Transcription
MEDICARE AND TECHNOLOGYA Guide to Medicare’sNew Remote PatientMonitoring ProgramHere’s how to implement this into your practice.By Josh White, DPM, CPedMultiple images Dreamstime.comThis article is written exclusivelyfor PM and appears courtesy of theAmerican Academy of Podiatric Practice Management. The AAPPM has aforty-plus year history of providing itsmember DPMs with practice management education and resources. Visitwww.aappm.org for more information.IntroductionThis article explains remote patient monitoring (RPM), how to implement it into podiatry practices,and reviews how well a trial workedfor a group of patients and practices. Remote patient monitoring is anew Medicare program that takesadvantage of advanced technology toimprove the way care for chronic disease is delivered. It offers podiatristsa way to leverage our role as expertsin lower extremity care and to stay atthe forefront of healthcare reform.Change in healthcare is being acwww.podiatrym.comcelerated by an unprecedented agingof our population. America is on theverge of a demographic tsunami thatis driving a transformation in our traditional fee-for-service approach tohealthcare. The percentage of the USed a strategic approach for healthcarepolicy for communities and organizations ever since.2 Goals of these principle are articulated as a “Triple Aim”: Improving the individual experience of care,Change in healthcare is being accelerated by anunprecedented aging of our population.population over 65 is to increase from13% in 2010 to 21% in 2050. Thenumber of people age 65 and over isexpected to more than double from40 million in 2010 to nearly 84 millionin 2050. 1 Recognizing the need forhealthcare reform, researchers at theInstitute for Healthcare Improvement(IHI) in 2008 developed an organizingprinciple that influenced the creationof Obamacare in 2010 and has provid- Improving the health of populations, Reducing the per capita costs ofcare for populations.The transformation of Medicare isdriving a focus on preventative care,particularly given the high percentage ofcosts associated with the treatment ofchronic disease. Remote patient monitoring is likely to help accelerate this change.Continued on page 66OCTOBER 2020 PODIATRY MANAGEMENT65
MEDICARE AND TECHNOLOGYRemote Monitoring (from page 65)66What Is Remote PatientMonitoring (RPM)?Remote patient monitoring is theuse of digital technologies to collectphysiological health data from patients in one location and electronically transmit that information securely to healthcare providers in adifferent location for assessment andrecommendations. RPM services include establishing, implementing,revising, and monitoring a specificpatient treatment plan related to achronic condition. RPM may be usedto promote patient self-care, monitorpatients’ key measures, and allowproviders and patients easy accessto information about patient healthissues.Remote patient monitoring aimsto allow more of physician office timeto be used for visits that require morecomplex intervention. Many RPMtechnologies have not had enoughreimbursement attached to them tomake financial sense for most physicians—until now. CMS is betting thataffordable new monitoring deviceswill help seniors stay in their homeslonger and out of the hospital. Suchan approach makes sense given therapid growth in Medicare and Medicaid spending, totaling almost 1.3trillion in 2017.3 RPM offers most podiatry practices the potential to earnover 100,000 additional annual revenue. While creating an entirely newrevenue stream for practices, it’s CMS’belief that preventing costly complications associated with chronic disease will result in a reduction of totalhealthcare costs.Considerations for Adopting RPMEffective remote patient monitoring programs target the right conditions, promote patient adherence todata collection, and ultimately directbehavior to prevent avoidable highcost healthcare use such as emergency room visits or hospitalizations. When considering remote patient monitoring, factors to considerinclude the program’s effectivenessat measuring and communicatingabout a physiological parameter, theease of workflow to implement intothe practice and lastly, how com-pelled patients will be to continueusing the program, in some instances, indefinitely.Bringing on RPM entails determination of the physiologic parameterthat makes the most sense for thepractice to monitor. The conditionmust be common in the practice andthe reason for monitoring must beaccepted by patients. The best devices will be the ones that are easy forpatients to use. Onboarding entailsinstructing patients how to use a device and obtaining their commitmentto working together to improve theirlong-term health. There also needs tobe commitment by the practice to en-cians to focus on providing in-personcare when most warranted.DevicesOnce a physician determineswhich parameter to measure, he/sheneeds to compare different devicesthat can be used. The primary considerations should be: Patient ease of use, The likelihood of patientcompliance, Accuracy of measurement, Cost to physician.Medicare doesn’t have specificrequirements for device-proven ac-Bringing on RPM entails determination ofthe physiologic parameter that makes the most sensefor the practice to monitor.sure that measurements are reviewedand patients communicated with tomake called-for changes.ParametersMeasure what matters. The firstconsideration in employing a remotepatient management program is deciding what to measure. The Medicare guidelines state that monitoring entails “physiologic parameter(s)(e.g., weight, blood pressure, pulseoximetry, respiratory flow rate)”. Theparameter must be within the practitioner’s scope of practice. There hasnot, as of yet, been more specificguidance beyond the provided examples as to what other conditionsMedicare considers acceptable.By 2050, half of all seniors arepredicted to be obese. These 42 million people will either have diabetesor, by definition, be pre-diabetic. At 43 billion per year, the cost of diabetic limb complications is moreexpensive than any form of cancer.4Remote monitoring technology existsthat can prevent ulceration, reducehealing time, and keep healed ulcers“in remission”. RPM offers the promise of fundamentally changing thecurrent approach to diabetic foot careby connecting patients to their risklevel in real time and allowing physi-OCTOBER 2020 PODIATRY MANAGEMENTcuracy or reliability, only that devices comply (though not necessarily be registered) as an FDA device.The FDA defines RPM equipmentas “wireless medical devices” thatutilize wireless radio-frequency (RF)communication (like Wi-Fi, Bluetooth, and cellular/mobile phonenetworks) to support the delivery ofhealthcare.”When comparing RPM devices,practitioners will discover that somedevices need to be plugged in, somecharged by patients every day, andsome don’t need to be charged atall. There are devices that last foryears while some have to be replacedevery few months. Some devicessend measurements via Bluetooth toa patient’s cellphone, and some to aprovided communication hub. Somedevices send information directly toa cloud platform via WiFi, some usecellular transmission.Medicare requires that the cost ofthe device be borne by the physician.Device cost should be taken into consideration with what RPM companies charge as a monthly fee. Somecompanies charge less for devices upfront and then bill more each monthfor as long as the patient is usingthe device; some devices are moreContinued on page 68www.podiatrym.com
MEDICARE AND TECHNOLOGYRemote Monitoring (from page 66)expensive but this is offset by lowermonthly fees.68Patient OnboardingPatient onboarding includes education about the parameters, the significance of monitoring it on a dailybasis and the mechanisms for makingadjustments when there is determination of what being monitored is out ofsorts. Onboarding can be done in thephysician’s office if the device is provided on-site; sometimes it’s done bythe device provider remotely if the device is shipped directly to the patient.Gaining patient trust to use RPMdepends largely on the provider’slevel of comfort with the technologyand his/her relationship with the patient. Providers need to understandhow to use the RPM device prior toencouraging its use. When patientssee providers struggling to use thetechnology, it can cause uncertaintyin patients about its value in the delivery of their care.The key to engaging patients withRPM is to make it easy. Devices workbest if they require little prior knowledge about technology, easily connectto patients’ smart phones or othercommunication devices, and seamlessly integrate into patients’ dailylives. Patients will be most receptiveto adopting RPM if the patient’s family members are included in the engagement/education process.Platform/DashboardThe RPM platform allows someone the physician employs, potentially off-site and possibly a contractedvendor, to manage patients througha single comprehensive dashboard.The dashboard should offer analytictools to report on and assess patientdata, and allow the physician to integrate reports into their EHR. Thedashboard should track the amountof time spent reviewing patient data,accessing other documents, and providing patient communication. HIPAAsecurity requires separate log-ins byindividuals accessing the platform.Communication StrategyNudge theory contends that indirect suggestions and positive re-inforcement can influence people’sactions. The simple act of being reminded, or “nudged,” to respond toreported measures on a consistent,unobtrusive basis can elicit positive health behaviors. While relevant patient-reported data captureand revenue enhancement are theprimary goals of an RPM program,an ancillary benefit is stronger pa-ers and business models to use thetechnology.CPT code 99453: Patient educationand set up“Remote monitoring of physiologic parameter(s) (e.g., weight, bloodpressure, pulse oximetry, respiratoryflow rate), initial; set-up and patienteducation on use of equipment.”The RPM platform allows someone thephysician employs, potentially off-site and possibly acontracted vendor, to manage patients througha single, comprehensive dashboard.tient engagement. Programs will bemost successful when patients havea single point of contact for technicaland clinical issues. It is through therelationship building that occurs withmonthly communication that patientsbecome willing to accept RPM as away to achieve better outcomes.Every RPM company must finetune its communication strategy tonot send too many alerts that arefalse positives nor miss significantfindings by creating false negatives.Too many warnings that are not trulyurgent risk patients becoming irritated and even worse, choosing to withdraw from the program. Too littlecommunication and patients mightfail to value the merit of their continued participation.Medicare Program OverviewRemote patient monitoring became covered by Medicare in January 2018. It’s significant that thenew CPT codes 99457 and 99458can be billed “incident to” andunder “general supervision” rather than “direct supervision”. General supervision means the servicecan be furnished under the billingpractitioner’s overall direction andcontrol, but the billing practitioneris not required to be physically present or even within the same officebuilding as the practice associateproviding the care. The “incident to”revision aims to expand RPM reimbursement by allowing more provid-OCTOBER 2020 PODIATRY MANAGEMENTCPT 99453 offers reimbursementfor the work associated with onboarding a new patient onto an RPMservice, setting up the equipment,and educating the patient on usingthe equipment. The 2020 nationalMedicare payment for these servicesis 18.77. Patient must opt-in for theservice Patient cannot be charged forthe device. Device must meet the FDA’sdefinition of medical device and capture physiological data. Physician must order the device. Anyone on staff can perform theset up and education. Monitoring must be for at least16 days. No RVUs, a technical code Documentation should be basedupon the provider’s clinical judgmentof the patient’s condition and include:– Nature and severity of condition– Detailed history of condition– Medical necessity and clear rationale for monitoring– Goals to be achieved by RPM CMS does not reference a faceto-face requirement associated withRPM, despite having previously imposed such a requirement for CPT99091. This omission supports theinterpretation that CMS does not intend to carry forward the consentand face-to face visit requirementsfor the new RPM codes.Continued on page 70www.podiatrym.com
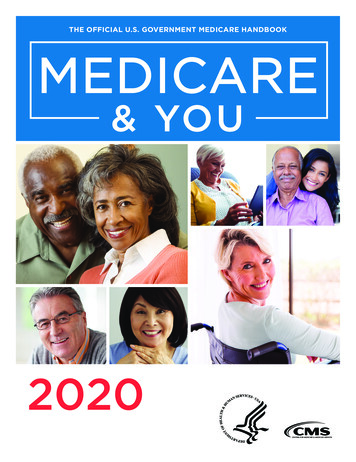
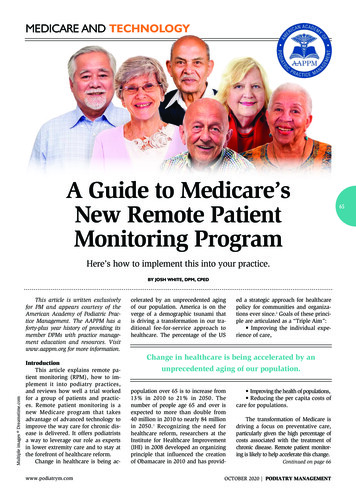
MEDICARE AND TECHNOLOGYRemote Monitoring (from page 68)70CPT code 99454: Device and transmission of data“Device(s) supply with daily recording(s) or programmed alert(s)transmission, each 30 days.”CPT 99454 offers reimbursement for providing the patient withan RPM device for a 30-day period.99454 can be billed each 30 days.The 2020 national Medicare paymentis 64.15. Device must be supplied for atleast 16 days to be applied to a billing period. The service must be ordered bya physician or other qualified healthcare professional. Data must be wirelessly syncedwhere it can be evaluated No RVUs May be used with either CPT99091 or 99457. There is no minimum numberof measurements that must be collected each day.CPT code 99457: Interpretation andManagement“Remote physiologic monitoring treatment management services,clinical staff/physician/other qualified health care professional time ina calendar month requiring interactive communication with the patient/caregiver during the month, first 20minutes.”CMS will reimburse for clinicalstaff time that contributes towardmonitoring and interactive communication which includes phone,text, and email. It’s significant thatin January 2020, Medicare changedthe rules to allow RPM services tobe delivered by auxiliary personnel who are not under direct supervision of the physician. Auxiliarypersonnel can be in a different location from the supervising physician.These changes permit technologyvendors and other third parties whohave not historically been involvedin the delivery of direct patient careto engage in RPM arrangements thatsupport physicians and other careproviders. The 2020 national Medicare payment for these services is 51.61. Report once each 30 days. Do not report in conjunctionwith CPT99091. Do not count any time on a daywhen the physician reports an evaluation/management service. May be billed as an “incidentto” service. Does not require live face-toface or voice communication.Services billed as “incident to”must be an integral, though incidental, part of the billing practitioner’s service in the course of thepatient’s diagnosis or treatment.This means the practitioner submitting the bill must furnish an initialservice (e.g., an E/M visit) to whichthe subsequent RPM services areintegral and incidental, establishingthe patient relationship prior to furnishing RPM. During the COVID-19Continued on page 71Table 1:Annual Revenue per Patient1st MonthMonth 2-12AnnualTotalSetup (99453) 19 19Equipment Data Transmission (99454) 62 62 744Viewing Data, Communicating with Patient—Initial 20 Minutes (99457) 52 52 624Viewing Data, Communicating with Patient—Additional 20 Minutes (99458) 42 42 252* 175 156 1,639Annual revenue opportunity of approximately 1,500 per year per patient, or higher***Assumes spending additional 20 minutes for 50% of monthly communication**Does not include cost of equipment or softwareOCTOBER 2020 PODIATRY MANAGEMENTwww.podiatrym.com
MEDICARE AND TECHNOLOGYRemote Monitoring (from page 70)crisis, E&M visits can be performedvia telehealth.CPT code 99458: Interpretation andManagement, additional 20 minutes“Add-on code for patients whoreceive an additional 20 minutes ofRPM services in a given month (i.e.,40 minutes of RPM services).”CPT 99458 allows for the physician or clinical staff, under generalsupervision, to provide, when thecomplexity of the patient’s conditionwarrants it, additional interactivecommunication beyond the initial 20minutes. The 2020 national Medicarepayment for these services is 42.22(each calendar month per patient).CPT code 99091: Collection and interpretation of physiologic data“Collection and interpretation ofphysiologic data (e.g., ECG, bloodpressure, glucose monitoring) digital-www.podiatrym.comly stored and/or transmitted by thepatient and/or caregiver to the physician or other qualified healthcareprofessional, qualified by education,training, licensure/regulation (whenapplicable) requiring a minimum of30 minutes of time, each 30 days.”When patients with chronic conditions are remotely monitored andthe physiological data indicates nothing abnormal and thus no modification of the care plan needed, it wouldbe appropriate to bill using chroniccare management code CPT 99091,“Data collection and interpretation”.CMS will reimburse for professional time dedicated to monitoringservices and does not require interactive communication like CPT 99457to bill. However, it requires the physician to perform these services, andrequires 30 minutes of time every 30days to bill. CPT 99457 and 99091cannot be billed concurrently. Theaverage 2020 Medicare payment forthese services is 59.19.How Podiatrists Can Implement RPMSelect ParameterPhysicians should focus on chronic conditions that they commonly seein their practice and that a plan ofcare would fall under their scope ofpractice. For most podiatrists, diabeticfoot ulceration is the chronic condition most frequently seen that can beimproved via on-going monitoring.The parameters that have been validated and that device manufacturers addressing DFUs have thus far focused on are foot temperature, plantarpressure, and patient adherence.Identify PatientsAs every state has a different Medicare carrier and because the programis so new, there are instances of somepayors not recognizing these newcodes. It’s expected that Medicare Advantage plans and private payors willbe soon coming on board and payingContinued on page 72OCTOBER 2020 PODIATRY MANAGEMENT71
MEDICARE AND TECHNOLOGYRemote Monitoring (from page 71)for RPM as well. Patients have to optin to remote patient monitoring programs and are responsible for applicableco-payments. It makes sense to workwith patients who are capable of working with new, easy-to-use technology,and who will be receptive to frequentreminders. It doesn’t pay to spend muchtime trying to convince patients to participate if they are not enthusiastic abouta program of self-care and demonstratea likelihood of dropping out.72Select DeviceCompanies will be competingbased on how easily they make it forpractices to onboard their patientsand how easy their devices are forpatients to use. The best devices willeasily integrate into patients’ routines, will be easy to keep charged,and will work with minimal hassle. Anumber of companies have recentlylaunched that offer a complimentaryapproach for improving diabetic footcare. They feature: Sensor impregnated socks thattrack foot temperature as a means ofdetecting impending ulceration, An innovative, adjustable bootthat tracks patient activity and patient compliance for healing plantarwounds, and Custom diabetic inserts thatincorporate sensors that measure foottemperature, pressure, and patientadherence.Develop Office ProtocolsPractices will potentially havehundreds of patients that they canenroll in remote patient monitoring.Focusing on the people implementingand using the technology, rather thanthe technology itself, will make all thedifference in developing a successfulprogram that incorporates a sustainable, new model of care.Your EHR should be used to flagpatients with the selected parameterand qualified payer. There should bea mechanism to remind clinicians topromote RPM to qualified patients, toeducate them about its benefits andobligations, and to get their consentto participate. Some devices can bestocked and dispensed that same day,some devices need to be individuallyordered. Some devices can be shippedto patients with patients on-boardedremotely; some programs require thepatients to return to the office.The practice must spend a minimum of 20 minutes communicatingwith each patient every 30 days in orderto bill Medicare. Twenty and sometimesforty minutes spent, per patient, permonth will become a substantial time Improved patient self-management Improved access to care Improved use of clinical resources Increased practice revenueImplementation is unfortunatelyfar more complicated than simplyproviding devices, collecting patientfoot information, and creating practice revenue. RPM success will beA successful RPM program has the potentialto improve the health of hundreds of patients ineach practice and creates an opportunityfor most offices to earn 100,000 or more.requirement for practices once hundreds of patients are enrolled. WhileMedicare reimbursement can easilycover the cost of office personnel doingthe monthly follow-up, many officeswill recognize the benefit of delegatingthis responsibility to an outside vendor.Develop MetricsYou cannot manage a program ifyou cannot measure it. A successfulRPM program has the potential toimprove the health of hundreds ofpatients in each practice and createsan opportunity for most offices toearn 100,000 or more (Table 1). Thephysician overseeing the programshould, on an ongoing basis, track: # Patients enrolled # Patients monitored # Patients dropping out Revenue collected Average time to heal ulceration Average time of re-ulcerationIt would also be valuable to doperiodic surveys to assess patient satisfaction and audits to ensure thatproper billing and documentationpractices are being followed.SummaryRemote patient monitoring is rapidly evolving and stands to become anincreasingly vital part of how podiatrists practice. Opportunities include: Reduction of diabetic footulceration Reduction of overall cost of careOCTOBER 2020 PODIATRY MANAGEMENTachieved by practices planning andstarting in a limited fashion, making adjustments along the way, andslowly and steadily enrolling patients. It would not be unrealistic tostart with a test group as small as5-10 patients to get a good understanding of issues that will be encountered. Once issues are identified and addressed, practices will bemuch better able to streamline protocols, improve patient outcomes andmake more money. PMReferencesPritzger, P, Gallagher P, 65 in theUnited States: 2010, U.S. Department ofCommerce issued 2014, pp 23-2014.2The Triple Aim: Care, Health, andCost. Berwick DM, Nolan TW, Whittington J, Health Aff (Millwood). 2008 MayJun; nationalhealthexpenddata/nhe-fact-sheet4American Diabetes Association, Boulton, Armstrong, D., ‘Diagnosis and Management of Diabetic Foot Complications’,2018.1Josh White, DPM,CPed is VP of OrthoFeetand the founder of SafeStep. He is a member ofthe American PodiatricMedical Association’sDME workgroup and aCodingline Expert Panelist. (Contact info: joshwhitedpm@gmail.com)www.podiatrym.com
OCTOBER 2020 PODIATRY MANAGEMENT www.podiatrym.com 68 MEDICARE AND teChNoLoGy ers and business models to use the technology. CPT code 99453: Patient education and set up "Remote monitoring of physiolog-ic parameter(s) (e.g., weight, blood pressure, pulse oximetry, respiratory flow rate), initial; set-up and patient education on use of .