Transcription
Reducing Underage and YoungAdult DrinkingHow to Address Critical Drinking ProblemsDuring This Developmental PeriodMichael Windle, Ph.D., and Robert A. Zucker, Ph.D.Forty years ago, when the National Institute on Alcohol Abuse and Alcoholism (NIAAA) was founded,alcoholism was considered an adult disease driven principally by physiological determinants. AsNIAAA expanded its research portfolio, new data and insights were obtained that led to an increasedfocus on underage and young adult drinking. Fostered by interdisciplinary research, etiologic modelswere developed that recognized the multiplicity of relevant genetic and environmental influences.This shift in conceptualizing alcohol use disorders also was based on findings from large-scale,national studies indicating that late adolescence and early young adulthood were peak periods for thedevelopment of alcohol dependence and that early initiation of alcohol use (i.e., before age 15) wasassociated with a fourfold increase in the probability of subsequently developing alcohol dependence.In recent years, developmental studies and models of the initiation, escalation, and adverseconsequences of underage and early young adult drinking have helped us to understand how alcoholuse may influence, and be influenced by, developmental transitions or turning points. Major risk andprotective factors are being identified and integrated into screening, prevention, and treatmentprograms to optimize interventions designed to reduce drinking problems among adolescents andyoung adults. In addition, regulatory policies, such as the minimum drinking age and zero-tolerancelaws, are being implemented and evaluated for their impact on public health. KEY WORDS: Underagedrinking; drinking in young adulthood; psychosocial development; development of alcohol disorders; risk factors;protective factors; alcohol effects on brain development; screening among youth; preventive interventions; collegedrinking; treatment for adolescents and young adultsIn 1970, the National Institutesof Health (NIH) established theNational Institute on Alcohol Abuseand Alcoholism (NIAAA). At that time,both the general public and the scientificcommunity predominantly regardedalcoholism as a disorder of adulthood,and the major focus of NIH-fundedscientific work was on understandingits etiology and finding new treatmentsfor it. Most of the etiological researchfocused on physiological and clinicalanalyses in adults, and the drinkingbehavior of adolescents only appearedin discussions of the epidemiology andsociology of drinking patterns (e.g.,Kissin and Begleiter 1972, 1976;Popham 1970).Vol. 33, Nos. 1 and 2, 2010Simultaneously, but unrelated tothe research on the adult psychopathology, a separate scientific communitywas sensitized to the public concernabout an illegal activity—underagedrinking—that potentially couldresult in great personal and societalcost in the form of accidents and lossof life. By the late 1970s, a significantbody of research was addressing thecritical issue of why most youth onlybegin drinking in mid- to late adolescence and consume alcohol in smallamounts at infrequent intervals andwithout problems, whereas othersbegin much earlier, and in some casesprogress to consuming near-alcoholiclevels within a short time after initia-tion. At that time, NIAAA’s Divisionof Epidemiology and Preventionincreasingly began to support researchaddressing these issues, and an impor tant body of theory and researchbegan to articulate the developmentalnature of drinking behavior and toMICHAEL WINDLE, PH.D., is a professorin, and chair of, the Department ofBehavioral Sciences and Health Education,Emory University, Atlanta, Georgia.ROBERT A. ZUCKER, PH.D., is a professorin the Departments of Psychiatry andPsychology and director of the AddictionResearch Center, University of Michigan,Ann Arbor, Michigan.29
identify individual and social contex tual factors that regulate it (Blane andChafetz 1979; Jessor and Jessor 1977;Kandel 1978). This research also start ed to investigate how the initiation ofdrinking could be delayed and how theoccurrence of problems could be reducedonce drinking had begun (Kandel1989; Robins and Przybeck 1985).As the developmental window fromchildhood to early adulthood hasbeen studied over the years, researchon early drinking origins to adoles cent problems on the one hand andon the origins of alcoholism on theother hand has begun to converge.An NIAAA news release in 2004 (Li2004) articulates this integration,stating that both alcohol-relatedproblems and alcohol use disorders(AUDs) needed to be understooddevelopmentally because they origi nate before adulthood; moreover, thehighest prevalence of alcohol depen dence occurs in youth ages 18–20(Grant et al. 2004). Since then, researchon underage drinking has increasinglycrossed disciplines and now involvesintegrative work on the genetics andneurophysiology of risk that is beingtied to behavioral and social environ mental science (Clark et al. 2008;Kendler and Prescott 2006; McGueet al. 2001).Two initiatives in the past decadeunderscore NIAAA’s recognition ofthe importance of underage and earlyadult drinking as a problem area ofnational significance and also haveled directly to the work summarizedin this article. One initiative, kickedoff in 1998, was the Task Force onCollege Drinking (NIAAA 2002;also see the article by Hingson, pp.45–54), which was charged withreviewing the existing research on col lege drinking as a basis for implement ing and evaluating alcohol preventionprograms. The other is the UnderageDrinking Research Initiative (NationalAcademy of Sciences 2004; also seesidebar), which was formed in 2004to intensify research, evaluation, andoutreach efforts on the underage drink ing problem. This initiative is ongoingand has led to the development ofthe committee on Assessment andScreening for Underage Drinking Risk.This article provides a brief snapshotof the current scientific knowledgeabout these earliest drinking years. Itsummarizes the epidemiologic evidencethat documents the importance of theNIAAA’s Underage Drinking Research InitiativeThe National Instituteon Alcohol Abuse andAlcoholism’s (NIAAA’s)Underage Drinking Research Initiativewas undertaken in response to theconvergence of recent scientificadvances and the increased publicconcern about the seriousness ofunderage drinking and its personaland societal costs. These concernswere expressed cogently both in the2007 Surgeon General’s Call to ActionTo Prevent and Reduce UnderageDrinking (U.S. Department ofHealth and Human Services 2007)and by the 2004 report ReducingUnderage Drinking: A CollectiveResponsibility (Bonnie and O’Connell2004), which was sponsored by theNational Research Council and theInstitute of Medicine. The focus ofthis NIAAA initiative is to intensifyresearch, evaluation, and outreachefforts regarding underage drinking.To accomplish this, NIAAA formedan interdisciplinary working groupon underage drinking that consistedof NIAAA staff members and amultidisciplinary steering commit 30tee. The mission of the steeringcommittee is to stimulate researchon underage drinking by drawingupon multiple disciplines (e.g., ado lescent development, genetics, neu roscience, prevention, and socialpolicy) to advise NIAAA on futureresearch to improve the preventionand treatment of underage drinking.Thus far, goals identified by thesteering committee have yieldednumerous products, including twospecial issues in scientific journals(i.e., the April 2008 issue of Pediatrics[Suppl. 4] and a 2009 issue ofAlcohol Research & Health [Vol. 32])that summarized existing researchand identified important gaps.NIAAA also has established a Website for the Underage DrinkingInitiative dPrograms/underage.htm) thatcontains updated statistics onunderage drinking; updates fromthe Steering Committee; print pub lications for parents, teachers, andyoung people, such as “Keep KidsAlcohol Free: Strategies for Action;”multimedia resources; and otherNIAAA-sponsored sites relevant tounderage drinking. Other NIAAAsponsored sites include The CoolSpot (http://www.thecoolspot.gov),an interactive site designed foryoung people that features FAQs,statistics, and other informationabout underage drinking, and TheLeadership to Keep Children AlcoholFree (http://www.alcoholfreechildren.org), a unique coalition ofGovernors’ spouses, Federal agencies,and public and private organizationswhose focus is on preventing the useof alcohol by children. ReferencesBONNIE, R.J., AND O’CONNELL, M.E., EDS.Reducing Underage Drinking: A CollectiveResponsibility. Washington, DC: NationalAcademies Press, 2004.U.S. Department of Health and HumanServices. The Surgeon General’s Call to ActionTo Prevent and Reduce Underage Drinking.Rockville, MD: U.S. Department of Healthand Human Services, Office of the SurgeonGeneral, 2007.Alcohol Research & Health
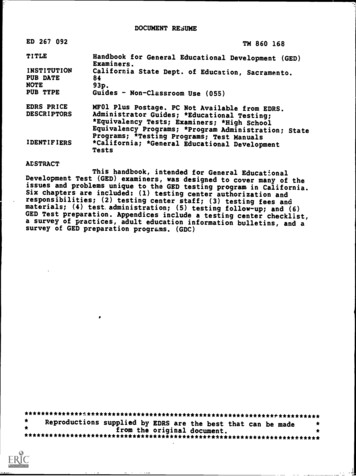
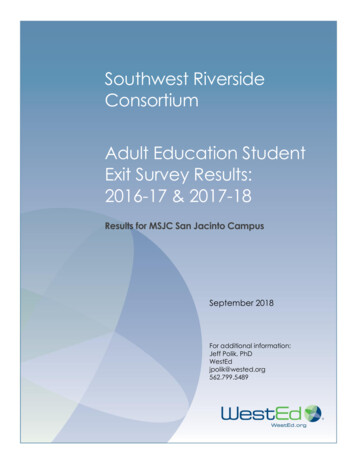
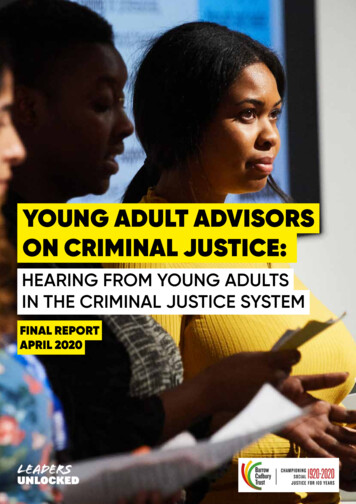
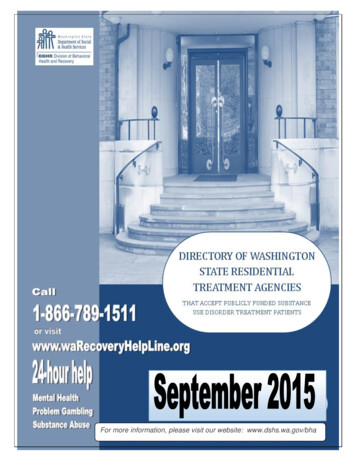
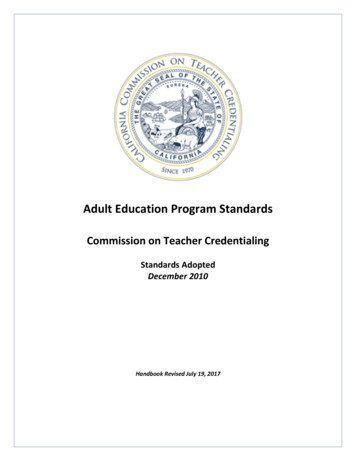
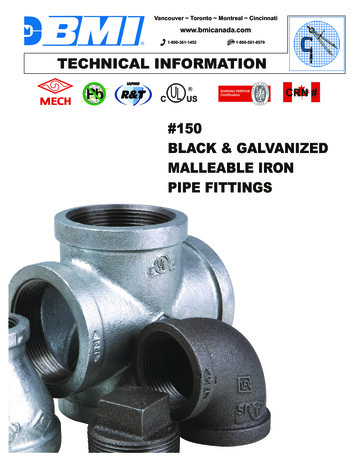
Reducing Underage and Young Adult Drinkingadolescent and young adult periods indetermining level of alcohol con sumption. The article then examinesthe developmental nature of problemuse, explores why the developmentalchanges of this age period are of par ticular importance from a publichealth standpoint, describes the criticalnature of timing in the onset of drink ing behavior, and explains the man ner in which the changes in drinkingthat occur between age 10 and theearly 20s map onto other develop mental challenges of this period of life.Finally, the article briefly reviewscurrent knowledge about the risk andprotective factors that exist duringadolescence and young adulthood andsummarizes the screening, prevention,and intervention programs focusedon this age-group. Note that althoughthe specific age ranges referenced indifferent places in this article may varyto some extent contingent on the citedstudies, there is consistent agreementregarding the problematic nature ofunderage and young adult drinking.Epidemiology of Underageand Young Adult DrinkingNational, large-scale surveys conductedover the past 20 years have providednew insights into the prevalence ofalcohol consumption, binge drinking,and AUDs, which have altered the man ner in which alcohol use and AUDs areviewed by professionals and lay peoplealike. For example, data from theNIAAA-funded National EpidemiologicSurvey on Alcohol and RelatedConditions (NESARC) (Grant et al.2004) have indicated that the preva lence of past-year alcohol dependence ishighest in late adolescence (ages 18–20)and early young adulthood (ages 21–24),with rates declining thereafter (seefigure 1). Similar findings have beenreported in other national surveys, suchas the National Survey of Drug Useand Health (NSDUH), which foundthat the highest prevalence of lifetimeAUDs was reported in late adolescenceand early young adulthood (SubstanceAbuse and Mental Health ServicesAdministration [SAMHSA] 2003, 2004,2006). For instance, according to theNSDUH, for a variety of population sub groups (i.e., both male and female as wellas for White, Black, and Hispanic sub jects) the highest rate of AUDs was foundin people ages 18–25 years.Another way to examine the associ ation between age and AUDs is toevaluate the age at onset of alcoholdependence. This variable is impor-Figure 1 Prevalence of past-year DSM–IV alcohol dependence in the United States.SOURCE: 18 years: 2001–2002 National Epidemiologic Survey on Alcohol and Related Conditions,12–17 years: National Survey on Drug Use and Health 2003.Vol. 33, Nos. 1 and 2, 2010tant because an earlier age at onsethas been associated with a moresevere course of alcoholism, poorertreatment response, and higher relapserates (Windle and Scheidt 2004).NESARC determined the age at onsetof alcohol dependence for a nationalsample of over 43,000 adults (see fig ure 2). The findings indicated thatonset of first-time alcohol dependenceoccurred most commonly in late ado lescence to early young adulthood,subsequently declining with age.Yet another variable relevant to theassociation between age, alcohol use,and alcohol dependence is the age offirst use of alcohol and its relation ship to an important risk factor (i.e.,family history of alcoholism). Grantand Dawson (1997) reported thatamong people who developed alcoholdependence, having a family historyof alcoholism (i.e., an alcoholic par ent) was significantly associated withan earlier age of first use of alcohol(also see figure 3). For example, amongpeople with alcohol dependence whowere family-history positive, almost60 percent initiated drinking at age13. By contrast, among people whodeveloped alcohol dependence andwere family-history negative, onlyabout 28 percent initiated drinkingat age 13. This finding demonstratesthat a family history of alcoholism isassociated with an earlier age of firstuse of alcohol, which for many peo ple ultimately evolves into alcoholdependence in later adolescence oryoung adulthood.The prevalence of AUDs is a valuableindicator of serious alcohol problemsduring late adolescence and earlyyoung adulthood. Another importantparameter is the frequency of alcoholconsumption and binge drinkingamong underage drinkers and youngadults. In the United States, alcoholconsumption occurs in the majorityof adolescents (i.e., is statisticallynormative). According to the 2008Monitoring the Future Survey (MFS)(Johnston et al. 2009), almost 72percent of high-school seniors report ed consuming alcohol during theirlifetime. Moreover, 43 percent hadconsumed alcohol in the past 3031
For the three alcohol use indicators(i.e., drinking in the past 30 days,being drunk in the past 30 days,and binge drinking in the past 2weeks), prevalence increased sub stantially as teens moved from earlyto middle and later adolescence. Whereas younger male and femaleadolescents were similar in their useof alcohol, older male adolescentswere somewhat more likely to becurrent drinkers and to use alcoholin heavier amounts than were femaleadolescents in the same grades.Percentage In Each Age Group Who DevelopFirst-time Alcohol Dependencedays, 28 percent reported being drunkin the past 30 days, and 25 percent hadbeen binge drinking1 in the past 2 weeks(see the table). The survey findingsallow several conclusions regardingpatterns of alcohol use among mid dle- and high-school students.AgeFigure 2 Age at onset of DSM–IV alcohol dependence. Data were derived from the 2003 NationalEpidemiologic Survey on Alcohol and Related Conditions (NESARC).SOURCE: NIAAA National Epidemiologic Survey on Alcohol and Related Conditions 2003. Across grades, Black adolescentsreported lower levels of current andheavy alcohol use than did Whiteand Hispanic teens. At younger ages,Hispanic teens were slightly morelikely to use alcohol than Whiteteens, but by 12th grade, this rela tionship had been reversed. This lat ter finding may be attributable, inpart, to higher school dropout ratesamong Hispanics compared withWhites and Blacks. That is, Hispanicteens who drink at higher rates maybe more likely to drop out of schooland therefore are not includedamong seniors in these school-basedepidemiologic studies.Although absolute prevalencerates may differ somewhat, these pat terns of alcohol use in terms of age,gender, and race/ethnic group differ ences obtained in the MFS are con sistent with those found in othersurveys, including the Centers forDisease Control and Prevention(CDC)-funded Youth Risk BehaviorSurveillance Survey and the NSDUH(CDC 2005; Johnston et al. 2009;SAMHSA 2003, 2004, 2006).Figure 3 Association between age at initiation of alcohol use and lifetime dependence (i.e., meetingthe DSM–IV criteria for dependence at some point in life). The blue curve represents allrespondents, the red curve represents respondents with a family history of alcoholism,and the black curve represents respondents without a family history of alcoholism.SOURCE: 2001–2002 National Epidemiologic Survey on Alcohol and Related Conditions.1Binge drinking was defined as having five or more drinks in a row.32Alcohol Research & Health
Reducing Underage and Young Adult DrinkingResearch studies based on nationalsurvey data from both adolescentsand adults have indicated that heavieralcohol use distinguishes late adolescentsand early young adults from adults.For example, for male and female sub jects, binge drinking increased duringadolescence, peaked between ages 18and 25 years, and declined thereafter(see figure 4). Similarly, the MFSindicated that the prevalence of “havingbeen drunk” in the past year increasedsubstantially from 8th grade (12.7percent) to 12th grade (45.6 percent)and to young adulthood (66.0 percent).Another measure of drinking patternsduring different portions of the life span is the number of drinking daysper month and the usual number ofdrinks per drinking occasion (see figure5). Survey data indicate an orderingby age-group of these variables—thatis, underage drinkers had the fewestnumber of drinking days per monthbut drank the most on the days thatthey did drink; young adults followedthe underage group with fewer drinkingdays and more drinks per occasionthan adults. Thus, compared withadults, underage drinkers and youngadults drink on fewer occasions butconsume more per occasion. Thisdrinking pattern may be more haz ardous to the drinker’s social function ing and physical and mental health.In summary, extant epidemiologicdata indicate that the prevalence ofalcohol use begins in early adoles cence, steadily increases throughoutthe high school years, reaches a peakin the mid-20s, and begins to declinethereafter. The findings are consistentacross different indicators of drinking(e.g., alcohol use, drinking to intoxica tion, and binge drinking) and acrosssex and racial/ethnic groups. Theseage trends also are evident for AUDs,which peak in late adolescence andearly young adulthood.The Developmental Natureof Underage and YoungAdult DrinkingThe prevalence data on alcohol use andAUDs clearly illustrate that adolescenceand early young adulthood are criticalfor understanding the occurrence ofthese conditions. In and of themselves,these findings do not necessarily indicatethat alcoholism is a developmentaldisorder. However, data on age of initi ation of alcohol use and its relationshipto the subsequent development ofalcohol dependence provides a strongindication of the developmental natureof AUDs. Grant and Dawson (1997)reported that people who began drink ing before age 15 were four times morelikely to subsequently become alcoholdependent than people who did notdrink alcohol before age 21. Furthermore,the odds of subsequently developingalcohol dependence were reduced by14 percent with each increasing year ofage at first use. This latter finding isthe source of intervention programstargeted at delaying the age of initia tion of alcohol use.The significance of earlier initiationas a risk factor for AUDs, in conjunc tion with other data based on longi tudinal studies, has fostered the notionof the developmental nature ofunderage and young adult drinking,which has been confirmed by otherfindings. For example, Greenfieldand Rogers (1999) reported thatadolescents to young adults ages18–29 were disproportionately repre sented among the heaviest drinkers.Thus, although this age-group repre sented only 27 percent of the U.S.population, they accounted for about45 percent of overall adult drinking.In an analysis of the commercial valueof underage drinking, Foster andcolleagues (2006) determined thatin 2001, the short-term cash valueto the alcohol industry from under age drinkers was 22.5 billion dollars,representing 17.5 percent of totalconsumer expenditures for alcoholbeverages.In a separate study using differentdata sources, Miller and colleagues(2006) estimated that in 2001, under age drinkers accounted for 16.2percent of all alcohol sales in the UnitedStates. However, the economic costsattributable to alcohol-related youthproblems, such as drinking and driving,interpersonal violence, propertyTable Prevalence (%) of Various Indicators of Alcohol Consumption by Race/Ethnicity, Gender, and School Grade, in 2008.DemographicVariablesSchool leFemaleAlcohol Use in thePast 30 DaysPercentage of Students ReportingHaving Been Drunkin Past 30 DaysHaving Had Five orMore Drinks in aRow in Past 2 629.226.28.18.18.016.016.615.424.628.421.3SOURCE: National Institute on Drug Abuse and University of Michigan, Monitoring the Future Surveys (Johnston et al. 2009).Vol. 33, Nos. 1 and 2, 201033
crimes, and suicide, totaled 61.9 bil lion (in 2001 dollars). These costsincluded medical care costs, lost workand other monetary costs, and quality of-life costs. Hence, underage andyoung-adult populations clearly areheavy consumers of alcoholic beveragesand result in economic costs that arenearly three times higher than theprofits of the alcohol industry.From a public health perspective,it also is important to highlight that thethree major causes of death among12- to 20-year-olds in the UnitedStates—unintentional injuries (withmotor vehicle crashes accounting forthe majority of deaths), homicides,and suicides (Subramanian 2006)—all are associated with alcohol use,especially heavy use. For example, in2003, motor vehicle crashes were theleading cause of death among 12- to20-year-olds. In that same year, a reportby the National Highway TrafficSafety Administration (Pickrell 2006)indicated that among drivers ages 20years or younger who were involvedin fatal traffic crashes, approximately20 percent had consumed alcohol atthe time of the crash. In addition, themedian blood alcohol concentration(BAC) for this age-group ranged from0.12 to 0.14 percent, well above thelegal limit of intoxication (i.e., 0.08percent) of intoxication.Finally, higher levels of alcohol useare associated not only with increasedmortality but also with a broad rangeof other problem behaviors, includingcigarette and other drug use, deviantbehavior, earlier sexual activity andincreased risk for sexually transmittedinfections (including infection withthe human immunodeficiency virus[HIV]), as well as truancy, academicdifficulties, and school drop out. Theseconsequences of heavy alcohol useamong teenagers and young adultsaffect not only the drinker but alsomay adversely impact others via alcoholrelated injuries and violence (e.g.,victims of adolescent or young adultalcohol-related crashes, campus disrup tions, or enhanced aggressive tendencies).Clearly, the morbidities, mortality,and collateral damage associatedwith underage and early young adult34drinking represent a pervasive publichealth problem involving the entirepopulation in this age-group. Therefore,appropriate responses also should betargeted at the entire adolescent andyoung adult population rather thanbe restricted only to those who meetclinical diagnostic criteria for an AUD.Developmental Frameworkfor UnderstandingUnderage and YoungAdult DrinkingAs the findings provided in the previoussections show, drinking behavior anddrinking problems change across ado lescence and young adulthood, with aclear pattern of age-graded variation. Toconsider these changes as “maturation”—that is, as a process of emergence andlinear growth of alcohol use and alcoholproblems—is insufficient becausedrinking levels across this developmentalperiod vary considerably among indi viduals. These differences in course havebeen demonstrated vividly by Schulenbergand colleagues (1996) in their trajectoryanalysis of a nationally representativesample they had followed through ages18–22 years. The analysis found thatthe pattern of binge drinking based onthe means of the total sample over theinterval does not reflect the pattern forany subset of individuals (see figure 6)but is a composite of five starkly differ ent trajectory courses: A chronic trajectory of continuouslyhigh frequency of binge drinking; A trajectory with decreasing fre quency of binge drinking over time; A trajectory with increasing fre quency of binge drinking over time; A “fling” trajectory with a transientincrease in binge drinking frequency;and A trajectory of continuously lowfrequency of binge drinking.More recent trajectory studies ofthis age-group continue to supportthe validity of these trajectory patterns,although class membership percent ages vary somewhat as a function ofsample age, number of waves of dataavailable, and trajectory class analyticmethod (Brown et al. 2008; Windleet al. 2005). It is important to note,however, that this variability is occur ring during a developmental periodFigure 4 Number of days in the past 30 days on which drinkers consumed five or more drinks,by age and gender.SOURCE: Substance Abuse and Mental Health Services Administration, National Survey on Drug Use and Health 2007.Alcohol Research & Health
Reducing Underage and Young Adult Drinkingwhen a great deal of life change isoccurring. (This will be discussedfurther below.)A maturational concept of thedevelopment of drinking behaviorsdoes not account for these radicallydifferent trajectories, nor is it capableof addressing a variety of major publichealth concerns about drinking inthis and younger age-groups, suchas the following: Why does drinking start when it does? Why do some youth cross thatthreshold earlier than others? How can we explain the fact thatsome youth begin drinking in midto late adolescence in small amountsat infrequent intervals and withoutproblems, and others begin muchearlier, with some drinking at nearalcoholic levels within a short timeafter they start? Do factors unrelated to alcoholplay any significant role in thedevelopment of drinking?To address these questions,researchers have turned to a develop mental conceptual model of stabilityand change that also has served as apowerful guide for investigation infields as far removed as plant biology,evolutionary biology, and early child hood development. The model empha sizes the importance of studying earlierbehaviors and identifying the multilevelprocesses involved in creating themand the contexts in which they emerge,persist or change, increase or decline(Cicchetti 2006; Masten et al. 2008).Understanding the earlier system ofrelationships provides clues to conti nuity, even when no apparent linkexists, and discontinuity, even whenthere appears to be no organismicexplanation of it.Examples of the Utility of theDevelopmental FrameworkThe developmental framework describedabove can be used to probe the causesof, and highlight the critical issuesassociated with, underage and youngadult drinking. This is illustrated herewith three examples.Exploring the Salience of EarlierBehavior for Later Outcomes. One ofthe major principles of development isthat later behavior evolves out of earlierbehavior and that the pathway is iden tifiable, even though the later manifes-Figure 5 Number of drinking days per month and usual number of drinks per occasionfor youth (ages 12–20), young adults (ages 21–25), and adults (ages 26and older).SOURCE: Substance Abuse and Mental Health Services Administration, National Survey on Drug Use and Health, 2007.Vol. 33, Nos. 1 and 2, 2010tations may be more differentiated oreven changed in structure or appearance(i.e., morphologically changed). Forexample, there is compelling evidencethat a developmental connection existsbetween behavioral undercontrol inearly life and problem drinking andAUD outcomes in late adolescenceand early adulthood.In adolescence and young adulthood,one of the most robust correlates ofproblem alcohol use is behavioralundercontrol (Zucker et al., in press).Measures of this construct aresubsumed under a number of differ ent labels, such as disinhibition,externalizing behavior, aggressiveness,delinquency, conduct problems, andsensation seeking (Brown et al. 1996;Clark et al. 2005; Dubow et al. 2008;Guo et al. 2001; Jessor and Jessor1977). These measures are positivelycorrelated with one another, tend tooperate similarly in their relationshipswith other variables, and in factoranalyses load on the same factor (Boggand Finn, in press; Donovan andJessor 1985). Moreover, longitudinalstudies have found that behavioralundercontrol in adolescence is a robustpredictor of alcohol problems, AUDs,and other substance use disorders inearly adulthood (Brown et al. 1996;Clark et al. 2005; Dubow et al. 2008).However, the question is whether thisrelationship already exists at earlierdevelopmental stages.The evidence for such a connectionin fact is quite strong and has beenreplicated many times. A recentreview (Zucker 2006) identified fourlongitudinal studies in the generalpopulation and two studies withhigh-risk subjects that found a positiverelationship between measures ofundercontrol and aggressiveness inearly to middle childhood and problemalcohol use in mid-adolescence andsevere alcohol problems and AUDsin young adulthood. In two of thosestudies, undercontrol/disinhibitionwas identified as early as the preschoolyears. Another series of four longitu dinal studies (Schulenberg and Maggs2008) reported similar relationships.Without the conceptual frameworkof developmental theory, it is doubt35
ful that this long chain of relationshipswould have been uncovered. Yet theserelationships are highly significantbecause they indicate that some centraletiologic components that contributeto alcohol problems and AUDs arenonspecific to alcohol. And whateverthe underlying predisposition is, it issufficiently strong to emerge very earlyin the developmental course. Moreover,the strength of the developmentalpathway suggests it should be, to asubstantial degree, under genetic control.Contexts of Alcohol Use and LifeCycle Transitions. Home is the primarysource of alcohol in childhood andpreadolescence (Donovan and Molina2008) and one of the primary
underage and young adult drinking. Figure 1 Prevalence of past-year DSM-IV alcohol dependence in the United States. SOURCE: 18 years: 2001-2002 National Epidemiologic Survey on Alcohol and Related Conditions, 12-17 years: National Survey on Drug Use and Health 2003. Epidemiology of Underage and Young Adult Drinking