Transcription
Rappahannock Rapidan Community ServicesProgram Committee MeetingFebruary 27, 2018 – 1:00 PM – Bradford Road OfficesAgenda1. Call to order: Donalda Lovelace, Chair2. Review of agenda for additions / deletions3. Presentation by SAARA-(Substance Abuse and Addiction Recovery Alliance)4. Other updates5. AdjournThe next Program Committee meeting will be March 27th at 1:00pm.
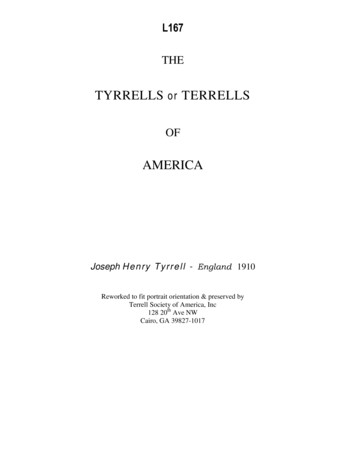
Certified peer recovery specialistsWhat is a Peer Recovery Specialist?A peer specialist is an individual with lived experience (either personally or as afamily member of an individual) with mental health, substance use, or traumarelated issues) who utilizes this experience to empower and support otherindividuals in recovery.What do Peer Specialists Do?Peer specialists foster hope for recovery by role modeling their own recovery tothe peers they serve. They do this by helping the peers identify their personalstrengths, uncovering community resources and supports, developing goals andsteps to achieve those goals, utilizing tools to support in recovery, and providingunconditional positive regard in individual and group atmospheres.Where do Peer Specialists Work?Peer specialists work in a variety of public and private environments, includinginpatient and outpatient mental health centers, in crisis centers and emergencyrooms, and with peer run organizations. Often they serve as an instrumental partof an individual’s treatment team.Why are Peers Important?To Qualify to Become a CPRS in Virginia, anindividual must:1.Have lived experience with mental health,substance use, or trauma related issues.2.Have 500 hours of supervised experience(paid or unpaid) providing Advocacy,Mentoring, Recovery/Wellness support,and/or Ethically Responsible Services toindividuals with mental health and/orsubstance use issues3.Have received 25 hours of llnesssupport,and/orEthically Responsible Services to individualswith mental health and/or substance useissues.4.Have earned a high school diploma or GEDcertificate.5.Have successfully completed a 72 hourDBHDS certified CPRS training course. Tolocate available trainings, visit the ertboard.org/cprs6.Take and pass the IC&RC Peer RecoverySpecialist Examination (following approvalof the CPRS application)7.Complete the Certified Peer hds.virginia.gov/library/recovery/vcb cprs application%20(2017).pdfPeer support services have been identified as an evidence-based model of carewhich has been demonstrated to reduce individual’s symptoms, improvecommitment to treatment goals, support peers’ overall quality of life, and lowerhealth care costs of these individuals.Are Peer Specialists the Same as Counselors?No, while both peer specialists and counselors work with individuals experiencingmental health and/or substance use issues with establishing and maintainingrecovery (often resulting in overlapping roles), their roles, knowledge, andexpertise are different. The major distinction between peers and counselors isthat peers self-identify as an individual with lived mental health and/orsubstance use, support other individuals in recovery through the reciprocity oftheir shared experience, and value the processing of learning together about theshared experience. Peer specialists do not deliver clinical interventions.Counselors, on the other hand, utilize their education and training to assessindividuals’ needs from a biopsychosocial perspective and deliver interventionsin a culturally appropriate manner. Although many counselors may have livedexperience with mental health and/or substance use issues, the focus of theirwork with individuals in recovery is not on their personal experience and insteadon the individual they are serving.Why Get Certified?The Certified Peer Recovery Specialist certification ensures that individuals havereceived the appropriate education, experience, supervision, and knowledge toperform their role as a peer specialist. As of July 1, 2017, Virginia Medicaid alsoapproved financial reimbursement for services delivered by a certified peerspecialist who is under appropriate supervision.
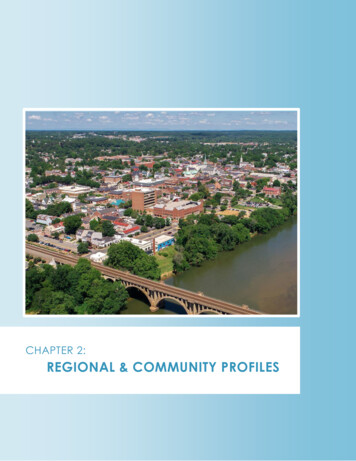
CERTIFIED PEER RECOVERY SPECIALIST (CPRS)CODE OF ETHICSPRINCIPLE 1: RECOVERY FIRSTPRINCIPLE 6: CONDUCTIn order to support others in recovery from mental healthand/or substance use issues, CPRSs must prioritize theirown recovery, ensuring that they seek additional outsidesupport in the event that they identify increasing mentalhealth and/or substance use issues in their own recovery.CPRSs must abide by appropriate boundaries with thosethey serve, including but not limited to representing self asa peer and limitations of which, refraining from use ofphysical force or intimidation, not excepting gifts ofsignificant value, not lending/borrowing from peers, notengaging in sexual relationships with peers (for at least twoyears following termination of working relationship), andnot providing services to individuals in which a previoussexual/intimate relationship existed.PRINCIPLE 2: SHARING PERSONAL RECOVERY STORYIn order to develop the reciprocity necessary for aneffective peer relationship, CPRSs must share their ownexperience with the goal of promoting resilience andrecovery.PRINCIPLE 3: SERVICE APPROACHWhile peers share a lived experience with mental healthand/or substance use issues, each person’s journey isunique. CPRSs must work to support others in their ownself-determined goals and perform advocacy based onthose identified goals.PRINCIPLE 4: CONFIDENTIALITYPRINCIPLE 7: INTEGRITYCPRSs must inform the peers they serve regardingdiscontinuation of services. When possible a referral forother services should be provided. In addition, CPRSs mustinform the appropriate individuals of any violation of theCPRS Code of Ethics by a CPRS.PRINCIPLE 8: CONFLICT OF INTERESTCPRS are unable to promote any treatment, procedure,product, or service for their own personal gain.Often a cornerstone of any helping relationship, CPRSsmust respect the privacy of those they serve whileoperating within the framework of applicable federal, state,local, and agency regulations.CPRSs cannot provide services outside of the scope of theirtraining.PRINCIPLE 5: NON-DISCRIMINATIONPRINCIPLE 10: PERSONAL DEVELOPMENTCPRSs provide support services regardless of an individual’scultural identity. Differences that exist with the potential toeffect the recovery process must be communicated withthe supervisor and referrals made as appropriate.CPRSs must continue to receive ongoing education,training, and supervision.PRINCIPLE 9: SCOPE OF PRACTICECONTINUING EDUCATION DOMAINSCertified Peer Recovery Specialists (CPRS) must complete a minimum of 20 hours of continuing educationevery two years, including a minimum of one hour in ethics. Understanding the Peer Support Role and Whatmakes it UniqueUnderstanding the Recovery ProcessMental Health and Addiction Recovery PathwaysCurrent Research in MH and SA RecoveryPeer Support Ethics and BoundariesBasic Principles Related to Health and Wellness Delivering Peer Services within Agencies andorganizationsTrauma and Its Impact on RecoveryCommunity Resource NavigationPeer Support Role in Crisis InterventionCultural Sensitivity and PracticeEmployment Support for Individuals in Recovery
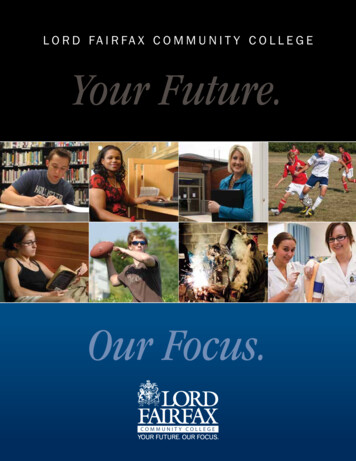
WHAT ARE PEER RECOVERY SUPPORT SERVICES?Peers SupportingRecoveryfrom SubstanceUse DisordersPeer recovery support services,1 delivered by peerrecovery coaches, are one form of peer support.They involve the process of giving and receivingnon-clinical assistance to support long-termrecovery from substance use disorders. A peerrecovery coach brings the lived experience ofrecovery, combined with training and supervision,to assist others in initiating and maintainingrecovery, helping to enhance the quality ofpersonal and family life in long-term recovery(White, 2009). Peer recovery support services cansupport or be an alternative to clinical treatmentfor substance use disorders.Peer-based recovery supports are part of anemerging transformation of systems and servicesaddressing substance use disorders. They areessential ingredients in developing a recoveryoriented system in which clinical treatmentplays an important, but singular, role. Acute caresubstance use treatment without other recoverysupports has often not been sufficient in helpingindividuals to maintain long-term recovery.Substance use disorders are currently understoodto be chronic conditions that require long-termmanagement, like diabetes. Peer-based recoverysupport provides a range of person-centered andstrength-based supports for long-term recoverymanagement. These supports help people inrecovery build recovery capital—the internaland external resources necessary to begin andmaintain recovery (Best & Laudet, 2010; Cloud &Granfield, 2008).WHAT DO PEER RECOVERY COACHES DO?“Peer support helped me seethat I was not hopeless. Itgave me my voice back andbolstered my self-worth.”—Michelle“When I needed someone towalk beside me, peer supportwas there.”—StevePeer recovery coaches walk side by side withindividuals seeking recovery from substance usedisorders. They help people to create their ownrecovery plans, and develop their own recoverypathways.Recovery coaches provide many different types ofsupport, includingemotional (empathy and concern)informational (connections to information andreferrals to community resources that supporthealth and wellness)instrumental (concrete supports such as housing or employment)affiliational support (connections to recoverycommunity supports, activities, and events)Recovery plans and other supports are customized,and build on each individual’s strengths, needs, andrecovery goals.1. Peer recovery support services, peer-delivered recovery support, andpeer-based recovery support are used interchangeably.Peer recovery support focuses on long-termrecovery and is rooted in a culture of hope, health,and wellness. The focus of long-term peer recoverysupport goes beyond the reduction or eliminationof symptoms to encompass self-actualization,community and civic engagement, and overallwellness.The unique relationship between the peer recoverycoach and the individual in or seeking recovery isgrounded in trust, and focused on providing theindividual with tools, resources, and support toachieve long-term recovery.Peer recovery coaches work in a range of settings,including recovery community centers, recoveryresidences, drug courts and other criminal justicesettings, hospital emergency departments, childwelfare agencies, homeless shelters, and behavioralhealth and primary care settings. In addition toproviding the range of support encompassed in thepeer recovery coach role, they take an active role inoutreach and engagement within these settings.
IS PEER RECOVERY COACHING EFFECTIVE?People who have worked with peer recoverycoaches provide strong testimonies of thepositive impacts of peer recovery support on theirown recovery journeys. The research supportsthese experiences. While the body of researchTwo rigorous systematic reviewsexamined the body of publishedresearch on the effectiveness of peerdelivered recovery supports publishedbetween 1995 and 2014. Both concludedthat there is a positive impact onparticipants (Bassuk, Hanson, Greene,Richard & Laudet, 2016; Reif et al, 2014) Taken as a whole, the current body ofresearch suggests that people receivingpeer recovery support may experience:is still growing, there is mounting evidence thatpeople receiving peer recovery coaching showreductions in substance use, improvements ona range or recovery outcomes, or both. Tworigorous systematic reviews examined the bodyImproved relationship withtreatment providers(Sanders et al., 1998; Andreas et al., 2010)of published research on the effectiveness of peerdelivered recovery supports published between1995 and 2014. Both concluded that there is apositive impact on participants (Bassuk, Hanson,Greene, Richard, & Laudet, 2016; Reif et al., 2014).Increased satisfaction with theoverall treatment experienceIncreased treatment retention(Armitage at al., 2010)(Mangrum, 2008; Deering et al., 2011;Tracy et al., 2011)Improved access tosocial supports(O’Connell, ND; Boisvert et al.,2008; Andreas et al., 2010)Decreasedemergency serviceutilization(Kamon & Turner, 2013)Reduced substance useReducedre-hospitalization rates(Min et al., 2007)(Bernstein, et al., 2005; Boyd et al.,2005; Kamon & Turner, 2013; Mangrum,2008; O’Connell, ND; Rowe, et al., 2007;Armitage at al., 2010)Decreased criminal justiceinvolvement(Rowe, et al., 2007; Mangrum, 2008)REFERENCESArmitage, E. V., Lyons, H., & Moore, T. L. (2010). RecoveryAssociation Project (RAP), Portland, Oregon. AlcoholismTreatment Quarterly, 28(3), 339–357.Bernstein, E., Bernstein, J., Tassiopoulos, K., Heeren, T.,Levenson, S., & Hingson, R. (2005). Brief motivationalintervention at a clinic visit reduces cocaine and heroin use.Drug and Alcohol Dependence, 77(1), 49–59.Boisvert, R. A., Martin, L. M., Grosek, M., & Claire, A. J. (2008).Effectiveness of a peer-support community in addictionrecovery: Participation as intervention. OccupationalTherapy International, 15(4), 205–220Greater housing stability(Ja et al., 2009)Reduced relapse rates(Boisvert et al., 2008)Boyd, M. R., Moneyham, L., Murdaugh, C., Phillips, K. D., Tavakoli, A.,Jackwon, K., . . . Vyavaharkar, M. (2005). A peer-based substance abuseintervention for HIV rural women: A pilot study. Archives of PsychiatricNursing, 19(1), 10–7.Ja, D. Y., Gee, M., Savolainen, J., Wu, S., & Forghani, S. (2009). PeersReaching Out Supporting Peers to Embrace Recovery (PROPSPER): Afinal evaluation report. San Francisco, CA: DYJ, Inc., for Walden House,Inc., and the Center for Substance Abuse Treatment, Substance Abuseand Mental Health Services Administration.Kamon, J., & Turner, W. (2013). Recovery coaching in recovery centers:What the initial data suggest: A brief report from the VermontRecovery Network. Montpelier, VT: Evidence-Based Solutions.Mangrum, L. (2008). Creating access to recovery through drug courts:Final evaluation report for the Texas Department of State Health Services.Austin, TX: University of Texas Addiction Research Institute. Retrievedfrom http://view.officeapps.live.com/op/view.aspx?src cMin, S. Y., Whitecraft, E., Rothbard, A. B., & Salzer, M. S. (2007). Peersupport for persons with co-occurring disorders and communitytenure: A survival analysis. Psychiatric Rehabilitation Journal, 30(3), 207–213. doi: 10.2975/30.3.2007.207.213O’Connell, M. J., Flanagan, E. H., Delphin-Rittmon, M. E., &Davidson, L. (2017). Enhancing outcomes for persons with cooccurring disorders through skills training and peer recoverysupport. Journal of Mental Health, Epub ahead of print. Retrievedfrom e, M., Bellamy, C., Baranoski, M., Wieland, M., O’Connell, M.J., Benedict, P., . . . Sells, D. (2007). A peer-support, groupintervention to reduce substance use and criminality amongpersons with severe mental illness. Psychiatric Services, 58(7),955–961.
Rappahannock Rapidan Community Services . Program Committee Meeting . February 27, 2018 - 1:00 PM - Bradford Road Offices . Agenda . 1. Call to order: Donalda Lovelace, Chair