Transcription
QUALIT Y 2021 MedicalHome PartnershipA Program Guide to Rewarding Quality Outcomes
Table of ContentsKey Principles of the Medical Home Partnership (MHP) . . . . . 3Population Health Management . . . . . . . . . . . . . . . . . . . . . . . . 4Care Coordination Model . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5Program Evaluations: Quality and Cost Improvement . . . . . . 6MHP Benefits to the Practice . . . . . . . . . . . . . . . . . . . . . . . . . . . 7MHP Benefits to the Patient . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7Practice Responsibilities . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8BlueCross Responsibilities . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10MHP Provider and Network Participation . . . . . . . . . . . . . . . . 12MHP Attribution . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12MHP Care Coordination Fee . . . . . . . . . . . . . . . . . . . . . . . . . . 15MHP Utilization Management Program . . . . . . . . . . . . . . . . . 15Appendix . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15(A) Quality Measures(B) Quality Scorecard Example(C) Utilization Measures(D) Utilization Scorecard ExampleMedical Home Partnership (MHP) Aim:Better outcomes and value for BlueCross BlueShield of Tennessee membersand customers through partnerships with selected primary care providersto establish the three components:1) care coordination2) quality improvement3) utilization management1
In 2009, BlueCross began working with primarythe primary focus for outreach and engagement.care practices to implement the Patient-CenteredCurrently, the BlueCross PCMH program is theMedical Home (PCMH) program. A PCMH is alargest in the state with 27 primary-care partners,team-based model of providing care, designed toand approximately 360 individual locations,support providers in improving and maintaining1,758 providers and approximately 325,500the health of their patients, or BlueCross members.attributed members seeking care withinThe model of care highlights the individuals on thea PCMH primary care practice.health care team and the importance of theBeginning in 2020, the PCMH program becamepatients’ role in their own health. Additionally, thethe Medical Home Partnership (MHP), a populationgoal is to improve coordination of care among thehealth management program designed to improvemedical system, community, family and patientcare coordination, quality, and utilization.resulting in better outcomes and patientThe MHP program, emphasizes a populationsatisfaction. From 2009 to 2018, the BlueCrossapproach to prevention (primary, secondaryPCMH program emphasized disease managementand tertiary), wellness/health promotion andand primary prevention screenings. Specificdisease management.chronic conditions such as diabetes, heart disease,respiratory conditions and cancer screenings were2
Key Principles of the Medical Home Partnership:The principles of the Medical Home Partnership align with the patient-centered modelof care, developed by the American Academy of Pediatrics (AAP), and include:›Physician-directed medical practice:The personal physician leads a practiceteam to take responsibility for the ongoingcare of the patient.›Care is coordinated and integrated acrossall elements of the health care system:Care is facilitated by data registries andinformation technology, such as EMR or HealthInformation Exchange platforms, to ensure thatpatients receive the best quality care when andwhere they need it (hospitals, health agencies,nursing homes, etc.).3›Quality and safety:Evidence-based medicine andclinical outcomes are measuredand monitored to check for continuousquality improvement in patient care.›Enhanced access to care:Access is enhanced through openscheduling, expanded hours, andemail/telephone consultations.
Population Health ManagementAccording to the National Institute of Health, Population Health Management is the shift in care providedat an individual level to improve managing and paying for health care services for a defined population.The MHP model of care focuses on an attributed, risk stratified population in which care gaps areidentified and managed by an embedded nurse care coordinator. BlueCross’ proprietary analytics andreporting capabilities allow for better care coordination and chronic disease identification to ensureeducation, self-management and decision support skills are taught and transferred to the BlueCrossmember. Program outcomes include quality and utilization improvement, measured by practicescorecards and an annual program evaluation. Member satisfaction is measured annually with a survey.Population HealthManagement Diagram4
Care Coordination ModelCare coordination is the foundation of the Medical Home Partnership. It involves organizing patient careactivities and sharing information among all participants involved in the patient’s care to achieve safe,appropriate and effective quality care. The main goal of care coordination is to satisfy the patient’s needsand preferences while delivering high-quality health care in a cost-effective manner. The result is a highlyengaged patient.The Care Coordination Model, developed by Group Health Cooperative, looks at care coordination from theperspective of a patient-centered model of care. It considers the major external providers and organizationswith which the patient interacts: medical specialists, community service agencies, and hospital andemergency facilities. These providers and organizations contribute to successful referrals and transitionsin care. All patient referrals and transitions should meet the six Institute of Medicine goals of high-qualityhealth care, including care that is:›Timely – Transitions and consultative services are provided without delays.›Safe – Planned and managed referrals and transitions prevent harm to patients.›Effective – Referrals and transitions are centered around scientific knowledge and properly executed.›Patient-centered – Patient needs and preferences are met through responsivereferrals and transitions.›Efficient – Referrals and transitions avoid unnecessary or duplicative services.›Equitable – Quality of service does not vary by the personal characteristics of patients.THE CARE COORDINATION MODELProviders receive theinformation they needwhen they need it.Practice knows the statusof all referrals/transitionsinvolving its panel.Patients report receivinghelp in coordinating care.BlueCross-embedded care coordinators have the unique opportunity to help coordinate care for patientswho are BlueCross members. Care coordinators are integrated and should be considered part of thepractice health care team. They assist with coordinating services, such as specialist appointments andcommunity resources, as well as, transitions in care.5
Program Evaluations: Quality and Cost ImprovementOver the past ten-years, collaboration with the2018 Evaluation Resultsparticipating providers in the Patient-CenteredMedical Home Program has resulted in significant›An average 4.86 return on investment (ROI)compared to non-PCMH practices›Approximately 4.8M in cost savings›An average 0.8% reduction in inpatient (IP)admissions per 1000 and an average 1.3%reduction in ER visits per 1000›Statistically significant higher qualitycompliance scores on 22 out of 27 key HEDIS measuresquality and cost improvement. The annualPCMH results, outlined below, are the resultof a collaborative partnership between thepractices and BlueCross. With the addition of theMHP Utilization Management Program in 2020,additional improvements in the health outcomesof BlueCross members are expected.2019 Evaluation Results›An average 13.76 return on investment (ROI)compared to non-PCMH practices2017 Evaluation Results›Approximately 15 M in cost savings››An average 3.5% reduction in pharmacy costand 2.25% reduction in medical benefit costAn average 3.59 ROI compared to non-PCMHpractices›Approximately 2.4M in cost savings›A 5.7% reduction in IP admissions per 1000 anda 2.9% reduction in ER visits per 1000›Statistically significant higher qualitycompliance scores on 14 out of 27 key HEDIS measures outcomes of BlueCross members areexpected.›Statistically significant higher qualitycompliance scores on 23 out of 27 keyHEDIS measuresHEDIS is a registered trademark of NCQA.6
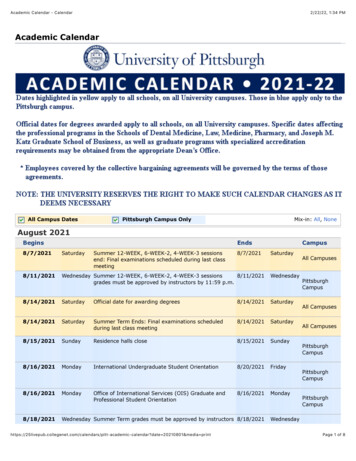
Shared Benefits§ Motivates employees to be more activeparticipants in their healthImproved quality of outcomes§ Care focused on prevention and wellnessto keep patients healthy longer§ Helps guide employees to higher value care§ Fewer ineffective or redundant testsand procedures§ Healthier employees result in moreproductive workforce with fewer absencesGreater member satisfaction§ Higher patient scores in overall provider satisfaction§ Patients have expanded access to care and better accessMHP Benefitsto the Practiceto their own informationPCMH Provider BenefitsBetter dataBetter dataBestpracticesBestpractices§ Sharing best practices with peers›§› Supportand resourcesto aidEnablessharingofinbesttransformation to patient-centeredpractices across the state § Financial› rewardscareOpportunitiesfor coordinatedto becare§ More productive and rewarding timereimbursed for qualitypatients and resources› withSupport§ Access to more comprehensive,actionable data on patientsAccess to more§ Data-driven models for staffing,comprehensive,systems and health IT to enablebetterdataintegrationacross careactionableon patientssettings›More sustainableMore sustainablereimbursement methodsreimbursementmethods§ Opportunitiesto be reimbursed forquality careto aid in transformationto a patient-centered modelData-driven modelsto enable better integrationacross care settingscare›Opportunities to bereimbursed for improvementin utilization›Financial opportunitiesfor coordinated careMHP Benefits to the PatientSimplified, personalizedhealth care›Care coordination bringsmore personal andcontinuous interaction withproviders, so patients get thecare they need to stay healthy.Improved quality of outcomesGreater member satisfaction›Care is tailored for thepatients’ needs andpreferences.›Patients have expandedaccess to care and betteraccess to their owninformation.›Care coordination results infewer ineffective or redundanttests and procedures.›Multiple mechanisms forcommunicating with theirprovider through newtechnology.7
Practice Responsibilities1. The practice will identify a physician champion whose responsibilities include, but are not limited to:››Providing visible and sustained leadership›to lead specific strategies to improve quality,lower medical cost and improve patientsatisfaction›Ensuring that the MHP utilization efforthas the time and resources needed tobe successful››Distributing provider scorecards anddiscussing best practices among colleagues›Educating providers and staff on carecoordination and the role of the BlueCrossMHP care coordinatorAttending and participating in joint quarterlyMHP program meetings with the BlueCrossMHP medical director and clinical teamMonitoring and tracking performance data andoutcomes of the MHP program initiativesSupporting collaborative care activitiesto improve quality2. The practice agrees to use the BlueCross technology platform to identify the targeted population.›Stipend Care Coordinators are required to complete BlueCross compliance training annually.Failure to comply will result in loss of funding for the stipend care coordinator resource(s).›Failure to use the Care Coordination platform may result in termination of MHP contract.3. The practice agrees to participate in collaborative quality and cost initiatives(e.g. utilization reduction) through joint meetings and process improvement activities.8
4. The practice agrees to identify an NCQA champion to work with the BlueCross NCQA consultant andachieve NCQA PCMH recognition.›BlueCross requires that all MHP practicesachieve NCQA recognition and maintainannual submission requirements. Practices must meet the minimumrequirements to achieve NCQAAnnual Recognition in order tomaintain current eligibility withinthe BlueCross MHP program. For practices new to NCQA PCMHrecognition, BlueCross requires allpractices to achieve recognition within thefirst 18 months and enroll in QPass withinsix months of signing the MHP contract. In the event of a merger or acquisition,the Professional Provider will have 18months to obtain such recognition forany new locations.Note: It is recommended that each MHP practiceuses the BlueCross NCQA discount code whenapplicable. This code can be obtained by yourBlueCross NCQA consultant.5. The practice will provide a workstation, including a desk and chair, for the MHP care coordinatorwithin a clinical space of the practice. Clinical space is not considered administrative space or off-sitelocations where BlueCross members are not seeing the providers.The entity employing the care coordinator willbe responsible for supplying the following:›Practice desktop computer orlaptop computer›Two monitors (BlueCross canprovide, if needed)››EMR access and training on EMR›Remote access to EMR›Access to printer within practice›Access to fax within practice›Practice phoneKeyboard (BlueCross can provide, if needed)6. The practice will allow the MHP stipend care coordinator to attend onboarding training, monthly carecoordinator meetings and the BlueCross annual meeting.9
BlueCross Responsibilities1. BlueCross provides an MHP clinical team to work with the practice team.›BlueCross has a clinical team consisting of a Clinical Operations Manager, Nurse Supervisorand Corporate Medical Director that partners with practices to improve quality outcomes.2. BlueCross provides a technology platform that supportsthe Medical Home Partnership.›BlueCross provides a care coordination, reporting and analytical platform for the MHP program.Through a defined attribution process, BlueCross members are attributed to a specific providerpanel based on claims history. The technology allows care coordinators to review a patientpopulation by practice, provider, chronic condition and/or utilization triggers such as ER visits. Thetechnology platform also allows the MHP care coordinators to read notes and care plans, and refermembersto internal BlueCross complex case managers needing additional support.3. BlueCross provides an employed or stipend MHP care coordinatorfor the practice.Care coordinator responsibilities include, but are not limited to:››››Assisting with coordination of patient careneeds and education on chronic conditions(telephonic and face-to-face). Patients CaregiversBuilding relationships and trust with PCPsand their clinical teams as well as otherspecialists within the MHP practiceFocusing on moderate and highIP/ER utilizersCare transition management10›Ensuring medications prescribedat discharge have been filled and patientis taking medications properly›Coordinating care for symptommanagement›Coordinating preventive care›No PCP visit within the year – reaching outto schedule appointment and ensure visitcompleted›Completing a comprehensive assessment todetermine plan of care
4. BlueCross provides New Employee Orientation and Training.BlueCross provides training support for all employed and stipend care coordinators. The educationprogram focuses on:›New Employee Orientation(for hired employees only)›Communication Techniques and Strategies: Motivational interviewing Shared decision-making›The Care Coordination Model›The Chronic Care Model›Chronic Condition management training›Transitions in Care›Annual BlueCross Compliance Training›BlueCross Quality Program – HEDIS 101›Quarterly BlueCross Security Training5. BlueCross provides a Care Coordination Fee to the Practice.›BlueCross runs claims data monthly to attribute patients to a specific provider within the MHPpractice. BlueCross pays a monthly Care Coordination fee to the practice. The amount is based onthe Exhibit 4 in the MHP Agreement.6. BlueCross provides NCQA PCMH Recognition Support.›BlueCross provides an on-site resource,the NCQA Consultant, to assist with theNCQA recognition process.›BlueCross provides funding to purchase theNCQA web-based tool to guide providersthrough the accreditation process and paysthe initial application fee.›BlueCross will reimburse forannual recertification basedon the MHP Agreement.›BlueCross requires that all MHP sites achieveNCQA recognition and maintain recognitionwith annual recertification by NCQA on thewebsite listed below: es/patient-centeredmedical-home-pcmh/Note: If a practice is enrolled in both BlueCross MHP and the Division of TennCare PCMH, NCQAreimbursement will be discussed individually with the practice.11
MHP Provider and Network ParticipationBlueCross recognizes that certain administrative functions are necessary to run the operations of theMHP program. These functions include patient attribution, data exchange, analytics and reporting. MHPis a program designed to include primary care providers exclusively.Primary Care Physician (PCP) ClassificationFor purposes of the MHP Program, PCP classification includes the following provider specialties whoseprimary credentialing by BlueCross is as a primary care provider:›Family Medicine›Nurse Practitioner – Adult Acute Care›Family Medicine – Adolescent Medicine›Nurse Practitioner – Adult Health›Family Medicine – Adult Medicine›Nurse Practitioner – Family›Family Medicine – Geriatric Medicine›Nurse Practitioner – Gerontology›General Practice›Nurse Practitioner – Pediatrics›Internal Medicine›Nurse Practitioner – Primary Care›Internal Medicine – Adolescent Medicine›Pediatrics›Internal Medicine – Geriatric Medicine›Pediatrics - Adolescent Medicine›Nurse Practitioner›Physician Assistant – MedicalNote: The PCP classification may differ by MHP component. For QCPI, please refer tothe QCPI Addendum and QCPI Program Guide for PCP Classification.MHP Provider Network ParticipationThe BlueCross MHP program applies to the networks according to the Exhibit 1 of the MHP Agreement.MHP AttributionPatient Attribution MethodologyAttribution. The BlueCross attribution methodology differs by MHP component; for instance, attributionto one component of MHP doesn’t always mean a member will be attributed to all components. Theattribution methodology for each MHP Program component is set forth below. BlueCross will apply theattribution methodology consistently among providers participating in the MHP program.Attribution is at the member level and is based on face-to-face office or telehealth visits over an18-month look-back period. Members are attributed to the provider with whom they’ve had the mostvisits during the look-back period. If there is a tie, then the member is attributed to the provider they’veseen most recently.12
A. Quality Component. BlueCross BlueShield of Tennessee members1 who receive health benefitsthrough a Commercial network (i.e., Blue Network PSM, Blue Network SSM or other futurecommercial networks) will be attributed to a PCP for the purposes of the QCPI.Attribution is at the member measure level. Members are identified and attributed to a single PCP whomeets one of the QCPI PCP Classified Provider Types and who has seen the member the most withinan 18-month look-back period. If there is a tie, the member will be attributed to the PCP they have seenmost recently.Four measures, Appropriate Treatment for Children with Upper Respiratory Infection (URI), AppropriateTesting for Children w/Pharyngitis (CWP), Avoidance of Antibiotic Treatment in Adults with AcuteBronchitis (AAB), and Use of Imaging Studies for
› EMR access and training on EMR › Remote access to EMR › Access to printer within practice › Access to fax within practice › Practice phone 6 . The practice will allow the MHP stipend care coordinator to attend onboarding training, monthly care coordinator meetings and the BlueCross annual meeting .