Transcription
Maggi et al. BMC Infectious Diseases (2017) 17:551DOI 10.1186/s12879-017-2626-zREVIEWOpen AccessCardiovascular risk and dyslipidemiaamong persons living with HIV: a reviewPaolo Maggi1*, Antonio Di Biagio2, Stefano Rusconi3, Stefania Cicalini4, Maurizio D’Abbraccio5, Gabriella d’Ettorre6,Canio Martinelli7, Giuseppe Nunnari8, Laura Sighinolfi9, Vincenzo Spagnuolo10 and Nicola Squillace11AbstractBackground: Aim of this review is to focus the attention on people living with HIV infection at risk of developing acardiovascular event. What is or what would be the most suitable antiretroviral therapy? Which statin or fibrate toreduce the risk? How to influence behavior and lifestyles?Discussion: Prevention of cardiovascular disease (CVD) risk remains the first and essential step in a medical interventionon these patients. The lifestyle modification, including smoking cessation, increased physical activity, weight reduction,and the education on healthy dietary practices are the main instruments.Statins are the cornerstone for the treatment of hypercholesterolemia. They have been shown to slow the progression orpromote regression of coronary plaque, and could also exert an anti-inflammatory and immunomodulatory effect.However the current guidelines for the use of these drugs in general population are dissimilar, with important differencesbetween American and European ones. The debate between American and European guidelines is still open and, alsoconsidering the independent risk factor represented by HIV, specific guidelines are warranted.Ezetimibe reduces the intestinal absorption of cholesterol. It is effective alone or in combination with rosuvastatin. It doesnot modify plasmatic concentrations of antiretrovirals. A number of experimental new classes of drugs for the treatmentof hypercholesterolemia are being studied.Fibrates represent the first choice for treatment of hypertriglyceridemia, however, the renal toxicity of fibrates and statinsshould be considered.Omega 3 fatty acids have a good safety profile, but their efficacy is limited. Another concern is the high dose needed.Other drugs are acipimox and tesamorelin.Current antiretroviral therapies are less toxic and more effective than regimens used in the early years. Lipodistrophy anddyslipidemia are the main causes of long-term toxicities. Not all antiretrovirals have similar toxicities. Protease Inhibitorsmay cause dyslipidemia and lipodystrophy, while integrase inhibitors have a minimal impact on lipids profile, and noevidence of lipodystrophy. There is still much to be written with the introduction of new drugs in clinical practice.Conclusions: Cardiovascular risk among HIV infected patients, interventions on behavior and lifestyles, use of drugs toreduce the risk, and switch in antiretroviral therapy, remain nowadays major issues in the management of HIV-infectedpatients.Keywords: HIV, Cardiovascular risk, Statins, Ezetimibe, Fibrates, Omega 3 fatty acids ART, Lipodystrophy, Dyslipidemia* Correspondence: p maggi@yahoo.com1Clinica Malattie Infettive Policlinico, Bari, ItalyFull list of author information is available at the end of the article The Author(s). 2017 Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, andreproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link tothe Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication o/1.0/) applies to the data made available in this article, unless otherwise stated.
Maggi et al. BMC Infectious Diseases (2017) 17:551BackgroundIn the recent years we observed an improvement of survival and quality of life in people living with HIV(PLWHIV), due to the success of combined antiretroviral treatment (cART) [1].The early treatment, the reduced toxicity of antiretroviral regimens and the fading of thymidine-analoguesbased regimens and the high dosage of ritonavir representless atherogenic antiretroviral agents for most PLWHIV.This is not enough since PLWHIV live longer, thus inaddition to age they add up all degenerative diseasescaused by HIV and the side effects of antiretroviral drugs.This should encourage physicians and researchers inseeking the patient’s well-being, not only throughHIV-RNA suppression, but thinking about other moreambitious goals, perhaps more distant from infectiousdiseases.Aim of this review is to focus the attention onPLWHIV at risk of developing a cardiovascular event.What is the most suitable cART? Which statin or fibrateto use in order to reduce the risk? How to influence behavior and lifestyles? Everything in the coming years willbe played in this field, so we must be prepared.Prevention of cardiovascular eventsAn inappropriate lifestyle, in particular smoking, reduced exercise, unhealthy diet and psychosocial stressare responsible for an increased CVD risk. The “lifestyle”is generally based on established patterns of behaviourover time, which have been internalized from childhoodand adolescence through the interaction of genetic andenvironmental factors and that are maintained or evenencouraged by the social context in adulthood age.The dietary habits and physical activity in particularare key factors for the reduction of CV diseases: risk factors such as alcohol use, high blood pressure, high bodymass index, hypercholesterolemia, diabetes, low fruitand vegetable intake and physical inactivity, collectivelyaccount, with smoking, for more than 60% of cardiovascular deaths globally [2]. Energy intake should be limitedto the amount of energy needed to maintain (or obtain)a healthy weight, that is a BMI 20.0 but 25.0 kg/m2.The wide variety of foods of animal and vegetable origin is the basis for a healthy and balanced diet. Manypublished data show that the Mediterranean diet appearsto be protective against cardiovascular disease and totalmortality. The use of this type of diet can have beneficialeffects not only on prevention of the main CVD risk factors but also on the course of the disease once it presented. The recommendations of the Mediterranean dietare reasumed in Table 1.Smoking remains the main responsible for the majorityof CVD [3]. The 10-year fatal CVD risk is approximatelyPage 2 of 17Table 1 Main recommendations of the Mediterranean diet [127–131]Increase the consumption of fresh fruit and vegetables of all kindsIncrease the consumption of legumes such as beans, peas, chickpeasand lentilsEat fish two or three times a weekEncourage the use of extra-virgin olive oil and sunflower and maize oilsLimit the consumption of animal saturated fat acids such as butter, lardand creamdoubled in smokers. The RR in smokers 50 years of ageis five-fold higher than in non-smokers [4].Preventing PLWHIV from starting smoking is critical,because stop smoking remains a formidable challenge. Although the percentage of smokers is declining in Europe,it still remains high and is rising in women, including adolescents and people socially disadvantaged [5]. Wideningeducation-related inequalities in smoking cessation rateshave been observed in many European countries. Therisks associated with smoking show a dose-response relationship with no lower limit for deleterious effects [4].Duration also plays a role, and while cigarette smoking isthe most common, all types of smoked tobacco, includinglow-tar (‘mild’ or ‘light’) cigarettes, filtered cigarettes, cigars and pipes, are harmful [6]. There is no age limit tothe benefits of smoking cessation.Some studies have investigated how much the increasedmortality in PLWHIV was attributable to smoking. In2013, a Danish study [7] observed that the cohort ofPLWHIV who smoked had an increased risk of deathfrom causes non-AIDS related at least four times higher.A more recent analysis of the same cohort [8] shows thatamong HIV people who have never smoked the risk ofheart attack is similar to that of HIV-uninfected subjects;in contrast, among the HIV active smokers the risk wasthree times larger than that observed in HIV negativesmokers. The Danish data can be reproduced in the HIVpopulation of Western Europe who started an antiretroviral treatment. Researchers in the ART Cohort Collaboration [9] analyzed all living patients in antiretroviraltherapy by at least one year, for whom data on smokinghabits were available between January 1999 and December2008. However, they excluded the intravenous drug usersbecause in these subjects the habit of smoking is widespread and mortality rates are higher than the rest of theHIV population. The analysis took into account 17,995 individuals for a total follow-up of 79,760 person-years. Ofthese 60% were smokers. According to the results, themortality rate due to all causes was 7.9 (CI 95%: 7.2 to8.79) per 1000 person-years among smokers and 4.2 (CI95%: 3.5 to 5.0) among non-smokers.Finally, it as to be remembered that some ways inwhich people cope with stress such as drinking, smokingor overeating, are not healthy especially in PLWHIV.
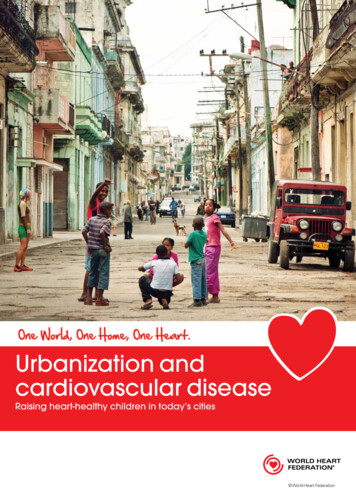
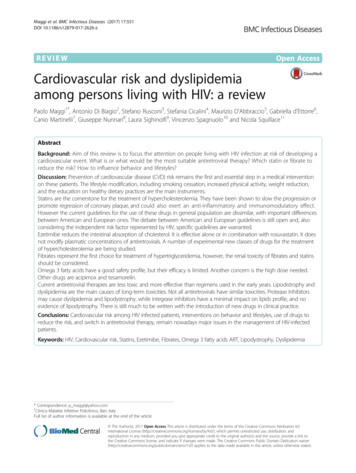
Maggi et al. BMC Infectious Diseases (2017) 17:551Combination antiretroviral therapy (cART)switchingGeneral principlesSwitching from current cART to a more lipid-friendlyregimen may represent an option to improve dyslipidemia and to reduce cardiovascular risk in PLWHIV. Theprinciples of cART switching also in the setting of dyslipidemia are to maintain virologic suppression, improveadherence and tolerability [10, 11]. Regimen or singledrug substitution may be done carefully and based onthe review of different patterns: a) individual factorscontributing to dyslipidemia; b) complete clinical andcART regimens history; c) virologic responses to previous cART regimens; d) historical genotypic resistancetest; e) adherence history; f ) previous cART associatedtoxicities. Besides, influence of current cART regimenon lipids profile could be evaluated. Clinical trial data onnaïve patients demonstrated that differences antiretroviral classes influence lipid values, even if there is heterogeneity among agents within every class: ritonavir(RTV) has been shown to significantly increase plasmalipid levels, in particular lopinavir/ritonavir (LPV/r) andfosamprenavir/ritonavir (FPV/r), to lesser extent withatazanavir/ritonavir (ATV/r) [12, 13].At the CROI 2017, much attention was centered on theD.A.D, findings on darunavir (DRV) in regards to the development of cardiovascular events. Their analysis hadbeen based on 7 years of follow-up and linked the cumulative use of DRV/r to a gradually increasing risk of CVD[14]. CVD incidence with cumulative DRV was similar tothat seen with old-times PIs indinavir and LPV/r. Authorsdid not show any clear explanation yet, after indicatingthat abnormal lipids did not modify the CVD risk withDRV/r, and did not provide any distinction between subjects treated with DRV/r BID versus QD.In the class of nucleoside/nucleotide reverse transcriptase inhibitors (NRTIs), dyslipidemia has been associatedwith exposure to stavudine, zidovudine and abacavir,whereas tenofovir disoproxil fumarate (TDF) has beennoted to have a favourable lipid influence [15, 16]. In theNNRTIs class, efavirenz has been associated with increases in total cholesterol and triglycerides, whereas rilpivirine has been shown to have less effect on lipidparameters than efavirenz [17]. Data on etravirine (ETR)are limited [18]. The integrase inhibitors (INIs) have a little effect on lipid profile [19–21], as well as C-C chemokine receptor type 5 (CCR5) inhibitor (maraviroc) [22].Since each cART switching has a potential virologic failurerisk, it is recommended to prefer regimens that are supported by clinical trials, switch studies or observational cohort studies. The potential options to appropriately switchcART agents are listed below:Switching within NRTIs: there is evidence of improvement of total cholesterol (TC), LDL-C and TGL switchingPage 3 of 17from abacavir (ABC)/lamivudine to TDF/emtricitabine(FTC) [23, 24].Switching from protease inhibitor boosted (PI/r) toNNRTIs: Most data on effect of switching from PI/r tonevirapine or efavirenz derived from the early cART era[25, 26]. In the recent years, the randomized SPIRITstudy, switching from PI/r to rilpivirine (RPV) has beenassociated with improved lipid parameters and 10-yearFramingham score [27]. In the ETRASWITCH study theswitch from PI/b to ETR showed a significant reductionin total cholesterol, TGL and glycemia [28].Switching from PI unboosted to NNRTI: in a most recent observational trials switch from unboosted PI toRPV has been associated with significant improved oflipids parameters [29].Switching from PI/r to an INSTI: Switching studiesfrom PI/r to raltegravir (RAL) (SWITCHMRK andSPIRAL) demonstrated a significant lipid and cardiovascular biomarkers reduction in RAL arm. However, in theSWITCHMRK study it was noticed an increased risk ofvirologic failure that was probably linked to a bias in thepatient’s selection [30, 31]. In the open-label STRATEGYstudy, including nearly 433 participants on first- orsecond-line treatment regimens with no previous virologic failure, were randomly assigned (2:1) to switch toelvitegravir/cobicistat (EVG/COBI)/FTC/TDF or continue stable PI/r regimens. At week 48, gastrointestinalsymptoms improved in the group switched to EVG/COBI/FTC/TDF. Moreover, the INI based regimens ledto significant decreases in total cholesterol, triglyceridesand HDL-c in LPV/r switches, decrease in triglyceridesin ATV/r switches and increase in HDL-c in darunavirswitches [32].Switch strategies in antiretroviral therapy in themanagement of dyslipidemiaAntiretroviral therapy suppresses viral replication andreduces the concentration of systemic immune activation markers [33, 34] and several studies reported the influence of therapy modification on biomarkers of CVD(Table 2). On the other hand, multiple evidences suggestthat some antiretrovirals such as the class of PI and theNRTI abacavir can contribute to the increased cardiovascular risk observed among HIV infected subjects[35]. Protease inhibitors are associated to higher rates ofdyslipidemia and increase of intima-media thickness[12]. ABC has been initially reported to increase the riskof myocardial infarction by data coming from the D:A:Din 2008 [36]. The supposed mechanism is that this drugcan be associated to endothelial disfunction and/or increased platelets activation. Subsequent reports from theD:A:D study highlighted that abacavir might represent arisk factor especially for patients presenting other preexisting cardiovascular risk factors, but further analyses
86 patients were included and74 patients (39 RAL, 35 PI/r)completed the substudy.SPIRAL-LIPsubstudyTo compare 48-week changes inbody fat distribution and bonemineral density (BMD) - usingDual-energy X-ray absorptiometryand computed tomographyscans - between patients switching81 (41 PI/r and 40 raltegravir)patients were evaluatedSPIRAL Substudy LDL subclasses and lipoproteinLDLphospholipase A2 activity insuppressed HIV-infected patientsswitching to raltegravir484848timeendpointevauationCT-scan:TAT (cm2) SAT (cm2) 48SAT (%) VAT (cm2) VAT (%)SAT/VATSAT, subcutaneousadipose tissue; TAT, totaladipose tissue; VAT, visceraladipose tissueTotal cholesterol, LDL-c,48HDL-c,Triglycerides, TC/HDL-c,Non-HDL-c, Apo A-I, ApoB, ApoA-I/Apo B LipoproteinPCSK9,LDL size, Cholesterolcontent in sdLDLLDLphenotype A, LDL phenotypeintermediate, LDL phenotypeB, Lp-PLA2 Total LDL-Lp-PLA2Total HDL-Lp-PLA2 8 (4; 14.9)8.7 (5.4; 17.2) 0.829Insulin,C-Peptide, HOMA indexhsCRP MCP-1 OPG IL-6 IL10 TNF-a ICAM-1 VCAM-1Selectin E SelectinP Adiponectin InsulinD-dimerOf 273 patients initiating studydrugs in the SPIRAL trial, 233(119 RAL, 114 PI/r) remained onallocated therapy for 48 weeksand had sera available for thepurpose of this substudyFasting serum cholesterol;fasting serum HDL-C;fasting serum LDL-C;fasting serum triglyceride;CD4 cell count; HIV RNA;SPIRAL Substudy Changes in cardiovascular biomarkersin HIV-infectedpatients switchingfrom ritonavir-boostedproteaseinhibitors to raltegravirMulticenter randomised open-labeltrial investigating the non inferiorityof switching to co-formuatedelvitegravir in patients virologicallysuppressed on a PI based regimenSTRATEGY PI439 patients. 266 out of 291participants randomized to theswitch group completed thestudy. 119 out of 143 participantsassigned to the no-switch groupcompleted the studyMarkers evaluatedFasting serum COL; fastingserum HDL-C; fasting serumLDL-C; fasting serum TG;CD4 cell count; HIV RNA;Randomized, open label switch studylooking at the non inferiority ofswitching patients who werevirologically suppressed on anNNRTI based regimen to coformulated elvitegravirSTRATEGYNNRTIEnrolled patients433 patients. 293 were includedin the group switching to coformulated elvitegravir and 140remained on their existingregimenStudy DesignStudy AcronymTable 2 Switch studies reporting the influence of therapy modification on biomarkers of cardiovascular diseaseSignificant increases in median VAT and TATwere seen within the PI/r group.No significantchanges in body fat were seen with RAL orbetween treatment groups.TC, LDL-c, non-HDL-c, TC/HDL, triglyceride,Apo B, Apo A-I and Lp (a) decreased inraltegravir arm compared to PI/r arm. A shiftfrom LDL phenotype B to the less atherogenicphenotype A was observed only in raltegravirarm.hsCRP (40%, P 0.0001), MCP-1 (20%,P¼0.0003), osteoprotegerin (13%, P¼0.0024),IL-6 (46%,P 0.0001), TNF-a (27%, P¼0.0011),insulin (26%, P 0.0001), and D-dimer (8%,P¼0.0187) decreased in RAL relative to PI/rgroup, whereas IL-10 (þ1%, P¼0.7773), ICAM-1(6%, P¼0.1255), VCAM-1(0%, P¼0.8671),E-selectin (9%, P¼0.2174), P-selectin (6%,P¼0.3865), and adiponectin (þ8%, P¼0.2028)remained unchangedAt week 48 3.8% of patients enrolled inthe switch arm abd 87.1% of participantsin the no-switch arm maintained a plasmaHIV RNA 50 copies/ml. Starting at week4 a stable non progressive increase in serumcreatinine occurred among switch armparticipants. A decrease in serum triglycerideswas observed in the switch group.At week 48 93% of participants in theswitch group and 88% in the no-switchgroup maintained plasma viral load 50copies/ml. No emergent resistances wereobserved among the two groups. Startingat week 4 increases of serum creatininewere observed among the switch group;increase was stable and non progressivethrough week 48. A small decrease inHDL-C was observed in the switch group.Laboratory markers change[34][31][34][32][32]referenceMaggi et al. BMC Infectious Diseases (2017) 17:551Page 4 of 17
multi-centric retrospective study wasconducted including HIV-1-positivepatients on raltegravir/nevirapinedualregimensrandomized open label,non inferioritytrialnaSTRIIVING551 patients on aintegraseinhibitors pr protease inhibitoror nonucleoside reversetrascriptase inhibitor regimenswith HIV-RNA 50 copie/mLwere included77 patients switching fromsuccessful regimensWe retrospectively identified from our39 patientselectronic database all patients withHIV RNA 50 copies/ml for 6 monthson an NVP-containing regimen and noprior exposure to integrase strandtransfer inhibitors who were switched toRAL plus NVP.na164 participants in the ANRS138trialTo compare the effect of randomlyswitching virologically suppressed,treatment-experienced patient fromenfuvirtide to raltegravir on biomarkerlevelsANRS 138Substudyfrom a ritonavir-boosted proteaseinhibitor (PI/r) to raltegravir (RAL)and patients continuing with PI/r.48,9624, 48, 7224, 48TC, HDL-C, LDL C, TG,TC/ratio; 24hs-PCR,sCD1s,sCD163, IL-6,D-dimer, sVCAM, I-FABProutine biochemical testsTotal cholesterol, HDLcholesterol,LDL-cholesterol,Total cholesterol/HDLratio,triglyceridesIL-6 hsCRP Level D-dimerTable 2 Switch studies reporting the influence of therapy modification on biomarkers of cardiovascular disease (Continued)[133][132]Significant declines of the levels of I-FABPand sCD14 was observed at 24 weeks[135]In patients switching with lipid abnormalities[134][n 52; 19 (36.5%) on statins, 3 on fibrates(5.7%), 4 on omega-3 fatty acids (7.7%)]triglycerides showed a significant decreaseboth at 48 and 96 weeks ( 83 mg/dL withp 0.004 and 51 mg/dL with p 0.011,respectively), while total and LDL-cl wereunchanged (p 0.11 and p 0.12, respectively).Median changes in serum lipids showedsignificant improvement at M6 for allparemeters except low-density lipoproteincholesterol in the whole population but lipidimprovement was greater in the PI/r groupAt week 24, a significant decrease frombaseline was observed in the IS arm,compared with the DS arm, for IL-6 level( 30% vs 10%; P .002), hsCRP level( 46% vs 15%; P .0001), and D-dimerlevel ( 40% vs 6%; P .0001). At week 48,there was a reproducible decrease in levelsof all biomarkers in the DS armMaggi et al. BMC Infectious Diseases (2017) 17:551Page 5 of 17
Maggi et al. BMC Infectious Diseases (2017) 17:551Page 6 of 17from the Food and Drugs Administration did not linkABC to increased frequencies of cardiovascular episodes,thus did not lead to restrictions in the prescription anduse of ABC [37]. Several trials have shown a beneficialeffect of switching to a NNRTI-containing antiretroviralregimen, as it is shown in Table 3.and triglycerides) should be assessed within 3 monthsafter the change and every 3 months during the firstyear. In absence of new complaints, subsequent monitoring should be performed on a regularly scheduledbasis [10, 11].Monitoring after switching cART regimenNew antiretroviral drugs and cardiovascular riskTenofovir AlefenamideDuring the first 3 months after the switch, the patientshould be closely monitored to assess tolerability andadherence to new cART regimen.HIV-RNA test may be performed to check for rebound viremia 4 weeks after the switch and then every3 months during the first year; fasting lipids (cholesterolTenofovir alafenamide (TAF) is a novel prodrug of tenofovir disiproxil fumarate (TDF). In this new formulationsTAF show higher levels of TDF-DP in periphereal bloodmononuclear cells and lymphoid tissues than TDF. TAFshowed safety advantages compared to TDF containingregimen regarding bone and renal toxicity [38], regardingTable 3 Trials on the therapeutic switch to a NNRTI-containing regimenStudy AcronymStudy Design and Enrolled PatientsMarkers evaluated time endpoint Laboratory markers changeevauationRefLIPNEFAA subset (n. 90) of virologically(a subset of NEFA) suppressed HIV-infected patientsenrolled in the NEFA study [98]enrolled in the NEFA study wereanalyzed for the HDL-C and LDL-C levels in the metabolic andbody-composition substudyLIPNEFA .HDL-C and LDL-Clevels24At 24 months, efavirenz (EFV) and nevirapine(NVP) produced similar lipid benefits: HDL-Clevels increased [EFV, 15% (p 0.001); NVP,21% (p 0.001)] and TC to HDL-C ratiosdecreased [EFV, 14% (p 0.001); NVP, 19%(p 0.01)].[25]SPIRITVirologically suppressed HIVinfected adults who werereceiving a PI-based HAARTwere switched to emtricitabinerilpivirine-tenofovir difumarate(FTC-RPV-TDF).TC, LDL-C, TGL,and TC:HDL-Cratio.24At 24 weeks, levels of TC, LDL-C, TGL, and theTC:HDL-C ratio had improved significantly inpatients switched to FTC-RPV-TDF comparedto those patients who kept their original PIbased treatment (p 0.001). Nevertheless,HDL-C levels declined significantly less withthe PI-based regimen (p 0.001).[17]Study 111Virologically suppressed patientswho were switched from EFVTDF- FTC to RPV-TDF-FTC.Fasting TC, LDL-C, 12, 48HDL-C, TGL, andTC:HDL-C ratio.A significative decline in fasting TC, LDL-C and [136]TGL at 12 weeks into the protocol. Results atweek 48 remained in the same direction(p 0.016), although changes from baseline inHDL-C and the TC:HDL-C ratio were notsignificant. The introduction of RPV in theclinical arena has been very positive for thepatients care, but we all have to rememberthe risk of a prolongation of QT interval withhigher doses of this compound (i.e. 75 and300 mg QD) as seen in the early phases ofclinical development.EtraswitchThe switch from a PI-containingregimen to etravirine (ETR) inpatients with therapeutic success.Glycemia, fastingTC, LDL-C, HDL-C,TGL, and TC:HDLC ratio.24The group of patients who received ETRshowed a significant reduction in TC(p 0.001), TGL (p 0.001), and glycemia(p 0.03). The 2 groups differed significantlyin TGL and glycemia at week 24. The greatestimprovement in all lipids was seen in patientswho switched from lopinavir/ritonavir to ETR.[28]naA prospective, open-label, 12-weekFasting TC, LDL-C, 12study of HIV-infected patientsHDL-C, TGL, andreceiving either a on bPI or EFV,TC:HDL-C ratio.and statin treatment. Four weeksafter statin interruption, bPI or EFVwas switched to ETR (400 mg for 8weeks) if serum low-density lipoproteincholesterol (LDL-C) was 3 mM. Theprimary endpoint was the proportionof patients not qualifying for statintreatment 8 weeks after the ETR switch.After 8 weeks of ETR treatment, 15 patients(56%) on ETR did not qualify for statintreatment. After the ETR switch, serum levelsof the cardiovascular biomarkers sICAM andMCP1/CCL2 decreased by 11.2% and 18.9%,respectively, and those of CCL5/RANTES andtissue inhibitor of metalloproteinase-1increased by 14.3% and 13.4%, respectively,indicating reduced cardiovascular risk.[137]
Maggi et al. BMC Infectious Diseases (2017) 17:551the lipid profile, increase from baseline in fasting totalcholesterol, LDL cholesterol, HDL and triglycerides wereobserved in TAF than with TDF. TAF has no “statin-like”phenomenon which characterized TDF. Long-term dataare not know.CabotegravirCabotegravir is an investigational HIV INI drug, currently being studied in Phase IIb clinical trials. Duringpreliminary studies conducted on healthy subjects bothin monotherapy and in combination with RPV [39, 40]no consistent, clinically significant, or dose-relatedchanges in haematology, clinical chemistry, vital signs,or ECG abnormalities or trends were observed. Lou etal. [41], in a study that assessed its effect on cardiac repolarization in healthy subjects, demonstrated that cabotegravir at a supratherapeutic dose had no effect oncardiac repolarization. In a fase IIa study, Spreen et al.[42] described two cases of laboratory abnormalities inHIV-1 infected patients in Cabotegravir monotherapyarm. A subject with type I diabetes had grade 2 hyperglycemia at baseline and at all time points other thanday 7 (hypoglycemia) and the follow-up visit (grade 3hyperglycemia). The other subject, on day 7, had grade 4TGL elevation subsequent to a very high–fat meal theprevious evening, and TGL were within normal limits atall other readings. Even the phase IIb studies, LATTEand LATTE-2 (still ongoing), underlined the good safetyprofile of cabotegravir with no cases of ECG abnormalities or metabolic disorders [43].DoravirineDoravirine is a NNRTI currently being studied in PhaseIII clinical trials as both a single-drug tablet and as partof a fixed-dose combination tablet. In a preliminarystudy with single and multiple doses of doravirine inhealthy subjects, no serious adverse events were reported, and there were no consistent, clinically relevant,treatment-related effects of doravirine on vital signs orECGs. Overall, no clinically significant trends or signalswere observed in laboratory assessments, vital signs orECGs [44]. In a randomized, double-blind, placebocontrolled, short-term monotherapy study of doravirineShurmann et al. described no clinically significant abnormalities in vital signs, routine blood and urine chemistrypanels, haematology, ECGs, or physical or neurologicalexaminations in any participant [45]. Results of a phaseIIb clinical trial, presented by Gatell et al. at the 12thInternational Congress on HIV Drug Therapy being heldin Glasgow, showed that 6.8% of patients had an increase in total cholesterol and 6.3% an increase of LDLcholesterol [46].Page 7 of 17Pharmacological treatment of dyslipidemiaDrugs for the treatment of hypercholesterolemiaStatinsStatins are the cornerstone of the treatment of hypercholesterolemia. They reduce the synthesis of cholesterolin the liver by competitively inhibiting the hydroxy-3methylglutaryl coenzyme A (HMG-CoA) reductaseactivity. The reduction in intracellular cholesterol concentrations induces LDL receptor expression on thehepatocyte cell surface, which results in increased extraction of LDL-cholesterol (LDL-C) from the blood anda decreased concentration of circulating LDL-C andother lipoproteins including triglycerides-rich particles.A number of large-scale clinical trials have demonstrated that statins substantially reduce cardiovascular(CV) morbidity and mortality in both primary and secondary prevention [47, 48]. In the general population,each 1.0 mmol/L (39 mg/dl) reduction in LDL-C levelhas been significantly associated with a 10% reduction inall-cause mortality, largely reflecting significant reductions in deaths due to coronary heart disease [47].Meta-analyses of randomized controlled trials that focused on primary prevention, demonstrated that inpeople without established CV disease but with CV riskfactors, the use of statins was associated with significantly improved survival and large reductions in the riskof major CV events [48, 49]. Benefits of statin therapywere observed in nearly all subgroups, including personswith diabetes mellitus, men and women, and across agegroups.The most recent clinical trials suggested that the LDL-Clowering effect of statins between PLWHIV is similar tothat seen in the general population. Several randomizedstudies of hypercholesterolemic HIV-infected patientsshowed that LDL-C decreased by 15% to 35% in patientstaking statins as compared with placebo [50]. In a trial inwhich PLWHIV on protease inhibitors (PIs) were randomized to atorvastatin 10
tle effect on lipid profile [19-21], as well as C-C chemo-kine receptor type 5 (CCR5) inhibitor (maraviroc) [22]. Since each cARTswitching has a potential virologic failure risk, it is recommended to prefer regimens that are sup-ported by clinical trials, switch studies or observational co-hort studies. The potential options to appropriately .