Transcription
Abdomen Sonography (AB)2017-18 Job Task Analysis Summary ReportAmerican Registry for Diagnostic Medical Sonography (ARDMS)Copyright 2018 Inteleos. All rights Reserved
Page 2TABLE OF CONTENTSTABLE OF CONTENTS . 2ACKNOWLEDGEMENTS . 3EXECUTIVE SUMMARY . 4BACKGROUND OF STUDY . 4METHODOLOGY . 4Job Task Analysis Working Group . 4Survey Questionnaire Development . 4Survey Process . 4Survey Administration Procedure . 4Response Rates. 4Data Analysis. 5SURVEY RESULTS . 6Demographics and Backgrounds of Participants . 6Gender . 6Race and Ethnicity . 6Location of Practice . 6Level of Education . 7Work Experience . 8Work Environment . 8Breakdown of Time. 9Conclusion . 12Discussion of Results . 12Final Approval by JTA Working Group . 12
Page 3ACKNOWLEDGEMENTSThis study was completed through the work of many individuals at Inteleos, who worked together to construct the survey,administer the survey, and analyze the data. Fifteen (15) subject matter experts also volunteered many hours to draft andreview materials before and after the survey was administered. Thank you to the 1200 ARDMS sonographer registrantsaround the nation and other countries who took the time to participate in the job task analysis survey.
Page 4EXECUTIVE SUMMARYSurvey Questionnaire DevelopmentThe American Registry for Diagnostic MedicalSonography (ARDMS) is the globally recognized standardof excellence in sonography. ARDMS is responsible forthe preparation of valid and reliable certificationexaminations in the field of sonography. Conducting jobtask analyses (JTAs) at the national and international levelsfacilitates ARDMS in evaluating the current practiceexpectations and performance requirements of thespecialty. The 2017 Abdomen Sonography (AB) JTA wasdesigned to collect information on the sonography-relatedwork activities sonographer registrants perform in practice.The results of the JTA were used in updating the testcontent outline, which guides content distribution of theAB Examination. This report details the methodology,data collection and analysis, and survey results. It alsoincludes the test content outline that resulted from theJTA.ARDMS contracted with The Caviart Group, a certificationand testing consulting group, to facilitate a kick-offmeeting. During this meeting, the JTA Working Groupdeveloped the task list and demographic questions toinclude on the survey. Tasks and demographic questionsfrom previous job task surveys were used as a startingpoint in this development. The JTA Working Groupreached consensus on a list of 99 tasks to be used in thesurvey. These tasks were divided into four (4) domains: (1)Anatomy, Perfusion, and Function; (2) Pathology, Trauma,Vascular Abnormalities, and Postoperative Anatomy; (3)Abdominal Physics; and (4) Clinical Care, Practice, andQuality Assurance. All task statements and responseoptions were relevant to RDMS-AB credentialedsonographers.BACKGROUND OF STUDYThe American Registry for Diagnostic MedicalSonography (ARDMS) recognizes that diagnostic medicalsonography is a valuable tool in the healthcare industry.There are several healthcare professions that are utilizingsonography in practice to increase the efficacy of theirpatient care.Successful mastery and demonstration of the knowledgeand skills required to hold ARDMS sonographercredentials will provide sonographers with an additionalsource of validation. This will support the veracity of thediagnostic medical sonography exams that thesepractitioners perform.The survey questionnaire was pilot-tested with the fifteen(15) members from the JTA Working Group and threevalidation group members.Survey ProcessSurvey Administration ProcedureThe survey was made available to participants as a webbased survey through the survey platform Qualtrics . Aninvitation to participate in the survey was sent via email tothe prospective respondents.METHODOLOGYARDMS sent the job task analysis survey to 2,590registrants credentialed since 2001. These registrants wereselected randomly using a stratified sampling method sothat the sample was representative of all ARDMSsonographer registrants in terms of specialty, gender, andgeographic region. The survey was made available to theparticipants for two weeks between July 24th and August6th, 2017. All responses to the survey were keptconfidential.Job Task Analysis Working GroupResponse RatesA JTA Working Group consisting of fifteen (15) subjectmatter experts (SMEs) led this project. The fifteen JTAWorking Group members are all volunteers and includedAssessment Oversight Team (AOT).A total of 1,257 (49% of those sampled) sonographersresponded to the survey. Of these, 1,143 (91% ofrespondents; 44% of the original sample) reported thatthey currently perform abdominal sonography. The finalJTA data analyses were based on the responses from the1,143 sonographers currently performing abdominalsonography.
Page 5Data AnalysisRespondents were asked the following questions for eachtask: 1) How frequently do newly certified Abdomensonographers perform this task? and 2) How important isthe task in affecting clinical decisions and patientoutcomes? The frequency and importance rating scaleswere scored 1-5. The response options for the frequencyscale were Never (1), Rarely (2), Occasionally (3), Often(4), and Always (5). The response options for theimportance scale were Not Important (1), SomewhatImportant (2), Important (3), Very Important (4), andCritically Important (5).The frequency and importance rating scales werecombined into a single measure of overall criticality(ranging from 0-16) using a hierarchical method in whichvalues on the importance scale outweigh or outrank allvalues on the frequency scale, with the exception of‘Never’ (see Table 1). Higher criticality values indicate themost critical tasks for a sonographer performing diagnosticmedical sonography examinations. These criticality valueswere averaged for each task and rank ordered andreviewed by the JTA Working Group. In addition, thecriticality values were summed within each domain. Thesum of criticality for each domain is divided by the overallcriticality score to determine the initial percentages of theexamination content in each domain.Table 1. Construction of Overall Criticality ScaleSurvey Response OptionsImportanceCritically Important (5)FrequencyAlways (5)Overall CriticalityScore16Often (4)15Occasionally (3)14Rarely (2)13Always (5)12Often (4)11Occasionally (3)10Rarely (2)9Always (5)8Often (4)7Occasionally (3)6Rarely (2)5Always (5)4Often (4)3Occasionally (3)2Rarely (2)1Not Important (1)All options0All optionsNever (1)0Very Important (4)Important (3)Somewhat Important (2)
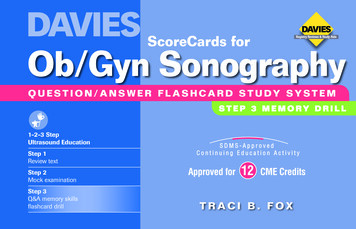
Page 6SURVEY RESULTSDemographics and Backgrounds ofParticipantsOf the 1,143 participants who were currently practicingabdominal sonography, 857 completed the demographicsportion of the JTA survey, and this section is based onthose 857 participants.GenderApproximately 88% of the respondents were female and12% were male (see Figure 1). Two (2) respondentsselected “other.”Location of PracticeOf the respondents who reported the country in whichthey practice, 86% reported practicing in the United Statesand 10% in Canada, with the other 5% of respondentspracticing in 20 other countries (see Figure 3). Among USresidents who provided the US state they practice in, overa third (35%) practiced in the southern region of theUnited States (as defined by the US Census Bureau; Figure4). One (1) respondent practiced in the District ofColumbia and two (2) in Puerto Rico.Race and EthnicityApproximately 67% of respondents were white orCaucasian, 14% of respondents were Asian, 4% black orAfrican American, and 9% Hispanic or Latino.Additionally, 4% of respondents marked “other” (seeFigure 2). Less than 1% of respondents selected AmericanIndian or Pacific Islander (not shown), and 2% ofrespondents selected more than one race/ethnicity.
Page 7Level of EducationApproximately 40% had an Associate’s degree and 42% ofrespondents had a Bachelor’s degree as their highest levelof education (see Figure 5). Within sonography-specificeducation, 49% of respondents had an Associate’s degreeand 33% of respondents had a certificate program as theirhighest level of education (see Figure 6).Almost all (86%) of respondents received their educationin the United States, 9% in Canada, and the remaining 5%of respondents were educated in 25 other countries aroundthe world (see Figure 7). A little over half of respondents(58%) had opportunities to continue their educationprovided by their employers (see Figure 8).
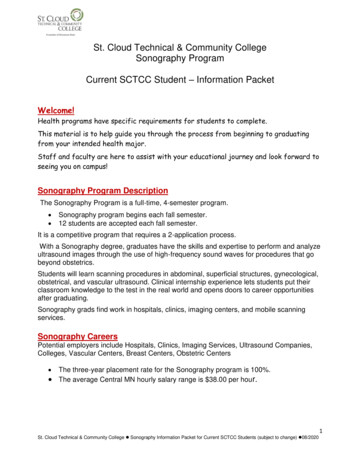
Page 8Work ExperienceApproximately 53% of respondents had been practicingsonography for fewer than 6 years, and 34% had beenpracticing for 6 to 10 years (see Figure 9). Approximatelya third of respondents performed 51-100 abdominal exams(33%) every month and another third performed over 100exams a month (32%; see Figure 10).Work EnvironmentThe respondents were asked to indicate the type ofenvironment in which they perform most of theirsonographic examinations. The most common response(49%) was a non-university hospital (see Figure 11).
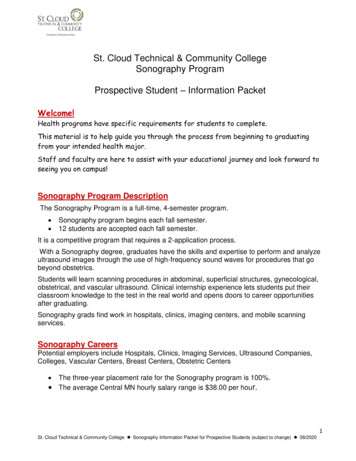
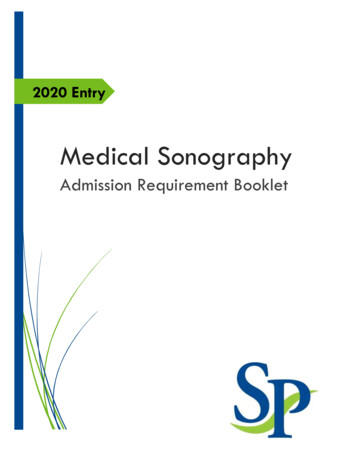
Page 9The most common number of sonographers inrespondents’ labs was less than 6 sonographers (39%)followed by 6 to 10 sonographers (29%; see Figure 12).Respondents reported that their labs performed a largenumber of abdominal exams in a month, with 59%performing over 200 (see Figure 13).Breakdown of TimeRespondents were asked to elaborate how theirprofessional time is spent. The majority of participantsspent less than half of their time as a sonography educator.The mean (Avg.) portion of time spent as a sonographyeducator among respondents was 32%, and the range ofone standard deviation (SD) away from the mean was 6%58% (see Figure 14).
P a g e 10The majority of respondents also said that the spend morethan 50% of their time performing examinations. Themean (Avg) portion of time spent performingexaminations among respondents was 70%, and the rangeof one standard deviation (SD) away from the mean was46%-93% (see Figure 15).A majority of the respondents (about 2 out of 3) said thatthey spent 100% of their time in a clinical setting. Themean (Avg) portion of time spent in a clinical settingamong respondents was 83%, and the range of onestandard deviation (SD) away from the mean was 53%112% (represented as 100%, the max possible portion oftime) (see Figure 16).
P a g e 11
P a g e 12ConclusionWhen the survey concluded, Inteleos staff analyzed the results to determine criticality ratings of each of the task statements.These results were used to develop an initial list of tasks and domain weightings. This list was shared with the JTA workinggroup via a Qualtrics survey to allow JTA working group members to review and provide feedback prior to the “Discussionof Results” call.Discussion of ResultsA call was held on November 2, 2017 to discuss the survey results with the JTA Working Group. Nine members of the JTAWorking Group and five Inteleos staff members were in attendance. The call was facilitated by The Caviart Group. Table 2shows the results shared with the Working Group. The overall frequency, importance, and criticality statistics are presented inrank order of criticality by domain and subdomain based on the survey data. Each task was reevaluated for inclusion in thefinal list based on the JTA Working Group’s opinion and criticality scoring from the survey participant. The JTA WorkingGroup decided to lower the number of tasks from 99 to 84, discarding 15 tasks with low criticality ratings and/or othercontent issues. The JTA Working Group also reviewed the preliminary content outline based on the data and the outline basedon their task removals/combinations to decide what percentage of the examination should be in each domain. The JTAWorking Group was allowed to deviate 10% in each domain from the preliminary content outline based on the 84 tasks.Table 2 below shows this process and the resulting domain weightings.Table 2. Content domain breakdown before and after JTA Working Group Review of Survey ResultsBased on JTADomainAnatomy, Perfusion,and FunctionPathology, Trauma,Vascular Abnormalities,and PostoperativeAnatomyAbdominal PhysicsClinical Care, Practiceand Quality AssuranceTotalAfter Task SelectionFinal on25%-30%30%#Tasks27CriticalitySum231% ofTotal25%#Tasks26CriticalitySum226% %-47%42%Final Approval by JTA Working GroupAfter the call, the JTA Working Group completed an approval survey (administered March 17-March 25, 2018). Somequestions were raised, and minor edits proposed through the survey. The proposed edits were reviewed, clarified and minoredits were made. There were no changes made to the final tasks and domain weightings. The Chair and co-chair of the JTAworking group approved these changes on a call held on April 5, 2018. The ARDMS Council voted and approved thiscontent outline on June 24, 2018.
P a g e 13Abdomen Sonography Examination Content Outline(Outline Summary)#DomainSubdomainPercentageAnatomy, Perfusion, and FunctionAssess physical characteristics of anatomic structuresAssess perfusion and function of anatomic structures30%Pathology, Vascular Abnormalities,Trauma, and Postoperative AnatomyAssess anatomic structures for pathologyAssess anatomic structures for vascular abnormalitiesAssess anatomic structures for trauma-relatedabnormalitiesAssess aspects related to postoperative anatomyApply concepts of equipment/image optimizationApply concepts of imaging artifacts12Abdominal Physics34Clinical Care, Practice, and QualityAssuranceIncorporate clinical data with performed studyIncorporate clinical standard/guidelines withperformed studyObtain accurate measurementsAssist/support during procedures42%8%20%(Detailed 14.1.B.Anatomy, Perfusion, and FunctionAssess physical characteristics ofanatomic structures (normalanatomy, anatomic variants,congenital anomalies)Biliary systemBreastChestLiverNeck (including: thyroid, parathyroid,salivary glands, lymph nodes)PancreasPenisPeritoneal cavity (including: stomach,bowel, appendix)ProstateRetroperitoneum (including: greatvessels & branches)ScrotumSpleenSuperficial structures (for example:abdominal wall & subcutaneoustissue)Urinary systemAssess perfusion and function ofanatomic structuresKnowledge and/or skill related to anatomy, perfusion, andfunctionKnowledge of normal anatomy, anatomic regions, and anatomicvariantsKnowledge of sonographic appearance of anatomic structuresAbility to recognize and utilize anatomic landmarks in obtainingand documenting diagnostic imagesAbility to recognize and apply proper scan technique in obtainingand documenting diagnostic imagesAbility to recognize, evaluate and document congenital anomalies
P a g e .2.A.12.2.A.13.Biliary systemChestLiverNeck (including: thyroid, parathyroid,salivary glands, lymph nodes)PenisPeritoneal cavity (including: stomach,bowel, appendix)ProstateRetroperitoneum (including: greatvessels & branches)ScrotumSpleenSuperficial structures (for example:abdominal wall & subcutaneoustissue)Urinary systemPathology, Vascular Abnormalities,Trauma, and Postoperative AnatomyAssess anatomic structures forpathologyAbdominal wall for hernia (forexample: ventral, inguinal, incisional)Adrenal glands for masses,hemorrhage, etc.Biliary system for infection, masses,metastatic disease, obstructions, etc.Breast for infection, abscess, masses,etc.Chest for fluid, masses, etc.Gastrointestinal system for masses,obstruction, pyloric stenosis,intussusception, etc.Joints for abnormalities (for example:fluid)Liver for hepatitis, fatty infiltration,cirrhosis, neoplasm, abscess, cyst, etc.Neck (including: thyroid, parathyroid,salivary glands, lymph nodes) fordiffuse parenchymal disease,inflammation, masses, etc.Pancreas for infection, masses,obstruction, etc.Penis for abnormalitiesPeritoneal cavity (including: stomach,bowel, appendix) for fluidPopliteal fossa for abnormalities (forexample: masses, fluid)Knowledge of normal vascular anatomy and hemodynamicsAbility to recognize appearance of normal vascular flow patternsAbility to recognize and utilize anatomic landmarks in evaluatingand documenting perfusion and functionAbility to recognize and apply proper scan technique in evaluatingand documenting perfusion and functionKnowledge and/or skill related to pathology, vascularabnormalities, trauma, and postoperative anatomyKnowledge of etiology/pathophysiology of abnormal perfusionand functionAbility to recognize ultrasound findings related to abnormalitiesof anatomy, perfusion, and function in obtaining anddocumenting diagnostic imagesAbility to recognize and apply proper scan technique in evaluatingand documenting pathologyAbility to recognize foreign bodies, infection, fluid, masses, etc.Knowledge of hernia types and their sonographic appearance
P a g e tate for parenchymal disease ormasses (for example: benign prostatichypertrophy)Retroperitoneum (including: greatvessels & branches) for fibrosis,lymphadenopathy, etc.Scrotum for fluid, hernia, masses,infection, parenchymal disease, etc.Spleen for splenomegaly,parenchymal changes, masses, etc.Superficial structures (for example:abdominal wall, subcutaneous tissue)for foreign bodies, infection, fluid,masses, etc.Urinary system for masses,obstruction, parenchymal disease,infection, etc.Assess anatomic structures forvascular abnormalitiesLiver for Budd-Chiari syndrome,arteriovenous fistula, portal veinthrombosis, collateralization, etc.Retroperitoneum (including: greatvessels and branches) for aneurysm,dissection, thrombus, etc.Scrotum for torsion, varicocele, etc.Spleen for infarction, hemangiomas,etc.Urinary system for renal arterystenosis, arteriovenous fistulas, etc.Assess anatomic structures fortrauma-related abnormalitiesHepatic systemPenisScrotumSpleenSuperficial structures (for example:abdominal wall, subcutaneous tissue)Urinary systemFocused assessment for free fluidrelated to traumatic eventsAssess aspects related topostoperative anatomyAnatomy of transplanted organsPerfusion and function oftransplanted organsComplications related to organtransplantsKnowledge of anatomic and vascular changes associated withvascular abnormitiesKnowledge of sonographic findings associated with vascularabnormalitiesAbility to recognize and apply proper scan technique in evaluatingand documenting vascular abnormalitiesKnowledge of sonographic appearance as a result of traumaAbility to rapidly prioritize and evaluate sonographic findings dueto traumaAbility to perform focused assessment for free fluid following atraumatic eventAbility to recognize and apply proper scan technique in evaluatingand documenting traumaKnowledge of hemodynamics of transplanted organsKnowledge of common causes of transplant failureAbility to recognize signs of rejectionAbility to adjust scan technique based on patient condition andsurgical history
P a g e 5.Abnormalities in Postsurgical AnatomyAbnormalities in Postsurgical BreastAbnormalities (for example: recurrentdisease, lymphadenopathy) inpostsurgical neckImplanted medical devices (forexample: transjugular intrahepaticportosystemic shunt [TIPS])Abdominal PhysicsApply concepts of equipment/imageoptimizationUse appropriate transducer (forexample: curvilinear, linear, phasedarray)Use two-dimensional, real-time, grayscale imaging (for example: B-mode,compound, harmonic)Use Doppler (for example: color,power, pulsed wave)Apply concepts of imaging artifactsAssess artifacts of gray-scale imaging(for example: shadowing, resonance,comet tail)Assess artifacts of Doppler imaging(for example: twinkle, spectralbroadening)Clinical Care, Practice, and QualityAssuranceIncorporate clinical data withperformed studyAssess indications for examinationrequestedAssess relevant clinical lab values forexamination being performedAssess relevant family history andpatient signs/symptoms forexamination being performedCorrelate ultrasound findings withprevious imaging resultsEvaluate images from other imagingmodalities (for example: computedAbility to distinguish characteristics of common anastomosis sitesAbility to recognize fluid collectionsAbility to interpret and integrate surgical history with sonographicfindingsKnowledge of surgical procedures used in organ transplantKnowledge of surgical zones of the neckAbility to evaluate and document findings within surgical zones ofthe neckKnowledge of patterns and sonographic appearance of diseaserecurrenceAbility to evaluate transjugular intrahepatic portosystemic shunts(TIPS)Ability to recognize and apply proper scan technique in evaluatingand documenting postsurgical findingsKnowledge and/or skill related abdominal physicsAbility to select the appropriate transducer and machine presetsbased on body habitusAbility to use acoustic windows creatively to optimizevisualizationAbility to adjust machine settings to maximize penetration whileminimizing resolution lossKnowledge of appropriate application of Doppler techniquesAbility to manipulate color, power, and pulsed wave settings toaccurately display and measure blood flowAbility to recognize artifacts and correlate them with anatomyand pathologyAbility to manipulate machine settings to enhance or minimizeartifactsKnowledge and/or skill related to clinical care, practice, andquality assuranceKnowledge of appropriate indications and contraindications for aspecific exam and/or procedureKnowledge of potential effects of patient medications on an examor procedureKnowledge of lab values relevant to specific examinationsAbility to obtain and evaluate patient history relevant to theexamAbility to assimilate patient’s signs and symptoms and modify theexam/or describe the findingsAbility to modify the exam based on information from othermodalitiesAbility to localize pathology for sonographic correlationAbility to modify the exam based on real-time findings
P a g e 17tomography, magnetic resonanceimaging, nuclear medicine, 4.C.2.4.D.4.D.1.4.D.2.4.D.3.Incorporate clinicalstandard/guidelines with performedstudyCommunicate effectively with thepatient, physician, and others,including communication of findingsthat require immediate actionInform patient or referringpractitioner of examinationpreparations (for example: fasting forbiliary imaging)Maintain and protect patientconfidentiality/privacyModify the examination based onpatient condition and/or sonographicfindingsUse multiple patient positions andscan planes to evaluate anatomicstructuresObtain accurate measurementsObtain measurements of anatomicstructuresObtain measurements of DopplerwaveformsAssist/support during proceduresObtain consent form and patient labresults prior to the procedureProvide ultrasound guidance forproceduresEvaluate for post-proceduralchanges/complicationsKnowledge of modalities associated with the exam beingperformedAbility to utilize resources, such as physicians, literature, or peersAbility to communicate with patient in a professional andappropriate manner to effectively explain procedures, dealwith inappropriate behavior, and engage patient cooperationAbility to communicate using appropriate medical terminologyAbility to modify exam preparation, patient position, and/orimage acquisition based on patient condition and/orsonographic findingsAbility to recognize findings and/or situations that requireimmediate action and respond effectivelyKnowledge of appropriate patient preparation for an exam andknowledge of factors that may affect patient preparation (forexample: patient history, patient condition, sequencingrequirements of multiple modality exams)Knowledge of sonographer scope of practice and regulationsregarding patient information and interactionsKnowledge of normal measurement rangesKnowledge of proper techniques for measuring anatomicstructuresKnowledge of hemodynamicsKnowledge of normal and abnormal Doppler waveformsAbility to analyze Doppler measurementsAbility to distinguish artifacts from actual blood flowAbility to apply knowledge of measurement techniques (forexample: Doppler and gray-scale)Knowledge of sonographer's role in obtaining consentAbility to verify and document patient consentAbility to verify correct patient, side (laterality), and siteKnowledge of contraindications for specific proceduresKnowledge of proper safety precautions in interventionalproceduresKnowledge of equipment and materials used for a specificprocedureKnowledge of interventional procedures and sonographer's roleKnowledge of protocols during surgical procedures, related to thesonographer's roleAbility to adapt protocol due to different circumstancesAbility to optimally display the needle path and tipAbility to recognize implanted medical devicesKnowledge of potential post-procedural complications
facilitates ARDMS in evaluating the current practice expectations and performance requirements of the specialty. The 2017 Abdomen Sonography (AB) JTA was designed to collect information on the sonography-related work activities sonographer registrants perform in practice. The results of the JTA were used in updating the test