Transcription
MEDICATIONADMINISTRATION BASICSThe purpose of this section is to help learnersunderstand the basics of medication administrationand their responsibility in implementing a safemedication administration system.KEY TERMS: Medication errors Prescription drugs Over-the-counter (OTC) drugs Medication routes Food and drug interactions Side effectsOBJECTIVES:After completing this section the learner will be able to: Describe the types of medication errors;List the medication routes;Demonstrate how to read a prescription label;Demonstrate how to read OTC drug label;Understand how foods can interact with drugs;Give examples of types of side effects that canoccur with medications.
MEDICATIONADMINISTRATIONINTRODUCTIONAdministering medication involves more than giving residents their medications.Handing out a pill is just a small part of the process. The AFH rules require thatAFH owners and their caregivers are able to demonstrate an understanding of eachresident’s medication administration schedule, the reason the resident is taking themedication, the effect of the medication and any potential side effects.The AFH provider is responsible for implementing and maintaining a safemedication administration process for all residents. Making sure you and yourcaregivers are well trained in proper medication administration will reduce thepotential for medication errors. Note: Be sure substitute caregivers are welltrained in safe medication administration.Medication errors are a common problem. A recent study estimated that, inone year, incorrect use of medications resulted in more than 9 million hospitaladmissions and more than 18 million emergency room visits.1Listed below are a few examples of common medication errors: Giving the medication at the wrong time; Not giving a scheduled medication; Giving an incorrect dose; Giving a medication that has been discontinued;Ensuring Quality Care Chapter 11 Medication AdministrationWhen you are caring for up to five residents who may be taking as many as 1015 different medications (including over-the-counter), the task of administeringmedications becomes complex.1
Giving a resident medication intended for someone else; Improperly stored medication; Missing or incomplete documentation.You are the first line of defense for the residents in your care. Understandingand implementing safe medication administration and keeping accuraterecords is an important responsibility of the AFH provider.A medication administration process includes: Obtaining medical orders; Transcribing medical orders on to the medication administrationrecord (MAR); Verifying medical orders against the MAR; Dispensing and delivering/administering; Monitoring and documenting; Storing; and Disposing of discontinued, unused, contaminated or expired medication.Be sure you and your staff understand the orders and can perform the tasksrequired to dispense the medications. If you or your caregivers need training, youmust get that training before giving the medication. Tasks such as taking a pulsemay need to be performed before giving a medication. Checking a pulse or bloodpressure (BP) before giving a medication is common in AFH.Medication administration is part of every AFH’s daily responsibilities. It is importantto routinely work with health care professionals to ensure safe and effectivemedication use by residents. The individual’s primary health care practitioner,prescribing practitioner, registered nurse and pharmacist are all part of ateam of health care professionals that can help you with the medicationsthat have been prescribed to a resident living in your home. Be sure to2
talk with them about your concerns or questions each time a medication isordered or refilled.A prescribing practitioner can be any health care practitioner with theauthority to prescribe treatment or medications who is involved with the careof the resident. In addition to the resident’s primary health care practitioner,other prescribing practitioners may include a dentist, podiatrist, specialist,psychiatrist or urgent care or emergency room physician or nurse practitioner.BASICS OF MEDICATIONSMEDICATION CATEGORIESMedications can be categorized into groups by the way they are marketed or sold.The most common categories are drugs that require a prescription and drugs thatcan be purchased over-the-counter. Prescription drugs are medications obtained from a pharmacist bywritten order from a prescribing practitioner. They are also referred toas prescribed drugs. Over-the-counter (OTC) drugs are widely advertised and can be purchasedby anyone without a prescription. OTC medications can cause serious sideeffects used alone or when combined inappropriately with each otheror with prescribed medication.Ensuring Quality Care Chapter 11 Medication AdministrationThis section will review types of medications, how medications are delivered(routes), how to read prescription and over-the-counter labels, drug interactions,side effects and other information about medication use.3
»» Common problems caused by OTC medications: They may change the effect of prescribed medications, forexample, making them stronger or less effective. As a result,the doctor may mistakenly increase/decrease the dose of theprescribed medication. The medications may mask symptoms of disease. Forexample, antacids taken for upset stomach may cover upwarning symptoms of ulcer disease, which could delaydiagnosis and treatment. They could act similarly to a prescribed medication. Combined,the medications may lead to drug overdose symptoms. The medications could interact with other OTC andprescribed medications. They may create unwanted side effects.Prescription and over-the-counter drugs are either sold as generic or brand-namedrugs. Generic medications are sold using a common name, instead of by a brandname. Aspirin is a common term (generic) used for acetylsalicylic acid, which is thename of the chemicals used. Bayer is a brand name for aspirin. Achromycin isthe brand name for the antibiotic tetracycline (generic). Generic drugs usually costless and can be requested from the pharmacist. However, a resident’s prescribingpractitioner may not approve a generic substitution because some generic drugsvary in their chemical properties.A drug may be classified by the chemical type of the active ingredient or by theway it is used to treat a particular condition. Each drug can be classified into one ormore drug classes. Common drug classifications include cardiovascular, respiratory,urinary, gastrointestinal, endocrine, antipsychotic, anti-anxiety and analgesics.4
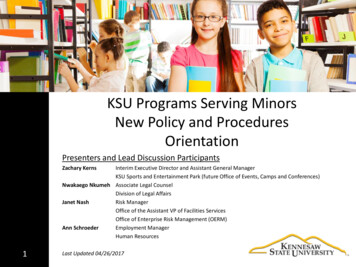
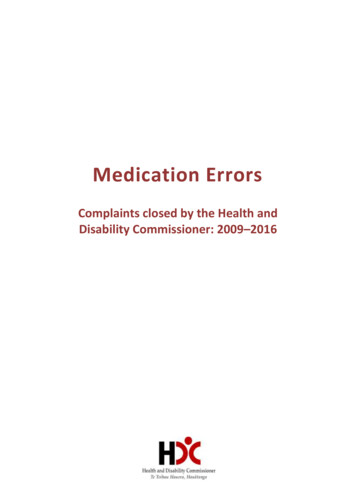
HOW TO READ A PRESCRIPTION LABELImportant in-depth information is available on the prescription label. Eachprescription label contains the same information, which is highlighted in theexample below. However, the format or design of the label may look ative-medicine/how-to-read-drug-labels.cfmEnsuring Quality Care Chapter 11 Medication AdministrationPrescription label*5
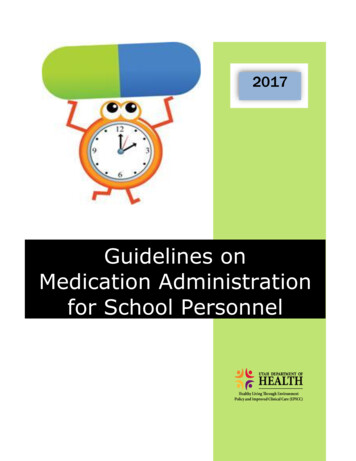
HOW TO READ AN OTC LABELEach OTC medication has a drug fact label on the bottle. Below is an example ofthe information found on a drug fact label for OTC medications:OTC drug fact e-medicine/how-to-read-drug-labels.cfm6
MEDICATION ROUTESMedication can be introduced into the body through many routes. The prescribingpractitioner will write one of the following routes for the medication to be given: G-tube/j-tube; Intramuscular (IM) injection*; Intravenous (IV)*; Nasal (drops or inhalers); Opthalmic (eye); Oral (taken by mouth); Otic (ear); Rectal; Sublingual (under the tongue); Transdermal (via skin); Vaginal.*An AFH provider or caregiver cannot administer intramuscular and intravenous medications. Anurse or other qualified health professional must give them.AFH providers are expected to correctly administer all medications, except for IMor IV medications, to the resident regardless of route. OAR Chapter 851 Division47 (Oregon Board of Nursing) prohibits RNs from delegating IM medications.Additionally, OAR Chapter 411 Division 50 (AFH rules) prohibits the delegation ofIV medications. IM and IV medications must be administered by a nurse or otherqualified health professional.Subcutaneous medication, for example insulin, can only be administered by theAFH provider or caregivers after an RN has provided appropriate training andEnsuring Quality Care Chapter 11 Medication Administration Subcutaneous injections (requires an RN to delegate);7
completed the delegation process. Refer to the section on RN delegation found inChapter 3 for additional information.If a resident has a medication ordered to be administered through the IM or IVroute, administration arrangements must be made with a licensed practitioner.Several options are available to assure residents receive their IM or IV medication: Make arrangements with the resident’s primary health care practitioner; Request a referral to a home health agency or, if the resident is on hospice,make arrangements with the hospice agency; or Contract with a private nurse to perform the task.The guidelines on the following pages provide basic information on how toadminister certain types of non-oral medications. If you are unsure or have anyquestions about how to administer any medication, contact the pharmacist or yourconsulting RN for assistance. Improper medication administration is considered amedication error.Source: – APhA Special Report: Medication Administration Problem Solvingin Ambulatory Care. Washington, DC: American Pharmaceutical Association;1994-9.e.8
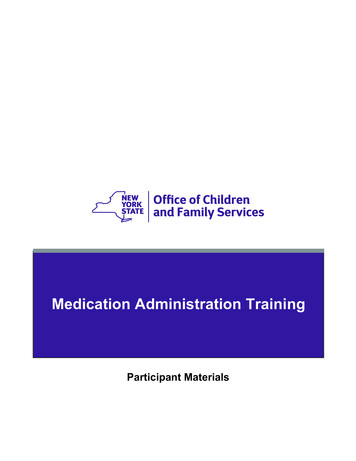
ChapterRelatedtoandColdsandAllergySection11VII s of ColdsGuidelines for Administering EardropsTABLE 30-1Guidelinesfor administeringeardropsMost peopledo not havecomplications fromcolds. However, complications of colds may be severe and, rarely, life1. Wash yourhands with soapand warmwater; thendry leearthoroughly.infections, bronchitis, bacterial pneumonia, and exacerbaand dry the outside of the ear, taking caretions2.ofCarefullyasthmawashor chronicobstructive pulmonary disease.not to get water in the ear canal.3. Warm eardrops to body temperature by holding the container ofin thepalm of your hand for a few minutes. Do notTreatmentColdswarm the container in hot water. Hot eardrops can causeear pain,nausea, and dizziness.TreatmentGoals4. If the label indicates, shake the container.Sinceis noknowncureproventreat5. thereTilt yourhead(or havetheorpatienttiltprophylactichis or her head)toment forgoalinofdrawingtherapyA.isOrto liereducethecolds,side astheshowndownbothersomewith theaffected ear up as shown in drawing B. Use gentle restraint,symptoms.if necessary, for an infant or a young child.General Treatment ApproachThe mainstays of therapy include rest and adequate fluidintake. If a patient desires to self-treat, symptom-specifictherapy with single-entity products is recommended (Figure11-1).10 Most cold symptoms are present sometime duringthe course of the cold; however, symptoms appear, peak,and resolve at different times. Combination products areconvenient, but the convenience must be weighed against6. Open the container carefully. Position the dropper tipthe risks from taking unnecessary drugs. Patient educationnear, but not inside, the ear canal opening. Do not allowregardingthe administration11-2) andthe dropperto touch the ofear,intranasalbecause it(Tablecould becomeocular contaminated(see Chapteror28)drugsimportant.injuretheisear.Eardrops must be keptNotall patients should self-treat colds (refer to theclean.exclusionsfor self-treatmentlistedear)in Figure11-1).Patients7. Pull yourear (or the patient’sbackwardand upwardto open the earischemiccanal as showndrawingcoronaryA. If the patientwith hypertension,heart indisease,arteryis ahyperthyroidism,child younger than 3diabetesyears old, pullthe ear increasedbackwarddisease,mellitus,and downwardin ertrophyshould use8. Place the proper dose or number of drops into the eardecongestantsonly after consulting a primary care provider.canal. Replace the cap on the container.9. Gently press the small, flat skin flap (tragus) over the earNonpharmacologiccanal opening toTherapyforce out air bubbles and push the dropsdown the ear canal.Nondrugtherapy includes increased fluid intake, adequate10. Stay (or keep the patient) in the same position for therest, a lengthnutritiousdietas tolerated,increasedhumidificaof timeindicatedin the productinstructions.If thetion withcoolsalinepatientis amistchildvaporizerswho cannotorstaysteamystill, theshowers,doctor maytellgargle,youandto nasalnasalspraysorchild’sdropsplace airrigation.clean piece Salineof cottongentlyinto theto preventthe medicationfromdrainingUse crustedlargeinexpensiveenough to removedo withnot leaveitmucus.pieceSimple,foodseasily,such andas tealemonintheearlongerthananhour.and honey, chicken soup, and hot broths are soothing and11. Repeat the procedure for the other ear, if needed.increasefluid intake. Limited evidence suggests that12. Gently wipe excess medication off the outside of theear,chickensoupcould have anti-inflammatory activity.11 Milkusing caution to avoid getting moisture in the ear canal.productsshouldnot be withheld as there is no evidence13. Washyour hands.that milk increases cough or congestion. Medical devices,such as Vicks Breathe Right nasal strips, are marketed forSource: ffromnasalMedicationcongestionand stuffinesslem Solving in Ambulatory Care. Washington, DC: Americanresultingfrom colds and allergies. These devices lift thePharmaceutical Association; 1994:9.nares open, enlarging the anterior nasal passages; mentholated strips produce a soothing odor, which may easeCarbamidePeroxidenasalirritation.Nondrug peroxidetherapy for6.5%infantsuprightposi-isCarbamidein nage,maintaininganapproved as safe and effective in softening, loosening,adeandquatefluid eearwax inand ofininspiredchildrenair,12andirrigatingthe14 nosewith salinedrops.Also, sincechilyearsand older.(See Table30-1 forthe properinstillationdrentypically cannotblowperoxidetheir ownnoses untilabout4of eardrops.)Carbamideis preparedfromhydroyears of age, carefully clearing the nasal passageways withgen peroxide and urea. When carbamide peroxide isa bulb syringe may be necessary if accumulation of mucusexposed to moisture, nascent oxygen is released slowly andinterferes with sleeping or eating.203AdministrationTABLEGuidelines for GuidelinesRemoving Excessive/TABLE11-230-2Guidelines foradministeringforNasalDrugsImpacted Cerumen nasal drugsNasalSprays1. Place5 to 10 drops of the cerumen-softening solution intothe ear canal, and allow it to remain for at least 15 minutes(see Table 30-1).nostril as shown in drawing A.2. Prepare a warm (not hot) solution of plain water or other Keep head upright. Sniff deeply whilesolution as directed by your doctor. Eight ounces of solusqueezing the bottle. Repeat with othertion should be sufficient to clean out the ear canal.nostril.3. To catch the returning solution, hold acontainer under the ear being cleaned.An emesis basin is ideal because it fitsthe contour of the neck. Tilt the headdown slightly on the side where the earis being cleaned.4. Gently pull the earlobe down and backto expose the ear canal as shown inPumpdrawingNasal SpraysA.5.Placetheopenbeforeend ofusingthe syringeinto the ear canal withthe first Prime the pumptheHoldtip pointedslightlytoward the side of the eartime.the bottlewithupwardthe nozzlecanal, asin thedrawing.Do not aim the syringebetweentheshownfirst twofingersand thumbbackofofthethebottle.ear canal. Make sure the syringe doeson intothe thebottomthe outflow of solution. Tiltnottheobstructhead forward.6. Squeezethebulbgently—notintroduce the Gentlyinsertthenozzletip avoidrupturingthe earnostril as shown in drawing B. Sniffdrum.(Note:Only healthdeeplywhiledepressingthe professionalspump once. trained in auralhygieneuse forced water sprays [e.g., Water Pik]withshouldother nostril. Repeatto remove cerumen.)7. Do not let the returning solution come into contact withthe eyes.8.Ifpain or dizziness occurs, remove the syringe and do notNasal Inhalersresume irrigation until a doctor is consulted.thesureinhalerin handjust before Warm9. Makeall wateris drainedfromuse.the ear to avoid preinserttotheinhaler fromtip intoone hownin drawingC. Sniff10.Rinseasthesyringethoroughlybefore and after each use,deeplywhileinhaling.and letit dry. 11.Repeatother nostril.Storewiththe syringein a cool, dry place (preferably, in its Wipethe inhalerafterawayeachfromuse. hotMakeoriginalcontainer)surfaces and sharpsurethe cap is tightly in place betweeninstruments.uses.after 2-3twicemonthsevenif the12.DoDiscardthis proceduredailyfor nolonger than 4 consecinhalersmells medicinal.utive stilldays. Gently insert the bottle tip into oneSource: Adapted with permission from Ohio Clinician. 1996;14(5):10.NasalDropsthe bulb to Squeezeactsas a weakantibacterial. The effervescence that occurswithdraw medicationduringthisprocess,from the bottle. along with urea’s effect on tissue debridement,helpstoheadmechanically break down and loosen Lie on bedwithtilted backcerumenthatoverhasthebeen softened by anhydrous glycerin.sideof thebed as remaining after treatment may beAnycerumenshown in drawing D.removedwith gentle, warm-water irrigation using a rubber Place theoticrecommendedbulb syringenumber(Tableof30-2).Improperuse Gentlyof antiltoticdrops intoone rumenhead from side to side.othernostril. Lieon bedfor ora coupleof minutes Repeatcanleave withexcessmoisturein thecanalfurthercompressafter placingdropsin thecannose.cerumen.Theseactionsalso cause otitis externa, per Do not rinse the dropper.forated tympanic membrane, pain, vertigo, otitis media,tinnitushissing,or buzzingnoises inthe ear),Note: Do(ringing,not share thedrug withanyone. Discardsolutionsif12,15,16andcough.ordiscoloredif contamination is suspected. Remove capsCarbamideperoxideis nonirritatingand maybeforeuse and replaceaftersolutionuse. Do notuse expired ose.be used twice daily for up to 4 days. If symptomsGentlypersistdepress the other side of the nose with finger to close off theafter4 days, the patient should see a primary care providernostril not receivingthe medication. Wait a few minutes after17forevaluation.usingthe drug before blowing the nose.Ensuring Quality Care Chapter 11 Medication Administration6369
recommended solution, and the presence of a preservative. As the number of drops per day increases, toxicityfrom preservatives becomes more likely.12Although PVA is compatible with many commonlyandDisorderspreservatives, certain compounds (includI Ophthalmic, usedOtic,drugsand Oraling sodium bicarbonate, sodium borate, and the sulfatesof sodium, potassium, and zinc) can thicken or gel solutions. For example, sodium borate is found in somelike, environAdministrationGuidelinesand may reactTABLE 28-2extraocularirrigatingsolutions or irrigants,ntact with the13 Thus,with contactlens eringeye PVA.dropsforDropsSystane is saidit is important to be cautious when using solutions thatthelial repair1. If youhave difficulty telling whether eye drops touch thecontainPVA.symptoms.eye surface, refrigerate the solution before instilling it. Doartificial tearsnot entshe ocular sur2. Wash hands thoroughly. Wash areas of the face around thectitioners and The primaryeyes. Contactlenses shouldbe removednonprescriptionunless the prodingredientsin commercialuct is designedspecificallyfor usearewithwhitecontactlenses.eserved prod- ophthalmicointments(Table 28-1)petrolatum3. Tilt headback.ialized storage (a lubricantandointment base), mineral oil (which helpsGently grasplowerbelow lashes,andlanolinpullopened.the 4.ointmentmeltat outerbody eyelidtemperature),andeyelid away from eye to create a pouch.(which facilitates incorporation of water-soluble medica5. Place dropper over eye by lookingalso prevents evaporation).Most patients tions anddirectly at it as shown in the drawing.artificial tears6. Just before applying a single drop,the morning Mechanismof Action/Indications The principal advanlook up.commending tage7.ofAsnonmedicated(bland)ointments is their enhancedsoon as the dropis applied,releasetheineyelidslowly.Closeappears to enhance theng point. The retentiontimethe eye,whicheyesfor 3film.minutesby placingcan then be integrityofgentlythe tearThus,both mucin- and aqueousyoureyesheaddownasthoughr more severe deficientcan benefit fromlookingthe application of lubricatat the floor (using gravity to pull theto four times ing ointments.drop onto the cornea). Minimize blinking or squeezingnse to therapythe eyelid.may be given DosageAdministrationGuidelinesOintment8. Useanda fingerto put gentle pressureover the openingofor those with the tear duct.m perborate; 28-3).However,dependingon thepatient’sclinical needs9. Blotexcessivesolution fromaroundthe eye.d in patients10. If multiple drop therapy is indicated, wait at least 5 minutesants requiresiscosity of theof a preservaeases, toxicityny commonlyunds (includd the sulfatesn or gel soluund in someand may reactg PVA.13 Thus,solutions thatnprescriptione petrolatum(which helpsand lanolinuble medica-ncipal advanheir enhancedenhance theand aqueouson of lubricat-Ointment10e daily (Tableclinical needsbefore instilling the next drop. This pause helps ensurethat the first drop is not flushed away by the second, orthat the second drop is not diluted by the first.11. If using a suspension, place that drop in last.12. If both drop and ointment therapy are indicated, instill thedrops at least 10 minutes before the ointment so the ointment does not become a barrier to the drops’ penetratingthe tear film or cornea.TABLE 28-3Administration Guidelinesfor Eye Ointments1. Wash hands thoroughly. Wash areas of the face around theeyes.2. If both drop and ointment therapy are indicated, instill thedrops at least 10 minutes before the ointment so that theointment does not become a barrier to the drops’ penetrating the tear film or cornea.3. Tilt head back.4. Gently grasp lower outer eyelidbelow lashes, and pull eyelid awayfrom eye as shown in the drawing.5. Place ointment tube over eye bylooking directly at it.6. With a sweeping motion, place 1/4to 1/2 in. of ointment inside thelower eyelid by gently squeezing thetube, but avoid touching the tube tipto any tissue surface.7. Release the eyelid slowly.8. Close eyes gently for 1 to 2 minutes.9. Blot excessive ointment from around the eye.10. Vision may be temporarily blurred. Avoid activities requiring good visual ability until vision clears.drops at least 10 minutes before the ointment so the ointment does not become a barrier to the drops’ penetratingthe tear film or cornea.TABLE 28-3Administration GuidelinesGuidelines forforadministeringEye Ointments eye ointments1. Wash hands thoroughly. Wash areas of the face around theeyes.2. If both drop and ointment therapy are indicated, instill thedrops at least 10 minutes before the ointment so that theointment does not become a barrier to the drops’ penetrating the tear film or cornea.3. Tilt head back.4. Gently grasp lower outer eyelidbelow lashes, and pull eyelid awayfrom eye as shown in the drawing.5. Place ointment tube over eye bylooking directly at it.6. With a sweeping motion, place 1/4to 1/2 in. of ointment inside thelower eyelid by gently squeezing thetube, but avoid touching the tube tipto any tissue surface.7. Release the eyelid slowly.8. Close eyes gently for 1 to 2 minutes.9. Blot excessive ointment from around the eye.10. Vision may be temporarily blurred. Avoid activities requiring good visual ability until vision clears.
254TABLE 13-7Section IV Respiratory DisordersGuidelines for Using MDIsGuidelines for using MDIsClosed-mouth Technique1. Remove dust cap from inhaler. Attach inhaler to spacer/holding chamber if you have one. Shake the inhaler well as shown indrawing A.2. Blow out all the air in your lungs (see drawing B).3. Seal lips tightly around the mouthpiece. As you breathe in slowly, press down on the inhaler to release the medicine until yourlungs are full (see drawing C).4. Hold your breath for 10 seconds to allow the medicine to reach deeply into your lungs (see drawing D).5. Blow out the air in your lungs (see drawing E).Open-mouth TechniqueTABLE 13-8Alternative Agents That May Worsen Asthma Symptoms or Cause Significant Harm24AgentRiskCoffee, black teaIncreased risk of hospitalization for acute asthmaCinnamon, canela (tea), essential oil (fromthe bark)Can be neurotoxic if ingestedEucalyptusEssential oil can be toxic if ingested, causing respiratory distress and neurologicsymptomsOregano teaMay contain inhalant allergensCayenne, chile (active ingredient iscapsaicin)Single use may aggravate acute asthma episodes; bronchoconstriction possible ifpowder is inhaledEnsuring Quality Care Chapter 11 Medication Administration1. Take off the cap. Shake the inhaler as shown in drawing F.2. Stand up and tilt your head back a little (see drawing G).3. Place your hand between your mouth and the inhaler as shown in drawing H to measure how far away the inhaler should befrom your mouth.4. Take a cleansing breath; in and out.5. Open your mouth wide; start to breathe in slowly; push down on the inhaler; while continuing to breathe in (see drawing I).6. Hold your breath; count to 10; then breathe out.7. If your asthma care plan instructs you to use 2 puffs, wait 1 minute and repeat steps 1-6.11
318TABLE 16-6Section V Gastrointestinal DisordersAdministration of Rectal Suppositories or EnemasAdministration of rectal suppositories or enemasEnemasSuppositories1. If someone else is administering the enema, lie on yourleft side with knees bent or in the knee-to-chest position(see drawings A and B). Position A is preferred for children older than 2 years. If self-administering the enema,lie on your back with your knees bent and buttocksraised (see drawing C). A pillow may be placed underthe buttocks.2. If using a concentrated enema solution, dilute solutionaccording to the product instructions. Prepare 1 pint(500 mL) for adults and 1/2 pint (250 mL) for children.3. Lubricate the enema tip with petroleum jelly or othernonmedicated ointment/cream. Apply the lubricant tothe anal area as well.4. Gently insert the enema tip 2 (recommended depth forchildren) to 3 in. into the rectum.5. Allow the solution to flow into the rectum slowly. If youexperience discomfort, the flow is probably too fast.6. Retain the enema solution until definite lower abdominal cramping is felt. The parent/caregiver may have togently hold a child’s buttocks closed to prevent the solution from being expelled too soon.is probably too fast. One pint (500 mL) or less of properlyintroduced fluid usually produces adequate evacuation if itis retained until definite lower abdominal cramping is felt.As long as 1 hour may be needed for the entire procedure.DRUG INTERACTIONS1. Gently squeeze the suppository to determine if it is firm enoughto insert. Chill a soft suppository by placing it in the refrigeratorfor a few minutes or by running it under cool running water.2. Remove the suppository from its wrapping.3. Dip the suppository for a few seconds in lukewarm water tosoften the exterior.4. Lie on your left side with knees bent or in the knee-to-chestposition (see drawings A and B). Position A is best for self-administration of a suppository. Small children can be held in a crawlingposition.5. Relax the buttock just before inserting the suppository to easeinsertion. Gently insert the tapered end of the suppository highinto the rectum. If the suppository slips out, it was not insertedpast the anal sphincter (the muscle that keeps the rectum closed).6. Continue to lie down for a few minutes and hold the buttockstogether to allow the suppository to dissolve in the rectum. Theparent/caregiver may have to gently hold a child’s buttocksclosed.7. Remember that the medication is most effective when the bowelis empty. Try to avoid a bowel movement after insertion of thesuppository for up to 1 hour so that the intended action can occur.may also be improved by drinking the product with a citrusfruit juice or with a citrus-flavored carbonated beverage.Complementary TherapiesA drug interaction occurs when a drug interactswith other drugs and/or certainPatients frequently treat constipation with a botanicalSuppositories Bisacodyl-containing suppositories are(Table16-7; see also Chapter53).20,32,45-48Althoughproductfoods toas producesideKnowledgeofdruginteractions,as wellas adversepromotedreplacementsfor effects.enemas whenthe distalmany of the commercially available stimulant and bulkcolonrequires forcleaning.that containforming laxativesderivedfrom plants,some n bisaby a residentcan arehelppreventproblems.12codyl are used for postoperative, antepartum, and postparprefer to use a “more natural” version of these products.tum care, and are adequate in preparing for proctosigmoidConsumers should be cautioned that FDA does not reguOne medicationmaysuppositoriesinteract arewithanother lateby increasing,or alteringoscopy.Although bisacodylprescribedthese products decreasingand the manufacturersare notrequired to provide information on how to use the prodand
4 » Common problems caused by OTC medications: They may change the effect of prescribed medications, for example, making them stronger or less effective.