Transcription
2017 Optional State Supplementation(OSS) ProgramSCDHHSCommunity and Facility ServicesPO Box 82061801 Main1 StreetColumbia, SC 29202-8206
SCDHHS Department Roles & Contact Numbers Resident’s Medicaid StatusOSS or OSCAP PolicesEligibilityOSS Program Staff Develop policies Daily operations of budget,training, rates OSCAP contracts803-898-2590Approve or Deny OSS applicationInitiate CRCF-01 form and Cost ofLiving Adjustment (COLA) formsProvide answers for eligibilityquestions888-549-0820Update facility informationBilling/payment informationProvider Enrollment/ProviderService CenterMedicaid Claims Control System (MCCS) Update address,telephone numbers, etc. Direct Deposit Change of Ownership888-289-0709 option 4 TAD questionsEdit Codes questionsBillings/payment questionsRegister for training888-289-0709 option 32
Nurses ConsultantsVacantCounties: Lancaster, Marlboro,Chesterfield, Horry, Florence,Darlington, Dillon, MarionJai-Netta Montgomery, RN(803) 667-5598Jai-Netta.Montgomery@scdhhs.govCounties: Aiken, Lexington,Richland, Fairfield, Chester, York,EdgefieldSandra Jones, RN(803) 605-7129jonessa@scdhhs.govCounties: Williamsburg,Georgetown, Berkeley,Dorchester, Colleton, Jasper,Hampton, Allendale,Barnwell, Charleston,BeaufortCharlena Hunter, RN(803) 457-2656Charlena.Hunter@scdhhs.govCounties: Bamberg,Orangeburg, Calhoun,Clarendon, Sumter, Lee,KershawDarlene Newton, RN(864) 617-0108Regina.newton@scdhhs.govCounties: Oconee, Pickens,Greenville, Anderson, Abbeville,McCormickQuantina Williams, RN(864) 323-5627Quantina.Williams@scdhhs.govCounties: Spartanburg,Cherokee, Union, Laurens,Newberry, Greenwood, Saluda3
Program Contact InformationTerrell McMorris, MSWOSS Program CoordinatorTerrell.McMorris@scdhhs.govOffice: (803) 898-1810Alexis Martin, MBA, CPMOSS Program Managermartina@scdhhs.govOffice: (803) 898-1060Candice Smith-Byrd, CPCQuality Assurance Managersmithbc@scdhhs.govOffice: (803)-898-3372
WHAT IS OPTIONAL STATE SUPPLEMENTATION (OSS)? OSS is an entitlement program that is a state supplement to aperson’s Security Income [Supplemental Security Income(SSI)/Social Security Administration (SSA)]. The South CarolinaDepartment of Health and Human Services (SCDHHS) pays thedifference between the OSS rate and the Social Security payment. The purpose of this program is to provide reimbursement toenrolled CRCFs (also known as Assisted LivingFacilities) that provide room and board and a degree of personalcare for eligible consumers. OSS is NOT a Medicaid program; it isfunded at 100% state funding.5
OSS Program Facilities must accept the OSS entitlement amount as payment infull. Facilities may not charge a resident or a resident’s family for anydifference over and above the OSS entitlement amount – even ifthe family is willing to pay the difference for a private room. The additional payment would be considered income for theresident and could make the resident ineligible for OSS due toincome limitations.6
Resident Assessments Medical assessments are required for all OSS and OSCAPparticipants. Assessments will be performed by a SCDHHS nurse at the CRCFwhere the residents reside. The resident’s assessment will occurafter admission into the facility and every 24 months thereafter forOSS residents and every 18 months for OSCAP residents.7
Questions . What is Optional State Supplementation? What agency is responsible for Optional StateSupplementation?8
OSS Stepsfor NewAdmission
Step 1: Who is OSS Eligible? Be 65 years or older, or 18 years of age or older andblind or disabled Be a U.S. citizen or qualified noncitizen Have a Social Security number or file for one File for any other benefits to which they may beentitled Effective January 1, 2017 meet net income limit of 1,420 Can’t exceed resource limit of 2,000 for anindividualQUICK FACTSNumber of Consumers3,338 (OSS & OSCAP)49% Female & 51% MaleAverage Age: 63CRCF Medicaid enrolledfacilities: 313Average Income: 811Recurring Income :SSA: 43%SSI: 59%Top 5 Primary esHyperlipidemiaDementia10
Step 2: OSS Check Eligibility5. Enter the one of the following in the fields indicated:Medicaid I.D.; SSN and Date of Birth; or Name and Date ofBirth along with the Date of Service (auto populates withtoday’s date).Note: The Web Tool will return SSN information only if yousearch eligibility using SSN.6. Click the Check Eligibility button. The EligibilityVerification Inquiry: Selection Summary screen will appear.Place a check mark in the box beside the beneficiary’sMedicaid ID number.1. Visit The Web Toolhttps://portal.scmedicaid.com/7. Click the Display button. The Eligibility Verification2. Enter your username and password Results screen will appear which contains the eligibility3. From the Menu, click Eligibility,information of the beneficiary in question.4. From the submenu choose Single– If you wish to check eligibility for another recipient,Query, to retrieve the Eligibilityclick the Back link. This will return you to the originalVerification Inquiry screen.screen.– If you wish to add this individual to your Beneficiary11List, click the Add Beneficiary link.
Step 3: What documentation is needed whencompleting an OSS application?Forms 3401 –No active Medicaid 3400A has active 00.pdf 1728 is receiving SSI only Send Medicaid EligibilityApplications to:Fax: 888-820-1204orMail: SCDHHSCentral MailPO Box 100101Columbia, SC 292021. 30 day bank statement from previousmonth2. Life Insurance policy (cash value anddividends) as of the 1st of the month3. Burial Contract4. Signed Authorized Representativeform(Form 1282)5. Client has to sign Form 943(Information for Release Form)6. Health Insurance Card (Medicare, VA,Pension) and award amounts7. Current recurring income amountfrom SSA/Pension8. Property owner have correct address12)and tax notice (intent to return home
LTC Workers List of Long Term CareCoordinators (LTCCs)responsible for serving countiesidentified in their regionthroughout the state.The state is divided into four (4)regions.To determine your points ofcontact, use the following mapand identify the county in whichyour facility is located. Next,locate your LTCCs as listed. Forexample, if your facility islocated in Richland County, youshould contact our Region 2team, Leighann and MelanieRegionLTC WorkerEmailPhoneNumber1 – BlueTeena BixlerBixlerT@scdhhs.gov864-250-58971 – BlueKathi DixonDixonK@scdhhs.gov864-229-52582- -30932 – 3- GreenPerry FossFoss@scdhhs.gov843-584-40663- GreenJoAnn KearseKearseJ@scdhhs.gov843-740-59254- 4- RedMekoWilliamswillmeko@scdhhs.gov803-435-4305x229 13
124314
Contacting Eligibility When you need to know the status of an OSSapplication please call 888-549-0820. Inform the customer service representativeyou are calling to check on the OSS status andgive them the date in which you applied. The OSS program area cannot provide youwith the status of your application.15
Step 4: CRCF-02 FormAdded Faxnumber toCRCF-02 Form
Step 5: Initial CRCF-01 FormHappy FeetHappy Feet17
Step 6: Add Resident to TADJohn Doe123456789002/1728 The Initial CRCF 01 form must be attached to the monthly Turn AroundDocument (TAD) and add the new resident’s name to the last page of theTAD. A copy is kept for the facility’s files.18
CurrentResident StatusChange Steps
When an OSS resident transfers To your facility fromanother CRCF?1. Verify that the resident is already participating in the OSSprogram by checking Web Tool.2. Complete a Status Change CRCF-01 Form. CompleteSection I and submit to Terrell McMorris atTerrell.McMorris@scdhhs.gov or Fax to 803-255-82093. Allow 5 business days for a return forms . Please keep acopy for your records.20
When an OSS resident transfers From your facility toanother CRCF? Complete the following steps:1. Complete a Status Change CRCF-01 Form Sections I andIII.2. Send the CRCF-01 form to Ms. Terrell McMorris via emailat Terrell.McMorris@scdhhs.gov or fax to 803-255-82093. Once a signed CRCF-01 Form is received, remove theresident’s name from the TAD by placing an X in thedelete column on the TAD and submit a copy of thesigned CRCF-01 Form.22
When a resident terminates from your facility1. Complete the CRCF-01 Form Sections I and III (B).2. Select the reason for termination and enter the date oftermination.3. Submit a copy of this form with your TAD and place an X in thedelete column on the TAD and fax copy to eligibilitydepartment 888-820-1204.4.No Signature is needed for terminations on the CRCF-01 Form.
Income ChangeHappy Feet06/07/1726
Optional Supplemental Care For Assisted Living ParticipantsOSCAP27
What is Optional Supplemental Care For Assisted LivingParticipants? The Optional Supplemental Care For Assisted Living Participants(OSCAP) service provides additional reimbursement to facilities thatprovide assistance with personal care for OSS residents who meetthe medical criteria required for participation. OSCAP gives additional reimbursement of 207 per month for eachqualified resident. Current OSCAP rate is 1, 627
Step 1: Does my OSS resident meet the Medical Necessity Criteria? Two (2) functionaldependencies One (1) cognitive and one(1) functional dependency Limited assistance withtwo (2) or moreActivities of Daily Living(ADLs) Limited assistance with one(1) or more ADLs in additionto a cognitive impairment29
How to apply for OSCAP?1. Must be OSS approved beforeyou can apply for OSCAP.2. To complete OSCAP referral 3. When applying for OSCAP,select OSS as the Reason forReferral. In the comment boxtype OSCAP.* OSCAP has not been added as a reason forreferral. The correct choice is OSS, but be sureto enter OSCAP in the comment box. Anyquestions? Best way to access referral is togoogle search “CLTC electronic referral” andselect the option with Phoenix in thedescription.30
What will the DHHS Nurse need to complete the OSCAPAssessment? A SCDHHS nurse will visit your facility to assess referredOSS participants for OSCAP. The SCDHHS nurse will need: Copy of Medication Administration Report(MAR)/Physicians Orders Copy of Individual Care Plan (ICP) Resident’s chart Recent height, weight, and vital signs Interview with direct care staff Interview resident OSCAP assessments are every 18 months, unless thereis a change in the level of care.31
Status Change Form When should I expect to receive the Status Change Form?The SCDHHS nurse for your region will send the form following herassessment via fax, email, or USPS mail. Do I attach this form to my TAD?You only attach the status form to the TAD if there is anauthorization or termination date. A copy should be kept for yourrecords. Should I keep a copy?A copy of the most current status form must be kept in the participant’s record.
Service Plan A service plan will be individualized for each OSCAPparticipant by the SCDHHS nurse. Service plans will be mailed, emailed, or faxed tothe facility following the assessment and level ofcare determination. Service plan must be used as guidance to reviseindividual care plans and to create the ResidentMonthly Task Log. A copy must be kept in the resident’s file andavailable to any SCDHHS staff upon request.34
Service Plan35
Service PlanThis section is used to completethe Resident Monthly Task Log
OSCAP Task Logs The initial OSCAP Task Log must be created by the CRCFlicensed nurse. The CRCF nurse must review, revise, sign anddate each monthly task log at least every 90 days. Must be completed on all OSCAP residents and kept on record. All direct care staff in contact with residents must initial allcompleted tasks. Administrator or designee must sign and date weekly. CRCF nurse must write a detailed nurse’s note/summary everythree (3) months including: height, weight, vital signs,functional/cognitive dependencies, any behavioral problemsand any medical complications following face to faceinteraction.37
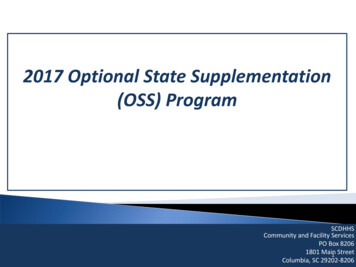
Resident Monthly Task LogName:John 04052017060708Month:091011121314 Lifted manually/mechanically Transfer aid Weight bearing Wheelchair/Cane/Walker x Other person wheelsE Put on prosthesis or brace WanderingBathing Does not bathe appropriately In/out of tub/shower Lower body/Upper body x CueingLDressing Buttons/zippers/snaps/tying Inappropriate dressing/layers Step by step guidance x21Room No.LRefuses to change/reappliesdirty Put on socks/shoesLevel of Care Key: L Limited E Extensive T Total15161234567890Medicaid No.July171819202122232425262728293031
Resident Monthly Task LogBladder &Bowel All direct care staff in contact with resident should initial allcompleted tasks. Scheduled toileting planx Pads/briefs usedLDD DDDD Bowel programCognitive Memory problem(s) Decision making capacity Mood problem(s)Diet Behavior problem(s) Good (75%) Fair (50%) Poor (25%) Refused Supplements Level of Care Key: L Limited E Extensive T Total Signatures and Initials of all Resident Assistants providing assistance this month. Initials DDSignaturesDonald Duck InitialsSignatures
Resident Monthly Task Log Weight & Vital Signs Date & Results Weight Blood Pressure Temperature Pulse Respiration Sugar Monitoring Date & ResultsDate & ResultsDate & ResultsI certify the information on this form is correct and documented services were provided.Date & ResultsDate & ResultsThe CRCF nurse must write a detailed nurse’s note/summary every 3 monthsincluding:height,weight,vitalsigns, functional/cognitivedependencies, any behavioralproblemsand any medicalcomplications following face to face interaction. Administrators Signature:Week 1Date:Administrators Signature:Week 2Date:Administrators Signature:Week 3Date:Administrators Signature:Week 4Date:I certify the information on this form is correct and documented services were provided.Nurse Signature:Progress Note(s) – Please date and initial each note.Date:
Individual Care Plans (ICP) Must be in each resident’s file/chart. Must be reviewed and updated every six (6) months. “No changes” isan unacceptable update. All ICPs/six (6) month review must be reviewed, updated, signed anddated by the CRCF nurse. Must be signed by the administrator, resident, or the responsibleparty/sponsoring agency. If the resident is unable to sign, then anexplanation must be written on the ICP. Must be reflective of the resident’s service category (OSCAP, OSS,Hospice, waiver) and current condition. Redeveloped at least every 24 months from the date of the initial ICP.41
Individual Care Plans (ICP)42
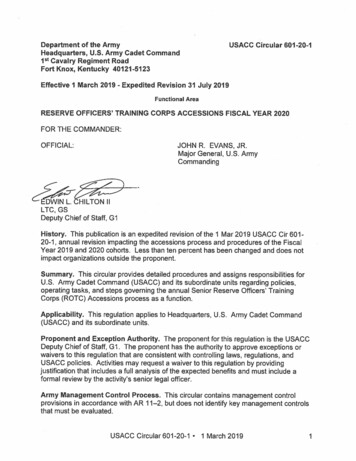
Individual Care Plans (ICP)John C. ResidentResident SignatureDate:Responsible Party/Sponsor[ ] Family chose not to participateJanie Administrator / Nurse Betty,RN - DATEFacility RepresentativeSent letter on (copy attached) or Called on & spoke with
Individual Care Plans (ICP)INDIVIDUAL CARE PLAN REVIEW[]Six (6) Month Review[]Change in NeedComments:“No changes” is not an acceptable update.John C. ResidentResident SignatureDATEDate:Responsible Party/SponsorJanie Administrator / Nurse Betty,RN - DATEFacility RepresentativeSent letter on or Called on & spoke with44
CRCF Nurse Duties OSCAP approved facilities are require to employ or contract with alicensed nurse (either a Licensed Practical Nurse or and RegisteredNurse). The ICP must be reviewed, revised or updated, signed and dated bythe nurse every at least every six (6) months. The initial Monthly Task Log must be created by the CRCF nurse.The CRCF nurse must review, sign and date all Monthly Task Logs atleast every 90 days. Revisions to the Monthly Task Logs must bemade by the CRCF Nurse as needed. The Nurse must sign and datethe Monthly Task Logs when revisions/updates are made.45
CRCF Nurse Duties The staff person responsible for supervision of direct care staff inthe CRCF nurse’s absence should be trained and determinedcompetent and capable by the CRCF nurse.A quarterly summary of each OSCAP participant in the CRCF mustbe written, dated, and signed by the CRCF nurse, following a faceto face evaluation of the resident. The summary must include:vitals, weight, functional/cognitive dependencies, any behavioralproblems, and medical complications.All CRCF nurses are required to attend any scheduled OSCAPtrainings or meetings provided by SCDHHS.46
OSCAP and Hospice Services Beneficiaries of Hospice and OSCAP may only receive personalcare through one service or the other; therefore, they mustchoose either Hospice or OSCAP. An OSCAP participant residing in a CRCF has the right to choosewhich service they receive.47
OSCAP Provider Requirements Licensure in good standing by the SouthCarolina Department of Health andEnvironmental Control (SCDHEC) OSS Participation Agreement Facility documentation of resident funds andPNA Facility notification to the SCDHHS andMCCS of admissions, discharges, transfers,and deaths within 72 hours Monthly processing of the OSS payments Meet specific basic requirements of theAmericans with Disabilities Act (ADA)including wheelchair accessibility Have a minimum of six (6) hours relevant inservice training per calendar year, in additionto SCDHEC required training Must designate, in writing, a licensedfull time facility administrator and anadministrator’s designeeMust notify SCDHHS within 10 businessdays in the event of a change in theadministrator, OSCAP nurse, address,phone number, or an extended absenceof the administratorEnsure the nurse is in good standingwith the South Carolina Board ofNursingEnsure that resident to staff ratios areconsistent with SCDHEC regulation at alltimesThe facility must not be without nursingcoverage for more than 90 days
Questions . How are OSCAP services documented? How often must the CRCF nurse review, sign and dateall Monthly Task Logs ?49
OSS & OSCAP Billing & Payment50
Rates for 2017Date of ServiceJanuary 2017Payment DateMarch 03, 2017OSS and OSCAP RatesOSS Rate : 1,420PNA: 67Facility Payment: 1,353 permonthOSCAP Rate: 1,627PNA: 67Facility Payment: 1,560 permonthFebruary 2017April 7,2017March 2017May 5, 2017April 2017June 2, 2017May 2017July 7, 2017June 2017August 4, 2017July 2017September 1, 2017August 2017October 6, 2017September 2017November 3, 2017October 2017December 1, 2017November 2017January 5, 2018December 2017February 2, 201851
Personal Needs Allowance OSS beneficiaries who receive recurring income of SSI only areallowed to keep 67 per month for personal needs. Eligible beneficiaries who have income other than SSI are allowedto keep an extra 20 for personal needs, bringing their total to 87. PNA increases by 2 each year, if there is a COLA. Please refer to the CRCF-01 for each beneficiary to determinetheir PNA amount.52
TAD Reminders Changes to the TAD, MUST be submitted with a CRCF-01 Form to supportthe action made on the TAD. OSS providers have 13 months from the date of the signed CRCF-01 Formto submit the form for billing. Any forms past the 13 month timeframemay not be processed. Failure to submit a CRCF-01 Form could result in delayed payment. Don’t send CRCF-01 form in with TAD until you havecompleted the form from eligibility with effective date,recurring income, PNA amount, signature and date. Please verify the mailing address on the TAD to ensure the address iscorrect. If the address is incorrect, please contact Terrell McMorris atTerrell.McMorris@scdhhs.gov with the correct information.53
TAD Mailing AddressClaims Receipt – CRCFClaims SectionPost Office Box 67Co
Georgetown, Berkeley, Dorchester, Colleton, Jasper, Hampton, Allendale, Barnwell, Charleston, . MBA, CPM OSS Program Manager martina@scdhhs.gov Office: (803) 898-1060 . Admission . Number of Consumer

![[ OPTIONAL ] CASE COLLATOR · 90667 LM3231 COMPLETE .](/img/4/91ga8yoa-ts.jpg)