Transcription
Bureau of Justice Assistance (BJA)Comprehensive Opioid, Stimulant, and Substance Abuse Program (COSSAP)Peer Recovery Support Services in New YorkOpioid Intervention Courts:Essential Elements and Processes for Effective IntegrationAbstractOpioid intervention courts (OICs)—a relatively new form oftreatment and recovery court—have shown early promisein addressing the needs of justice-involved individualswith opioid use disorders (OUDs). This article describesthe efforts of New York State OICs to heighten theirimpact by incorporating peer recovery support services(PRSS) into their work. The authors present a frameworkfor conceptualizing the adaptation and integration ofPRSS into court settings, identifying essential elements ofcomprehensive programs, essential integration processes,key program design factors, and drivers of success. Thelike fentanyl, have contributed to this epidemic. TheNew York State Department of Health 2019 Annual Reportindicates that “deaths involving opioids tripled from 2010–2017, from 5.4-16.1 deaths/100,000 population”(New York State Department of Health, 2019). The Centersfor Disease Control and Prevention’s (CDC) provisional dataposits that “overdose death rates in NYS [New York State]increased 30% from October 2019 to October 2021, whichis an historically high increase” (CDC, 2021). Effectivelyaddressing the epidemic—including preventing opioid usemorbidities and mortalities—requires a collaborative andcomprehensive approach across multidisciplinary systems.framework suggests that while the core elements remain theIncreasingly, PRSS are being incorporated into programssame, effective integration of PRSS programs will vary fromin various settings as a part of diversified efforts to addresssite to site.opioid use disorders. The New York State Office of CourtAdministration (OCA) is working to integrate peer recoveryIntroductionThe opioid epidemic continues to have devastatingconsequences across the United States with more than70,000 Americans dying from a drug overdose in 2019, 71percent of those overdoses involving opioids (OverdoseDeath Rates National Institute on Drug Abuse [NIDA], 2021).Heroin, prescription pain relievers, and synthetic opioids,professionals into its OICs as it adopts this new modelfor saving lives. As a part of those efforts, a conceptualframework was developed to assist the courts in successfullyconceptualizing, planning, and integrating peers into theirwork. This article describes the innovation involved inintegrating PRSS into OICs, their framework components,and early lessons learned.
The Emergence of a New CourtModel: The Opioid InterventionCourtPrior to arraignment, court staff go to the jail toSince the late 1980s, treatment courts, problem-solvingare administered a biopsychosocial screening by ancourts, or specialty courts have developed into a widelyon-site team of treatment professionals and caseused approach to address the needs of justice-involvedcoordinators immediately following arraignment.individuals with behavioral health needs. These courtsBased on the results, each consenting individual isdisrupt the cycle of relapse, crime, and reincarceration bytransported to an appropriate treatment provider,working to resolve the underlying personal issues related towhere most begin medication-assisted treatmentjustice involvement (Schaffer, 2011; Michell et al., 2012). Thewith buprenorphine, methadone, or naltrexone.first—and arguably best known—of these courts were drugThe process of initial interview, arraignment, bio-treatment courts launched in Miami-Dade County, Florida.psycho-social screening, and transfer to treatment isFamily courts, mental health courts, and veterans’ courtscompleted within 24 hours of arrest.interview defendants, using a brief survey developedby the court to identify those at risk of opioidoverdose. Individuals identified to be at high riskfollowed. There are now more than 3,000 such courts in theUnited States, serving approximately 120,000 individualsOnce connected with a treatment provider, theannually (Office of National Drug Control Policy, 2011).participant receives a comprehensive clinicalThis article refers to these courts by the emerging termassessment and an individualized treatment plan. OIC“treatment and recovery courts” (TRCs) as it reflects theirstaff provide daily case management for participants,overarching purpose.including helping with transportation, doing curfewOpioid intervention courts (OICs) are the newest additionto the TRC contingent. OICs present opportunities toaddress the opioid epidemic and prevent overdose deathsby immediately linking participants to evidence-basedtreatment, including medication-assisted treatment (MAT)and recovery support services. OICs differ from drug courtsin several ways: they are pre-plea, voluntary (in that theydo not rely on legal leverage), short-term, and focusedon stabilization and crisis intervention. Drug courts areanalogous to a long-term care hospital, providing extendedsupport for court-involved individuals with substance usedisorders (SUDs); OICs are like emergency rooms, offeringshort-term services to individuals at high risk of overdoseto prevent overdose and reduce other barriers whilechecks, and linking participants with a primarymedical doctor and a range of recovery supportservices. Participants must return to the opioid courtevery business day for 90 days to see the judge forprogress updates. Participants are randomly testedfor drugs to monitor their clinical needs. The courtdoes not sanction participants for positive drug tests;rather the results of the toxicology test are used tomake adjustments to the participant’s treatment plan,such as increasing treatment intensity or changingmedications, and to help the court recognize whena participant is in danger . . . . While a defendantis participating in the Buffalo Opioid Court, theprosecutor’s office suspends prosecution of the case.encouraging early steps toward recovery. The country’s firstThe Buffalo OIC has shown promise. Findings from anOIC was launched in Buffalo, New York, in 2017. Since then,evaluation of the Buffalo OIC, conducted by NPC Research,multiple jurisdictions have adopted the model, which reliesdemonstrate that OIC participant death rates “were reducedon day-of-arrest intervention, OUD treatment, daily judicialby half and [participants] had lower rates of recidivism whensupervision, and wraparound services. The Center for Courtcompared to opioid users who were traditionally processedInnovation (2019) described the Buffalo OIC’s operations asthrough the criminal justice system and indicate a costfollows:savings of 301,744/participant” (NPC, 2020). As a result,2 / Peer Recovery Support Services in New York Opioid Intervention Courts
the NYS OCA is developing OICs in every judicial district.reduced substance use and SUDs, decreased return toThe goal is to integrate this new collaborative care modeluse rates, improved relationships with treatment providersacross the state, prioritizing interventions for offenders atand social supports, increased treatment retention, andhigh risk of overdose.greater treatment satisfaction (Eddie et al., 2019). ResearchIn February 2019, the NYS OCA’s Division of Policyand Planning, in cooperation with the Center for CourtInnovation (The Center), released the first state guidelinesthat defined this new problem-solving court based on theBuffalo model. The Center then worked with court andtreatment experts to draft national guidelines published inThe 10 Essential Elements of Opioid Intervention Courts(Center for Court Innovation, 2019), with the support ofthe U.S. Department of Justice, Office of Justice Programs,Bureau of Justice Assistance (BJA); the Substance Abuseand Mental Health Services Administration (SAMHSA);and the Center for Substance Abuse Treatment (CSAT).The “Essential Elements” include a focus on broad legaleligibility, immediate screening for risk of overdose,informed consent after consultation with defense counsel,suspension of prosecution during stabilization, rapid clinicalsuggests PRSS in community-based programs may lead toincreased use of detoxification programs and residentialSUD treatment (Deering et al., 2011), as well as reducedrehospitalization rates following treatment (Min et al.,2007). Research also suggests that integration of PRSSservices can assist in getting individuals to treatment fasterfollowing SUD treatment referral (James, Rivera, and Shafer,2014), as well as reducing criminal behavior and recidivismrates (Rowe et al., 2007; O’Connell et al., 2017). SUDs arechronic and require long-term management to maintainrecovery. Peer recovery professionals provide a “range ofperson-centered and strength-based supports for longterm recovery management. These supports help people inrecovery build recovery capital—the internal and externalresources necessary to begin and maintain recovery” (Bestand Laudet, 2010; Cloud and Granfield, 2008).assessment, the immediacy of medication for opioid useThrough the engagement and employment of peer recoverydisorder (MOUD), the use of evidence-based treatmentprofessionals in TRC, programming has grown over thefor opioid and polysubstance abuse, frequent judicialpast several years partly at the behest of funders as thesesupervision, intensive case management, and performanceservices are not yet well-researched. Two studies show theirevaluation metrics to identify service gaps and makepromise. The first study indicates that peer support groupsprogram improvements. An essential core element ofmay help address racial disparities in graduation ratesOICs is recovery support services, including PRSS—non-(Gallager and Wahler, 2017). The second study found thatclinical, social supports provided by persons with livedrecidivism rates for court graduates who were matched withexperience of addiction, recovery, and criminal justicepeer recovery professionals were reduced by half (Belenko,involvement. PRSS are critical to the operation of OICsLaPollo, Gesser, and Peters, 2018; Belenko, LaPollo,due to the voluntary nature of the court model andMarlowe, Rivera, and Schmonsees, 2019; Belenko et al.,the need for immediate engagement in services and2019).supports to address the high risk of overdose.According to the Centers for Medicare & Medicaid Services(CMS), peer support services are an evidence-based modelof care in which a qualified peer recovery professionalassists an individual with their recovery from substanceuse and mental health disorders (CMS, 2007). Researchfindings to date tentatively speak to the potential of PRSSto improve outcomes across a variety of settings, includingAdding Peer Recovery SupportServices to Treatment andRecovery CourtsIn theory, adding PRSS to TRCs is a straightforwardundertaking: Simply add peer recovery professionals tothe existing multidisciplinary teams composed of judges,prosecutors, defense attorneys, court administrators,3 / Peer Recovery Support Services in New York Opioid Intervention Courts
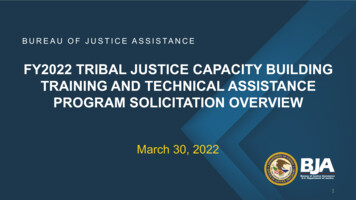
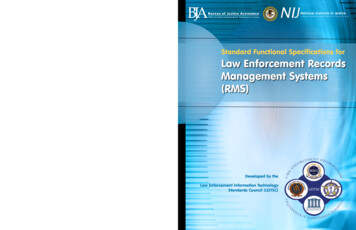
behavioral health clinicians, social workers, and other courtIn combining their lived experience of addiction, recovery,staff. In practice, it is more complex because of the natureand criminal justice involvement with practice-specificof peer relationships, the variety of roles and tasks thattraining, peer profession-specific ethics, and role-specificpeer professionals can have, and the range of possible peercertification, peer recovery professionals bring uniquesupports.philosophies, values, skills, and resources to supportingThe term ”peer” identifies a single person with relevantlived experience, a designation that positions the person asdistinct from others. PRSS programs are grounded in a set ofprinciples that have emerged from the experience of peoplein long-term recovery and their allies. The primary principleis that “recovery is a strengths-based process,” which keepsthe focus on building recovery capital and developing self-individuals on their path to recovery—known as ”peerpractice.” Peer practice arose to address the limitationsof the acute care model for treating addiction; it supportsindividuals along their path of recovery before, during,after, or instead of treatment (White, 2009a). This approachmay conflict with that of other specialties on the TRCmultidisciplinary team, especially medically focused ones.efficacy, while understanding that the process of change canPeer recovery professionals have many different titles andlook different based on the individual. Acknowledgment ofroles, depending on the setting and context. Additionally,the change process is another primary principle in meetingsimilar roles may have different titles based on jurisdictionindividuals “where they are at.” Peer recovery professionalsand regulatory oversight bodies. In the SUD realm, inare supportive, rather than directive or prescriptive, andNew York State, the most well-known title is the certifiedfocus on building strengths and resiliencies. Thus, recoveryrecovery peer advocate (CRPA). Others, including forensicbecomes a primary focus for both the peer professionalpeer recovery specialists, peer navigators, or crisisand the individual seeking support. Other foundationalinterventionists, are summarized in table 1. The core body ofprinciples relate to the authority and expertise of livedknowledge is the same across the roles, but the focus of theexperience (Borkman, 1976; Riddick, 2017), mutuality,core competencies varies in different contexts.collaboration, and reciprocity, with relationships built onrespect, trust, self-efficacy, and empowerment (White,2009a; Reif et al., 2014; Hoffman et al., 2019).Table 1. Examples of Peer Recovery Specialist RolesTitle/RoleKey TasksLocationsCertified RecoveryPeer Advocate/Recovery CoachGuide and mentor the person seeking or inrecovery, help identify and remove obstaclesand barriers, and support connections to therecovery community and other resources usefulfor building recovery capital.Recovery community centers, correctionalsettings, inpatient and outpatient SUD treatmentprograms, behavioral health clinics, communitybased settings, recovery residencesForensic PeerSpecialistSupport people involved with the criminaljustice system as a mentor, guide, and resourceconnector while the individual is incarcerated,on probation or in lieu of probation, or in thereentry process.Jails, prisons, jail diversion programs, drugcourts, community-based programsRecovery/CrisisInterventionistProvide support and guidance to the person atHospital emergency rooms, police and firean early (crisis) intercept point along the recovery departments, community-based street outreachsupport continuum, linking them to treatment or or harm reduction programs, crisis centersother recovery support services as requested.Family-SupportedRecovery4 / Peer Recovery Support Services in New York Opioid Intervention Courts
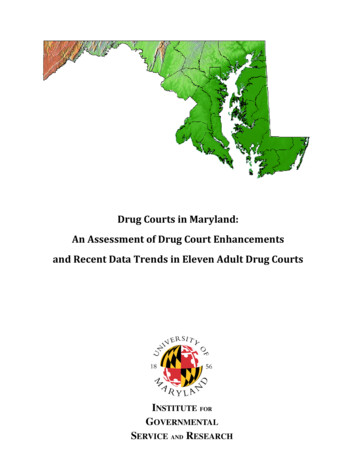
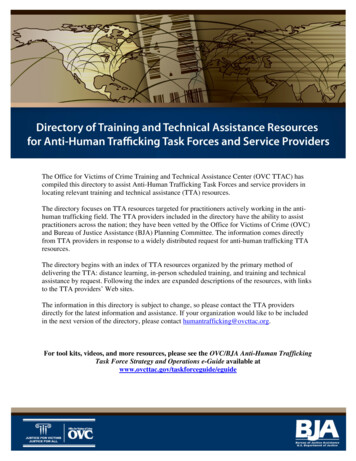
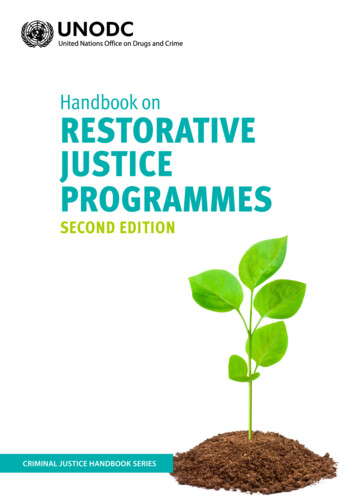
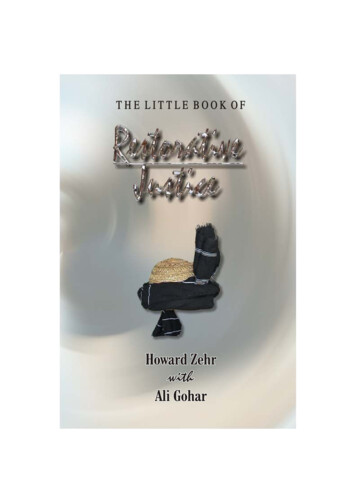
Title/RoleKey TasksLocationsPeer NavigatorProvide support and guidance for accessingappropriate services from complex medical,treatment, and social service systems, includingthe application process for health insurance andother entitlement benefits.Community-based street outreach or harmreduction programs, community health clinics,public health departmentsPRSS are person-centered: Through recovery (goal)The multifaceted nature of PRSS provides them with anplanning and resource sharing, a peer recovery professionalability to adapt to a variety of settings. However, successfulassists others in building their recovery capital—a processintegration takes careful forethought. NYS OCA approachedof making healthful choices, creating or recreating athe Training and Technical Assistance Center for PRSS,meaningful life, and being of service to family, friends, andfunded by BJA, to assist new and emerging OICs. The Newcommunity, leading to a sustainable life in recovery. ThereYork State Unified Court System (NYS UCS) worked withare four categories of social support: (1) emotional, (2)Altarum to develop a conceptual framework, summarizedinstrumental, (3) informational, and (4) affiliational (Cobb,in figure 1, that courts can use to conceptualize, plan, and1976; Salzer, 2002). Under this schema, a wide array of PRSSintegrate PRSS successfully.can be offered. Examples for each category are provided intable 2.Table 2. Types of Peer Recovery Support ServicesType ofSupportDescriptionPRSS ExamplesTech-assisted PRSS ExamplesEmotionalDemonstrate empathy, care,or concern to bolster selfesteem, confidence, andhope. One-on-one peer mentoring orcoaching Peer-led support groups Provision of support duringchallenging moments Modeling the use of recoveryoriented skill sets Telephone recovery support Video recovery check-ins Zoom support groupsInformationalShare knowledge andinformation, and provide lifeor vocational skills training. Discussing the therapeutic courtprocess Training for job readiness Offering wellness seminars orclasses Training on self-advocacy Offering parenting classes One-time webinars Learning communities Self-directed learning modulesInstrumentalProvide concrete assistanceto help accomplish tasks,increase access andopportunities, and reducebarriers. Accessing community health andsocial services Providing housing or child-carevouchers Providing public transportationpasses Tech on loan Paperwork clinic Online resource bulletin boardAffiliationalFacilitate contacts with otherpeople to promote learningof social and recreationalskills, create community, andfoster a sense of belonging. Arranging outings or activities,such as sober sports, alcohol anddrug-free dances, movie nights Celebrations and rituals Community coffee breaks Live-streamed group activities(e.g., meditation, yoga, fitness) Game playing sessions5 / Peer Recovery Support Services in New York Opioid Intervention Courts
Figure 1. Conceptual Framework for PRSS IntegrationEssential Elements Certified peersPre-court/early engagementChoiceAccessRecovery capital assessmentRecovery planning and check-insRecovery peer support groupsAvailability of other peer supportsLinkage to the recovery communityPost-court engagementCommunity educationCourt stakeholdersDesign FactorsDrivers of Success ConceptualFrameworkfor PRSSIntegration Partner type(s) Peerness perspective Comprehensiveness, duration,setting(s) ment/climateInfrastructure and resourcesEthical frameworkTraining and supportData and decision-makingEssential Integration Processes Prepare to integratePlan an appropriate menu of PRSSSet policies and proceduresLaunch and refine the programSchedule regular partner check-insPromote recovery orientationEssential Elements of PRSS inTreatment and Recovery CourtsCertification standardizes the core body of knowledge andFollowing the example of The Ten Essential Elements ofcompetency and ethical requirements set by independentOpioid Courts (Center for Court Innovation, 2019), NYScore competencies for the role at entry and advanced levels.Candidates demonstrate their proficiency in meeting thecertification boards through an examination and/or otherOCA sought to define the essential elements of peercompetency assessment. In many states, certifications alsosupport services in OICs. Three primary methods werehelp provide access to a reliable funding stream, as servicesused to identify potential elements: (1) review of relevantprovided by certified peers become Medicaid-billable. Inacademic research; (2) examination of publications by courtthe TRC context, it is essential to select and hire certifiedprofessional organizations; and (3) an audit of practices ofpeers or partner with an agency that hires them, such as ancourt-affiliated PRSS programs across the country. WhatSUD treatment provider, social service agency, or recoveryemerged were essential elements of peer support servicescommunity organization.in TRCs in general that can be applied to or adapted forOICs. These elements are described below.In New York, “certified peer specialist” is a term that isreserved for mental health peers; SUD peers whose servicesCertified Peer ProfessionalsWith the increasing interest in and expansion of peersupport services, peer credentialing emerged in theearly 2000s with state-recognized certification programsfor mental health and SUD peer recovery professionals.are Medicaid-reimbursable are called CRPAs. CRPAs havepractice-specific education, profession-specific ethics, androle-specific certification. They “bridge the gap betweenclinical prevention-treatment providers and relevantmultidimensional resources in the community” through“purposeful conversations using role modeling, motivating,6 / Peer Recovery Support Services in New York Opioid Intervention Courts
problem solving, and resourcing” (adapted from trainingNYS OICs incorporate CRPAs into the court process asmaterials by Ruth Riddick, Sobriety Together, 2017). Inearly as possible to engage individuals in a supportive andNYS OICs, CRPAs are integral parts of the multidisciplinaryproductive way. In several NYS courts, the CRPA is the firstopioid court team, providing support to participants duringperson point of contact for individuals who are consideringa very challenging time; their roles and tasks employedparticipation in the OIC. Court administrators stated thatwithin the NYS OIC system are summarized in the boxes inhaving the first engagement be with a peer rather than afigure 2.court staff member changes the dynamic. Individuals appearto be more receptive to the information received from aPre-Court/Early Engagement With PeerRecovery ProfessionalsPeer recovery professionals have the ability to engageindividuals outside the formal structures of the courtand traditional clinical service locations. This providesan opportunity to fill critical gaps to keep individualsfrom disconnecting or withdrawing from treatment and/peer because of their lived experience, meaning they canrelate to the situational experiences the individuals presentwith. Individuals perceive the CRPA as helping them throughshared experience to make an autonomous decision toparticipate in the court programming.Choiceor services. Research suggests outreach by peer recoveryChoice, self-direction, and empowerment are foundationalprofessionals may increase individuals’ self-awareness ofvalues of PRSS. These are put into practice in severalproblematic substance use (Boyd et al., 2005) and leadways, such as supporting the many pathways to recovery,to greater utilization of services among those needingbelieving the person seeking recovery is fully capable oftreatment (Deering et al., 2011).making informed choices, and respecting an individual’sFigure 2. Opioid Intervention Court Activities and CRPA Tasks7 / Peer Recovery Support Services in New York Opioid Intervention Courts
goals, objectives, and preferences (SAMHSA CSAT, 2009).is best predicted on the basis of recovery assets, notIn the general court context, choice means that an individualpathologies (White and Cloud, 2008). A recovery capitalshould be able to choose whether to participate in peerassessment is a strengths-based tool to measure thesupports. Since participation in OICs is voluntary, thestrengths, resources, motivation, and aspirations that courtchoice is whether to engage with the court at all. This re-participants have that can support them in their recoveryemphasizes the early role of the peer recovery professionaljourney (Groshkova, Best, and White, 2013). It is also a tooland points to the need for harm reduction and recoverythat programs can use to quantify individual-level (Laudetsupports if the individual elects not to participate in OIC.and White, 2008; Sánchez, Sahker, and Arndt, 2020) andprogram-level recovery outcomes (as opposed to treatmentAccessoutcomes).Peer support services and peer recovery professionals needTRCs can also play an important role in expandingto be easily accessible to court participants in terms ofcommunity recovery capital by partnering to create physical,location and time of day so that supports are available aspsychological, and social spaces in the community withinthey are needed. There are several strategies for facilitatingwhich recovery can thrive (White, 2008; White, 2009; Evans,access: having peer recovery professionals at the courtLamb, and White, 2013; Altarum Institute, 2017). In doingduring its hours of operation, offering mobile services,so, programs can also use the aggregate results of recoveryproviding access to peers in community-based settings, orcapital assessments to assess changes in communityoffering technology-assisted (phone, text, web-based) peerrecovery capital.support services. One respondent noted that a CRPA isavailable to their OIC participants 24 hours a day for crisissupport and to offer recovery supports between traditionalservice appointments. Another noted that CRPAs could beeffective in preventing relapse. When a participant sharesthat they are thinking of returning to using, the CRPAcan offer strategies for intervening on such thoughts andfeelings as well as options, such as taking the person toa treatment center if asked. The ability to connect withindividuals is also important for peer recovery professionalsto effectively do their work. According to respondents,CRPAs gauge the level of contact needed. The barriers theymay have in connecting with participants—initially and on anongoing basis—need to be assessed and addressed withinthe program design.Recovery Planning and Recovery Check-InsA recovery capital assessment is a strengths-based tool tochart current progress and help to identify opportunitiesfor growth. The recovery plan is a roadmap that takes intoaccount the specific strengths, desires, and motivationsof the recovering individual. Recovery planning assistsindividuals in (a) articulating and visualizing the kind oflife they would like to have in recovery, (b) outlining theirpersonal recovery goals, (c) developing action steps toachieve their goals related to the essentials for sustainedrecovery (e.g., a safe and affordable place to live, steadyemployment and job readiness, educational and vocationalskills, life and recovery skills, health and wellness, a sense ofbelonging and purpose, community and civic engagement,Recovery Capital Assessmentand recovery support networks), and (d) can act as anevaluation tool for individuals to assess where they are inRecovery is a journey that involves building recovery capital,their recovery process and make revisions to their actionwhich is the sum of the strengths and supports—bothsteps and goals as needed.internal and external—that are available to help someoneinitiate and sustain long-term recovery from addiction(Granfield and Cloud, 2004; White, 2008). Stable recoveryRecovery check-ins improve the likelihood of sustainedsobriety and engagement in a recovery program (Scott andDennis, 2003). They provide opportunities for participants8 / Peer Recovery Support Services in New York Opioid Intervention Courts
to reflect on progress toward the goals they set in theirinvolve the participation of a subject-matter expert. Peerrecovery plan, talk about challenges and barriers, andsupport groups also offer unique advantages for engagingidentify resources (Braucht, n.d.). The check-in can alsounderserved or difficult-to-engage populations (Rowe et al.,serve as a reminder of the next scheduled court, treatment,2007; Tracy et al., 2011) as they may build rapport based onor social services appointment. Additionally, check-ins alsoshared experiences.help to develop individual accountability and begin theprocess of encouraging self-efficacy.Availability of Other Peer SupportsThe practice of recovery planning and check-ins will varyCollaborating with a peer recovery professional on recoverydepending on both individual and program factors. Forcapital assessments, recovery planning, and recovery check-one NYS OIC, there are three built-in meetings (mandatoryins strengthens the desire, motivation, and coping skillscheck-ins): (1) an overdose awareness workshop (firstfor change, all of which may be helpful in establishing andmonth), (2) a medication management workshop, and (3) amaintaining recovery. Opportunities to practice new skills indischarge planning workshop. The program also encouragessafe and supportive environments (offered through optionsparticipants to have check-ins with their peer recoverysuch as classes, workshops, and social and recreationalprofessional each time that they appear in court. Anotheractivities) have also been found to be helpful (O’Connelloperates off a different schedule: in the initial stages ofet al., 2017; Page and Townsend, 2018; Best et al., 2020).the engagement, the peer recovery professional helpsThese extended informational and affiliational supportsparticipants in the development of their wellness plan.may be difficult to offer within the TRC setting; therefore,They schedule check-ins based on the goals participantspartnering with the community provides opportunitiesidentify they want to achieve. The wellness plan will helpto increase access to those resources that can supportto determine the number and frequency of check-ins thatmeaningful and lasting change.might be helpful. Recovery check-ins should be scheduledat regular intervals, more frequently in early recovery and atLinkage to Broader Recovery Communitytransition points, less frequently as time progresses, and asIt is said that the opposite of addiction is not sobriety butparticipants become more established in their recovery.connection (Johann Hari). Leamy et al. (2011) posited thatRecovery Peer Support Groupsthe essential elements of recovery are connectedness, hope,a positive sense of identity, meaning, and empowerment.In addition to one-on-one support, peer-facilitated orResearch indicates there are two social factors—socialpeer-led groups are another
Death Rates National Institute on Drug Abuse [NIDA], 2021). Heroin, prescription pain relievers, and synthetic opioids, Bureau of Justice Assistance (BJA) Comprehensive Opioid, Stimulant, and Substance Abuse Program (COSSAP) like fentanyl, have contributed to this epidemic. The New York State Department of Health 2019 Annual Report