Transcription
Medical First Response ProgramMedical Control ProtocolsStandard First Aid (SFA)First Medical Responder (FMR)Emergency Medical Responder (EMR)January, 2017
Medical First ResponseProtocolsJanuary 2017Document AuthorsDr. Kevin Hanrahan, Medical Director, MFR Program, Alberta Health ServicesJohn Hein, Strategist, MFR Program, Alberta Health ServicesEmily Barclay, Administrator, MFR Program, Alberta Health ServicesContributing AuthorsBarody, Blaine – MFR Program Manager, AHSCampbell, Jamie – Black Diamond Fire DepartmentEvans, Jennifer – Redwood Meadows Emergency ServicesEvans, Rob – Redwood Meadows Emergency ServicesManz-Henezi, Jodi – Alberta Health ServicesMartens, Keri – Lake Louise FireMeikle, Dave – Black Diamond Fire DepartmentMikkelsen, Lisa – Black Diamond Fire DepartmentMoore, Chad – MFR Strategist, AHSMunn, Susan – Lake Louise FirePaksi, Tyler – Redwood Meadows Emergency ServicesPirie, Mike – Airdrie Fire DepartmentRabel, Garth – Airdrie Fire DepartmentRoe, David – High River Fire DepartmentSchaaye, Gregg – M.D. of Foothills Fire DepartmentProvincial MFR MCPs Working GroupCaralho, Pierre – Alberta Health ServicesCohoe, Shauna – Alberta Health ServicesDonelon, Becky – Alberta College of ParamedicsGarofalo, Sergio – Alberta Health ServicesKugelstadt, Duane – Alberta GovernmentLandaker, Kelly – Alberta Health ServicesMartens, Keri – Lake Louise FirePedersen, Steen – Alberta Health ServicesPirie, Mike – Airdrie Fire DepartmentRead, Chris – Alberta Health ServicesRoe, Dave – High River Fire DepartmentWright, Alissa – Alberta Health ServicesContributing DocumentCalgary Fire Department – Medical Protocols – (November 23, 2010*)*Used with PermissionDr. Kevin Hanrahan – Medical Director, Calgary Fire DepartmentStephen Nicholl, Calgary Fire DepartmentDebbie Bateman, Calgary Fire DepartmentContact:Medical First ResponseAlberta Health ServicesGrande Prairie EMS Station10710-97 StreetGrande Prairie, ABT8V 7G6Email: mfr@albertahealthservices.caToll Free: 1-866-786-14402 PageAlbertaMFR.ca
Medical First ResponseProtocolsJanuary 2017Disclaimer and CopyrightAlberta Health Services (AHS) Emergency Medical Services (EMS) is committed toproviding high quality and safe patient care. AHS EMS has developed this set ofMedical First Response (MFR), Medical Control Protocols (MCPs). The MCPs containbest standard practice taken from evidence and expert informed care and treatmentinformation that is specifically intended for the use of medical first responders in Albertaand the physicians who provide medical oversight for these agencies. EMS reserves theright at its own discretion to make changes, including the correction of errors andcomplete revisions to the MCPs.At the same time, the information is presented “as is” and its use by externalorganizations or individuals is solely at their own risk. AHS EMS, its employees andphysicians accepts no responsibility for any modification or redistribution or use ofthe MCPs and is not liable for any actions taken by individuals based on the informationprovided, or for any inaccuracies, errors or omissions in these MCPs.2015 Alberta Health Services – All rights reserved in relation to these MCPs. Withoutlimiting the reservation of copyright, no person shall reproduce, store in a retrievalsystem or transmit in any form or by any means (electronic, mechanical, photocopying,recording or otherwise) part or the whole of these MCPs without the prior writtenpermission of Alberta Health Services.Please note that AHS does not retain any liability for the external use of these MCPs ortheir maintenance outside of the MFR Program. The written protocols have been madeavailable for viewing by the public. It is assumed that your use will be to enhance thecare you provide and is not for resale or redistribution purposes.Be advised that these MCP’s will continue to be reviewed and updated at regularintervals to ensure that they meet the above standards.Dr. Ian PhelpsSenior Medical DirectorAlberta Health ServicesEmergency Medical Services3 PageAlbertaMFR.ca
Medical First ResponseProtocolsJanuary 2017Table of ContentsAlgorithm 1Standard Approach and Ongoing Assessment . 5Algorithm 2Airway Control – Conscious Patients. 6Algorithm 3Airway Control – Unconscious Patients . 7Algorithm 4Altered Level of Consciousness . 8Algorithm 5Burns . 9Algorithm 6Cervical-Spine Assessment . 10Algorithm 7Chest Pain . 11Algorithm 8Control of External Bleeding . 12Algorithm 9CPR Adults . 13Algorithm 10CPR Children (1 to 8 years) . 13Algorithm 11CPR Infants (Less than 1 Year) . 15Algorithm 12Death On-Scene . 16Algorithm 13Drowning / Near Drowning . 17Algorithm 14Dyspnea (shortness of breath) . 18Algorithm 15Environmental Emergencies – Cold Related . 19Algorithm 16Environmental Emergencies – Heat Related . 20Algorithm 17Hypoglycemia . 21Algorithm 18Obstetrics and Gynecological – Vaginal Bleeding . 22Algorithm 19Obstetrics and Gynecology – Childbirth . 23Algorithm 20Obstetrics and Gynecology – Neonatal Resuscitation . 24Algorithm 21Obstructed Airway – Adults/Children . 25Algorithm 22Obstructed Airway – Infants (Birth – 1 Year) . 26Algorithm 23Poisoning. 27Algorithm 24Seizure . 28Algorithm 25Shock . 29Algorithm 26Stroke . 30Algorithm 27Trauma Assessment. 31Algorithm 28Overdose – Opioid. 324 PageAlbertaMFR.ca
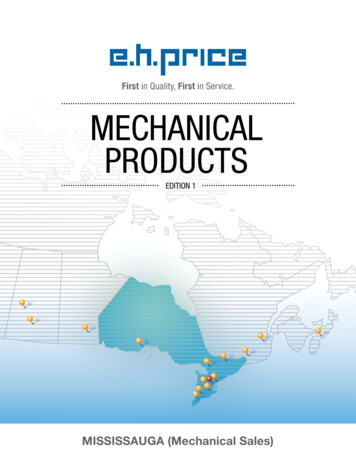
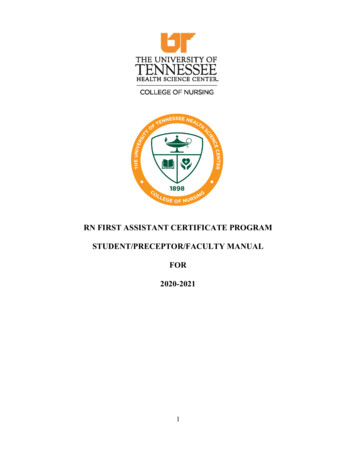
Medical First ResponseProtocolsJanuary 2017Algorithm 1Standard Approach and Ongoing AssessmentSFAFMREMRInitial Scene Assessment· Scene Safety· Additional Resources· Crime Scene?· Note Mechanism of Injury and Number of PatientsSFAFMREMR*SFAIf trained and equippedSFA*FMREMRFollow Infection PreventionPerform Hand HygieneDon Appropriate PPEPerform Primary Patient Assessment· Assess mental status· Assess A,B,C,Ds· Consider Spinal Motion Restriction· Expose and examine priority areas· Identify priority patients· Record Vital SignsPerform Primary Set of Vital Signs on all Patients*50th Percentile ValuesPulseRespirationsBlood Pressure(Systolic)SPO2GCSTemperatureNewborn110 – 160 b/min35 – 60 / min60 – 76 mm Hg94% – 100%n/a35.5 – 37.5 C1 Yr Old100 – 130 b/min30 – 50 / min86 mm Hg*94% – 100%1535.5 – 37.5 C6 Yr Old70 – 100 b/min18 - 30 / min95 mm Hg*94% – 100%1535.5 – 37.5 C10 Yr Old65 – 100 b/min12 – 25 / min103 mm Hg*94% – 100%1535.5 – 37.5 CAdult60 – 100 b/min12 – 20 / min(90 – 140 mm Hg)94% – 100%1535.5 – 37.5 CNoGo to Appropriatealgorithm5 PageAlbertaMFR.ca
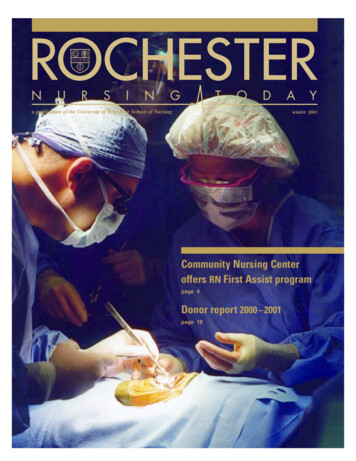
Medical First ResponseProtocolsJanuary 2017Airway Control – Conscious PatientsAlgorithm 2SFAFMREMRStandard Approach andOngoing AssessmentIs patientconscious?Yes*SFAIf trained and equippedIs theairway clear?NoNoYesAdequateRate, rhythmand quality ofrespirations?Go toUnconsciousPatientsalgorithmGo sider spinal motion restrictionAdminister O2 if SpO2 94% onroom air (RA)SFAFMREMRConsider spinal motion restrictionEnsure open airwaySFAFMREMRTreat for ShockProvide comfort/reassuranceMonitor patient’s LOC and ABCSFA*FMREMRSuction airway as neededBVM ventilationAdminister O2 if SpO2 94% on RASFA*FMREMRSecondary surveyHistory-SAMPLERecord Vital SignsSFAFMREMRTreat for shockProvide Comfort/reassuranceMonitor patients LOC and ABCSFAFMREMRPlace in recovery position if noevidence of traumaReassess every 5 minsuntil EMS arrivesSFA*FMREMRSecondary surveyHistory-SAMPLERecord Vital SignsSFAFMREMRPlace in recovery position if noevidence of traumaReassess every 5 minsuntil EMS arrives6 PageAlbertaMFR.ca
Medical First ResponseProtocolsJanuary 2017Algorithm 3Airway Control – Unconscious PatientsSFAFMREMR*SFAIf trained and equippedSFAFMREMRInitiate and maintainmanual C-Spine control IfneededYesIs the airwayclear?Rate, rhythmand quality ofrespirations?AdequateIs pulse present?Standard Approach andOngoing AssessmentNoNoGo toObstructedAirwayalgorithmInadequate or absent**NoGo to CPRalgorithmIs pulse present?YesYesSFAFMREMRConsider spinal motion restrictionEnsure open airwaySFAFMREMRConsider spinal motion restrictionEnsure open airwaySFA*FMREMRSecondary SurveyHistory-SAMPLERecord Vital Signs, Obtain BGLSFA*FMREMRSuction airway as neededBVM ventilation with OPAAdminister O2 if SpO2 94% on RASFAFMREMRPlace in recovery position if noevidence of traumaReassess patient every 5 min untilEMS arrivesEMRConsider NPASFA*FMREMRSecondary SurveyHistory-SAMPLERecord Vital Signs, Obtain BGLSFAFMREMRPlace in recovery position if noevidence of traumaReassess patient every 5 minsuntil EMS arrives**In the unlikely event there is a pulse but no breathing, provide ventilations 1 every 5-6 seconds7 PageAlbertaMFR.ca
Medical First ResponseProtocolsJanuary 2017Algorithm 4Altered Level of ConsciousnessSFAFMREMRStandard Approach andOngoing AssessmentIs patientbreathing?YesNo*SFAIf trained and equippedYesIs pulsepresent?Go toAirway ControlUnconsciousPatientalgorithmGo to CPRalgorithmNoDetermine LOCUnconsciousAltered/Decreased LOCSFAFMREMRConsider spinal motion restrictionEnsure open airwaySFAFMREMRConsider spinal motion restrictionEnsure open airwaySFA*FMREMRMaintain AirwayAdminister O2 if SpO2 94% on RASFA*FMREMRMaintain airwayBVM ventilation with OPAAdminister O2 if SpO2 94% on RAEMRConsider NPASFAFMREMRTreat for shockProvide comfort/reassuranceSFA*FMREMRSecondary SurveyHistory / SAMPLERecord Vital Signs, Obtain BGLSFAFMREMRPlace in recovery position if noevidence of traumaReassess patient every 5 min untilEMS arrives8 PageAlbertaMFR.ca
Medical First ResponseProtocolsJanuary 2017Algorithm 5BurnsSFAFMREMRStandard Approach andOngoing Assessment*SFAIf trained and equippedIs patientbreathing?NoGo toAirway ControlalgorithmYesSFAFMREMRRemove risk of further burnsIf necessary decontaminatefor 15 minSFAFMREMRTreat for shockProvide comfort/reassuranceKeep patient warmSFA*FMREMRMaintain airwayAdminister O2 if SpO2 94% on RAIs burnless than 10%body surfaceYESSFAFMREMRCool burnCover with clean, moist dressingNOSFAFMREMRCover with clean, dry non-stickdressingSFA*FMREMRSecondary SurveyHistory / SAMPLERecord Vital SignsSFAFMREMRReassess patient every 5 min untilEMS arrives9 PageAlbertaMFR.ca
Medical First ResponseProtocolsJanuary 2017Algorithm 6SFAFMREMRSFAFMREMRCervical-Spine AssessmentStandard Approach andOngoing AssessmentConfounding Factors that mayobscure or invalidate the findings ofa examination include:·Acute stress reaction·Intoxication·Altered level of consciousness·Distracting injuries·Communication difficultiesIn these situations complete spinalmotion restriction is indicated.Maintain C-spine control (if able)while assessing need for spinalmotion restrictionAge is greater than 65 orHigh risk factor for spinal injury* orParesthesia in extremitiesNOYesLow riskfactor for spinal injury whichallows safe assessment ofrange of motion**NoYesAble to voluntarilyRotate neck 45 left andrightNo*High risk factors for spinal injuryinclude but not limited to:·Fall greater than or equal to1m / 5 stairs·Axial load to head·Speed greater than 100 kph,rollover, ejection·Motorcycle / ATV recreationalvehicle (e.g. snowmobile)collision·Bicycle collision**Low risk for spinal injury include:·Simple rear-end MVC(Excludes patient being pushedinto oncoming traffic, hit by bus/large truck, rollover, hit by highspeed vehicle)·Ambulatory at any time·Delayed (not immediate) onsetof neck pain·Absence of midline C-spinetendernessPerform spinal motion restriction ifpractical to do soYesSFAFMREMRNo spinal motion restriction needed10 P a g eAlbertaMFR.ca
Medical First ResponseProtocolsJanuary 2017Algorithm 7Chest PainSFAFMREMRStandard Approach andOngoing Assessment*SFAIf trained and equippedYesGo toTraumaalgorithmSigns of traumaNoSFA*FMREMRMaintain AirwayAdminister O2 if SpO2 94% on RASFA*FMREMRAdminister ASA 160mg PO* ifsuspected cardiac causeSFAFMREMRTreat for shockProvide comfort/reassurancePlace patient in position of comfortMinimize patient activitySFA*FMREMRSecondary SurveyHistory-SAMPLE-OPQRSTRecord vital signsSFAFMREMRReassess Patient every 5 min untilEMS arrives11 P a g eAlbertaMFR.ca
Medical First ResponseProtocolsJanuary 2017Algorithm 8Control of External BleedingSFAFMREMRStandard Approach andOngoing AssessmentSFAFMREMRApply direct pressureElevate extremity if possibleSFAFMREMRTreat concurrently withshock protocolProvide comfort / reassuranceSFA*FMREMRSecondary SurveyHistory-SAMPLERecord vital signsSFAFMREMRReassess patient every 5 minuntil EMS arrives*SFAIf trained and equipped12 P a g eAlbertaMFR.ca
Medical First ResponseProtocolsJanuary 2017Algorithm 9CPR AdultsSFAFMREMRStandard Approach andOngoing AssessmentConsider the following:· Do Not Resuscitate Orders· Goals of Care· Personal Directive*SFAIf trained and equippedSFAFMREMRVisual scan to assess for signs of“breathing – gasping” (max 10 sec)Is MRSFAFMREMRSFAFMREMRMonitor LOC/ABCSecondary SurveyHistory-SAMPLERecord vital signs, Obtain BGLPlace in recovery positionIf no evidence of traumaReassess patient every 5 minuntil EMS arrivesSFAFMREMRIs pulse present(max 10 sec)NoGive 1 breath every 5 secondsCheck pulse every 2 minutesSFAFMREMRCAB SequenceStart Chest Compressions30 Compressions and 2 BreathsSFA*FMREMRManage airway prnBVM ventilation with OPAAdminister O2EMRConsider NPASFAFMREMRPrepare AEDUse as soon as availableSFAFMREMRContinue CPR and AED useuntil EMS arrives13 P a g eAlbertaMFR.ca
Medical First ResponseProtocolsJanuary 2017Algorithm 10CPR Children (1 to 8 years)SFAFMREMRStandard Approach andOngoing AssessmentConsider the following:· Do Not Resuscitate Orders· Goals of Care· Personal Directive*SFAIf trained and equippedSFAFMREMRVisual scan to assess for signs of“breathing-gasping” (max 10 sec)Is A*FMREMRSFAFMREMRSFAFMREMRSFAFMREMRMonitor LOC/ABCManage airway prnBVM ventilation with OPAAdminister O2Secondary SurveyHistory / SAMPLEPlace patient in recovery position ifno evidence of traumaRecord vital signs, Obtain BGLReassess patient every 5min until EMS arrivesSFAFMREMRGive 1 breaths every 3secondsCheck pulse every 2minutesAssess Pulse (max 10 sec)YesIs pulse present(max 10 sec)NoSFAFMREMRCAB SequenceStart Chest Compressions30 compressions / 2 breathsSFA*FMREMRManage airway prnBVM ventilation with OPAAdminister O2SFAFMREMRPrepare AEDUse after 5 cycles of 30:2 CPR(approx 2 min)SFAFMREMRIf second rescuer present switchto 15 compressions and 2 breathsSFAFMREMRContinue CPR and AED useuntil EMS crew arrives14 P a g eAlbertaMFR.ca
Medical First ResponseProtocolsJanuary 2017Algorithm 11CPR Infants (Less than 1 Year)SFAFMREMRStandard Approach andOngoing Assessment*SFAIf trained and equippedSFAFMREMRConsider the following:· Do Not Resuscitate Orders· Goals of Care· Personal DirectiveVisual scan to assess for signs of“breathing-gasping” (max 10 sec)YesIs or LOC / ABCSFA*FMREMRManage airwayBVM ventilation with OPAAdminister O2SFA*FMREMRSecondary SurveyHistory / SAMPLERecord vital signs, Obtain BGLSFAFMREMRPlace in recovery position if noevidence of traumaSFAFMREMRReassess patient every 5 minuntil EMS arrivesSFAFMREMRGive 1 breaths every 3secondsCheck pulse every 2minutesYesAssess Pulse (max 10 sec)Is pulse present(max 10 sec)No or rate is less than 60/minwith signs of poor perfusionSFAFMREMRCAB SequenceStart Chest Compressions30 compressions / 2 breathsSFA*FMREMRManage airway prnBVM ventilation with OPAAdminister O2SFAFMREMRPrepare AEDUse after 5 cycles of 30:2 CPR(approx 2 min)SFAFMREMRIf second rescuer present switchto 15 compressions and 2 breathsSFAFMREMRContinue CPR and AED useuntil EMS crew arrives15 P a g eAlbertaMFR.ca
Medical First ResponseProtocolsJanuary 2017Algorithm 12Death On-SceneSFAFMREMRStandard Approach andOngoing AssessmentIs there evidenceof presumed death?DRIED*YesNoDO NOT RESUSCITATESecure the scene and do notdisturb it unnecessarilyIs there a document towithhold resusitation?**Yes*DRIEDDecapitationRigor MRConfirm patient’sidentitySFAFMREMRProvide support forbystandersSFAFMREMRSecure the sceneNoGo to CPRalgorithm**DNR / Goals of Care Directive/Personal DirectiveDocument must be physically present. Verbal orders are not validIf in doubt, do not delay resuscitative efforts16 P a g eAlbertaMFR.ca
Medical First ResponseProtocolsJanuary 2017Algorithm 13Drowning / Near DrowningSFAFMREMRStandard Approach andOngoing Assessment*SFAIf trained and equippedYesIs there a pulse?NoSFAFMREMRConsider spinal motion restrictionEnsure open airwaySFA*FMREMRSuction airway as neededBVM ventilation with OPAAdminister O2 if SpO2 94% on RAEMRConsider NPASFAFMREMRTreat concurrently with shock protocolProvide comfort/reassuranceSFA*FMREMRSecondary SurveyHistory-SAMPLERecord Vital Signs, Obtain BGLSFAFMREMRPlace in recovery position if noevidence of traumaReassess patient every 5 min untilEMS arrivesGo to CPR algorithm17 P a g eAlbertaMFR.ca
Medical First ResponseProtocolsJanuary 2017Algorithm 14Dyspnea (shortness of breath)SFAFMREMR*SFAIf trained and equippedSFA*FMREMRManage airway prnAdminister O2 if SpO2 94% on RASFAFMREMRTreat concurrently with shock protocolProvide comfort / ReassuranceSFAFMREMRTREATMENT INTERVENTIONSMinimize patient activityPlace patient in position that allows forgreatest ease of breathing (usually sitting up)Pulmonary Edema orUnknown CauseSFA*FMREMRStandard Approach andOngoing AssessmentAnaphylaxisSFA*FMREMRHigh flow O2Medication AssistEpi-penPrescribed dosageSFA*FMREMRSecondary SurveyHistory-SAMPLERecord Vital Signs, Obtain BGLSFAFMREMRReassess patient every 5 min untilEMS arrivesBronchospasmSFA*FMREMRMedication AssistPrescribed dosage18 P a g eAlbertaMFR.ca
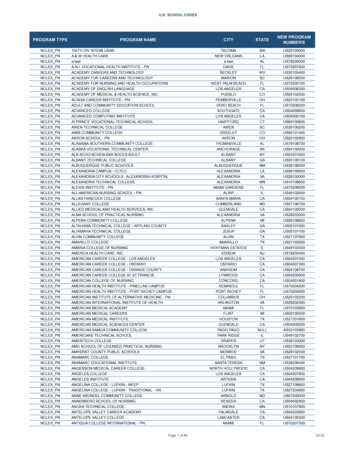
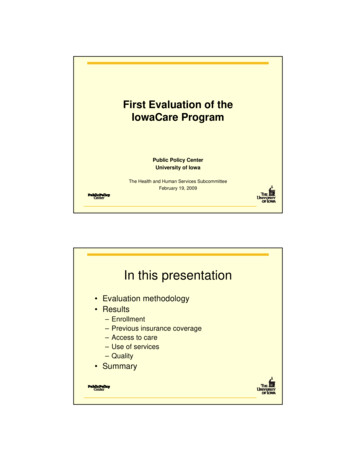
Medical First ResponseProtocolsJanuary 2017Algorithm 15Environmental Emergencies – Cold RelatedSFAFMREMRStandard Approach andOngoing AssessmentSFAFMREMRTREATMENT INTERVENTIONSRemove from cold environmentPrevent further heat lossHandle hypothermic patients gentlyYesSFA*FMREMRManage airway prnAdminister O2if SpO2 94% on RASFAFMREMRTreat concurrently withshock protocolProvide comfort/reassuranceSFA*FMREMRSecondary SurveyHistory-SAMPLERecord Vital Signs, Obtain BGLSFAFMREMRIs patientconscious?NoIs Pulse PresentYesNoGo to AlteredLevel ofConscio
Emergency Medical Responder (EMR) January, 2017. Medical First Response Protocols January 2017 2 P a g e AlbertaMFR.ca Document Authors Dr. Kevin Hanrahan, Medical Director, MFR Program, Alberta Health Services John Hein, Strategist, MFR Program, Alberta Health Services