Transcription
2019 ManagedLong-Term Care ReportDepartmentof Healthhealth.ny.gov
Table of ContentsPageExecutive Summary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .3Introduction. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .4The Managed Long-Term Care Program. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .5Types of Managed Long-Term Care Plans. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .5Eligibility. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .6Medicaid Redesign Team. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .6Enrollment and Availability . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .7Uniform Assessment System for New York . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .8Level of Care Score . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .8Table 1. Demographic Profile of MLTC Enrollees. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .9Table 2. Utilization and Patient Safety. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .10Table 3. Health Plan Profiles. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .11Enrollee Attributes. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .14Table 4. Overall Functioning and Activities of Daily Living . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .15Table 5. Continence, Neurological, and Behavioral Status. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .20Table 6. Living Arrangement and Emotional Status . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .23Plan Performance. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .26Current Plan Performance. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .26Table 7. Quality of Life, Effectiveness of Care, and Emergency Room Visits. . . . . . . . . . . . . . .27Table 8. Access and Experience of Care. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .32Performance Over Time. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .35Table 9. Functioning and Activities of Daily Living. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .36Table 10. Quality of Life and Effectiveness of Care . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .42Potentially Avoidable Hospitalizations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .45Table 11. Potentially Avoidable Hospitalizations. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .46Member Satisfaction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .47Satisfaction with the Experience of Care . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .47Table 12. Satisfaction with the Experience of Care. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .48Appendix A: Managed Long-Term Care Covered Services. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .53Appendix B: Region Definitions. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .54Appendix C: UAS-NY CHA Measure Descriptions. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .55Appendix D: Technical Notes. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .621
2
Executive Summary E ighty-five percent of enrollees had nobehavioral problems.New York State certifies and oversees the operationof New York State managed long-term care (MLTC)plans. This oversight includes evaluating quality ofcare delivered by MLTC plans. This report describesNew York State’s certified MLTC plans and presentsinformation about the quality of care they provideand enrollees’ satisfaction with the plans. The reportis organized into four sections: 1) MLTC programlevel information, 2) Plan level enrollee attributes,3) Plan level performance, and 4) Plan level membersatisfaction. Data sources and time frames for themeasures are described in the report. Thirty-four percent of enrollees were living alone.Plan PerformanceThe domains of quality performance in this reportinclude: 1) Current plan performance rates such asthe percentage of enrollees who received an annualflu shot, 2) Plan performance over time such asthe percentage of enrollees whose pain intensityremained stable or improved over time, and 3) Therate of potentially avoidable hospitalizations (PAH)per 10,000 days enrolled in the plan. The tablesinclude the plan-specific and statewide results andwhether the plan’s performance was statisticallyhigher, the same, or lower than the statewideaverage. The following are highlights:The Managed Long-Term Care ProgramTo keep chronically ill or disabled individualshealthy and living in the community, MLTC plansassist members who require health and long-termcare services. The benefit package includes a rangeof health and social services, including skillednursing facility (SNF) services. MLTC program levelhighlights include: Seventy-nine percent of enrollees receivedthe recommended annual influenza vaccination.Plan results ranged from 67 to 94 percent. Enrollment in the MLTC plans has been steadilyincreasing, with current enrollment of 274,271individuals as of November 2019. Ninety-six percent of enrollees had no fallsthat resulted in major or minor injury in thepast 90 days. Seventy-six percent of the membershipwas in New York City. Ninety percent of enrollees remained stableor demonstrated improvement in the activitiesof daily living function. Eighty-three percent of enrollees were overthe age of 64. Eighty-five percent of enrollees remained stableor demonstrated improvement inurinary continence. Eighty-five percent were dually enrolledin Medicare and Medicaid. The statewide rate of PAH was 2.76 andplan results ranged from 0 to 4.88 potentiallyavoidable hospitalizations per 10,000 daysenrolled in the plan. Eighty-one percent have been enrolled in theMLTC program for one year or more. Twelve percent of enrollees were admitted toa nursing home, and of that group 66 percentwere admitted for long-term placement.Member SatisfactionIn early 2019, the Department sponsored asatisfaction survey of MLTC enrollees who hadsix months of continuous enrollment in 2018.The overall response rate was 23 percent.The following are highlights: Twelve percent of enrollees were admittedto the hospital. The most common reason foradmission was respiratory problems. Six percent of enrollees visited an emergencyroom. The most common reason for a visit wasrespiratory problems. Eighty-nine percent of respondents ratedtheir health plan as good or excellent.Enrollee Attributes Eighty-six percent rated the helpfulnessof the plan in managing their illnessesas good or excellent. Thirty-two percent of enrollees were ableto transfer with little to no help.3
Introductionenrollment data for MLTC plans since 2012. This isthe eighth public report on MLTC performance. Theanalyses presented in this report provide the basisfor more data-driven improvement initiatives.The Long-Term Care Integration and Finance Act(Chapter 659 of the Laws of 1997) provides theCommissioner of Health with the authority to certifymanaged long-term care plans and oversee theiroperation, including the quality of care. In November2019, there were 35 MLTC organizations certifiedto enroll members in four plan types. Many MLTCorganizations are certified to enroll in more than oneplan type and are considered separate plans. Thecombination of MLTC organizations and plan typesresults in 51 plans. The tables in this report presentinformation about the MLTC organizations andplans that were enrolling members during the datacollection period.New York State Department of Health (NYSDOH)has been publishing quality performance andIf you have any questions or comments aboutthis report, please feel free to contact us at:Office of Quality and Patient SafetyCorning Tower Room 1938Empire State PlazaAlbany, New York 12237Phone: (518) 486-9012Fax: (518) 486-6098Email: MLTC OQPS@health.ny.gov4
The Managed Long-Term Care Programthe long-term care and select ancillary servicesdescribed in Appendix A. The enrollee’s ambulatorycare and inpatient services are paid by Medicareif they are dually eligible for both Medicaid andMedicare or by the Medicaid program if they arenot Medicare eligible. Partial capitation plans arerequired to coordinate all services for their members,including those that are not in the MLTC benefitpackage, such as visits to physicians and hospitaladmissions. The minimum age requirement is 18years. Partial capitation contracts must be approvedby the Centers for Medicare and Medicaid Services(CMS) and the NYSDOH. All partial capitation plansoperating in New York State receive a Certificateof Authority from the Department of Health.Managed long-term care (MLTC) plans assistchronically ill or disabled individuals who requirehealth and long-term care services. MLTC plansreceive a monthly risk-adjusted capitation paymentfrom the New York State Medicaid Program topay for a range of health and social services. Thebenefit package includes home care, personalcare, ancillary services, and transportation services.A list of covered services is included in Appendix A.Depending on the type of plan, ambulatory care,inpatient, and mental health services may alsobe included in the benefit package.Types of Managed Long-Term Care PlansWithin the MLTC program, there are four modelsof plans that are described below. All plans acceptMedicaid payment. Some plans also acceptMedicare or private payment for members whoare not eligible for Medicaid.Program of All-Inclusive Carefor the Elderly OrganizationsProgram of All-Inclusive Care for the Elderly (PACE)organizations provide a comprehensive systemof health care services for members age 55 andolder who are otherwise eligible for nursing homeadmission. Both Medicare and Medicaid pay forPartial CapitationA risk-adjusted Medicaid capitation paymentis provided to the plan to cover the costs of5
H ave a chronic illness or disability required foran individual to be eligible for services usuallyprovided in a nursing homePACE services on a capitated basis. PACE membersare required to use PACE physicians. An inter disciplinary team develops a care plan and providesongoing care management. The PACE plan isresponsible for directly providing or arranging allprimary, inpatient hospital, and long-term careservices required by a PACE member. The PACEorganization is approved by CMS and the NYSDOH.or A re expected to need long-term care servicesfor more than 120 days from the date ofenrollment.Medicaid Advantage PlusMedicaid Redesign TeamMedicaid Advantage Plus (MAP) plans must becertified by the NYSDOH as MLTC plans and by CMSas Medicare Advantage Plans. As with the PACEmodel, the plan receives a capitation payment fromboth Medicaid and Medicare. The Medicaid benefitpackage includes the services in Appendix A and alsocovers Medicare co-payments and deductibles. Theminimum age requirement is 18 years. All enrolleesmust be eligible for nursing home placement.In 2011, Governor Andrew Cuomo convened atask force consisting of policy experts and industryrepresentatives to collaborate on redesigningNew York State’s Medicaid program. The membersof the Medicaid Redesign Team (MRT) evaluatedthousands of proposals solicited from experts andthe public. Following a series of public meetings,the MRT voted on the proposals and 78 wereenacted in the 2011-2012 budget. More informationis available at: http://www.health.ny.gov/health care/medicaid/redesign/.MRT #90 required the mandatory transition andenrollment of certain community-based long-termcare services recipients into Managed Long-TermCare as a component of a fully integrated caremanagement system. In August 2012, the NYSDOHreceived written approval from CMS to beginmandatory enrollment in MLTC. This amendmentto the Partnership Plan Medicaid Section 1115Demonstration waiver required all dual-eligibleindividuals (persons in receipt of both Medicareand Medicaid benefits) ages 21 or older and in needof community-based long-term care services formore than 120 days to be mandatorily enrolledinto Managed Long-Term Care Plans. The transitionto MLTC was implemented in five phases endingin 2014. The following groups are excluded fromtransition to MLTC:Fully Integrated Duals AdvantageFully Integrated Duals Advantage (FIDA) plans areapproved by CMS and the NYSDOH. The planreceives a capitation payment from both Medicaidand Medicare and provides a comprehensive benefitpackage. The FIDA benefit package includes allMedicare physical health, behavioral health, andprescription drug services, as well as all Medicaidphysical health, behavioral health, and long-termsupport services. Some additional services andbenefits are also included. The minimum agerequirement is 21 years.EligibilityThe data in this report are representative of individ uals who have enrolled in one of the four typesof MLTC plans and have met the following criteria: Are able to stay safely at home at the timewhen joining the plan; Nursing Home Transition and Diversion Waiverparticipants; Meet the age requirement of the programand the plan; Traumatic Brain Injury Waiver participants; Assisted Living Program participants; Reside in the area served by the plan; Dual eligible individuals who do not requirecommunity-based long-term care services.and6
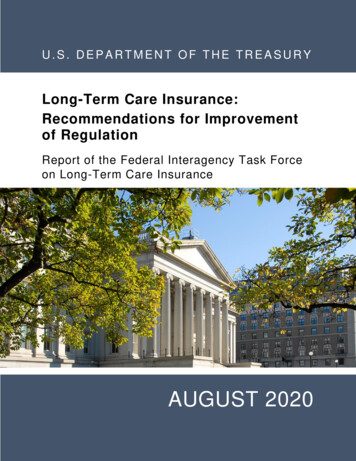
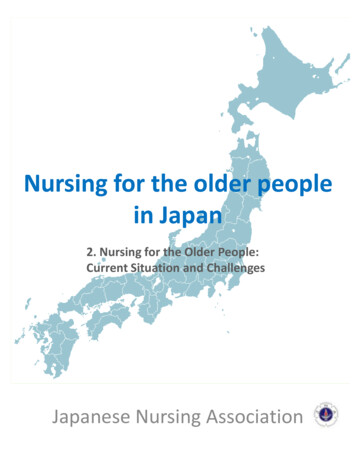
In 2015, New York State, in partnership with theCMS, began a MLTC FIDA demonstration projectin the New York City area. FIDA plans provide acomprehensive benefit package to MLTC enrolleesincluding Medicare covered services, Medicaidcovered services, and some additional servicesand benefits. Opt-in enrollment began in Januaryand passive enrollment occurred betweenApril and October 2015.10,000 in 2004 to over 274,271 as of November2019, with the number of plans growing from 16 plansto 51 plans. Ninety-one percent of the enrollment isin partial capitation plans and highly concentrated inNew York City, which accounts for 76 percent ofcurrent MLTC enrollment. Enrollment in MAP, PACE,and FIDA plans is 6, 2, and 1 percent, respectively.As shown in Figure 1, the increase in enrollment inMLTC has accelerated following the implementationof MRT #90.Every county in New York State has at least oneMLTC plan authorized to operate. As of November2019, MLTC has members enrolled in every county.Enrollment and AvailabilityFigure 1 shows that MLTC enrollment has steadilyincreased over the past 15 years from approximatelyFigure 1Managed Long-Term Care Enrollees by Location and Year300,000 Upstate NYC Total 00020042006200820102012Year72014201620182019
Uniform Assessment System for New Yorkdata remain critical to inform eligibility for the MLTCprogram, provide the basis for the MLTC plans’ caremanagement planning processes, and facilitate aplan’s identification of areas where the member’sstatus differs from optimal health or functional status.Submission of assessment data occurred twicea year with the SAAM instrument. Now, assessmentdata are submitted by plans to the UAS-NY electroni cally as assessments are conducted, and are addedto the database upon submission. Each year, MLTCUAS-NY CHA submissions will be used to create twostatic assessment files. One contains the most recentassessment for enrollees in each plan from Januarythrough June. The second contains the most recentassessment for enrollees in each plan from Julythrough December. These two files will be used todescribe and evaluate the MLTC plan performance.The MLTC plans are required to collect and reportto the NYSDOH information on enrollees’ levelsof functional and cognitive impairment, behaviors,and clinical diagnoses. This information is collectedat enrollment and then semi-annually thereafter.From 2005 through September 2013, these datawere collected using the Semi-Annual Assessmentof Members (SAAM) instrument, a modified versionof the Federal (Medicare) Outcome and AssessmentInformation Set (OASIS-B). The SAAM was usedto establish clinical eligibility for the MLTC programand assist health providers in care planning andoutcome monitoring.Beginning on October 1, 2013, the SAAMinstrument was replaced by the Uniform AssessmentSystem for New York (UAS-NY) Community HealthAssessment (CHA) instrument, which may includea Functional Supplement and/or Mental HealthSupplement. The UAS-NY is an electronic systembased on a uniform data set, which standardizesand automates needs assessments for home andcommunity-based programs in New York. TheUAS-NY is based on the interRAI suite of assessmentinstruments. interRAI is a collaborative networkof researchers in over 30 countries committed toimproving health care for persons who are elderly,frail, or disabled. Their goal is to promote evidencebased clinical practice and policy decisions throughthe collection and interpretation of high-quality data.The interRAI organization and its assessment toolsare used in many states as well as Canada andother countries. Using the UAS-NY facilitates accessto programs and services, eliminates duplicativeassessment data, and improves consistency in theassessment process. Whether using the SAAMinstrument or the CHA instrument, functional statusLevel of Care ScoreThe NYSDOH developed a functional assessmentscoring system, the Nursing Facility Level of Care(NFLOC) score, based on the CHA instrument. TheNFLOC score is comprised of 11 components that arederived from 22 items from the UAS-NY instrument.The items include the areas of incontinence, cognitiveperformance, Activities of Daily Living (ADLs), andbehavior. Points are allocated to the different levelsof functioning, with the number of points increasingas the functional deficits increase. The maximumnumber of points is 48. A Level of Care Score of fiveor more indicates need of services usually providedin a nursing home.The current statewide average CHA NFLOC scoreis 19.5. Some measures in this report are based onthe NFLOC score and its components, allowing fora comparison of case-mix among the plans.8
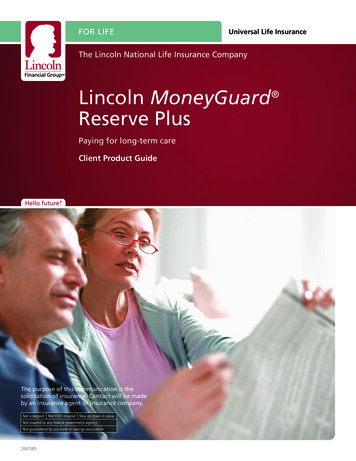
Demographic Profile of MLTC Enrolleesmembers are over the age of 64. Over two-thirdsof the enrollees are nonwhite (71 percent) and10 percent were in a nursing home at the timeof the assessment. Almost 81 percent have beencontinuously enrolled in MLTC for 12 months or more.The data in Table 1 are based on CHA data for theJanuary through June 2019 enrollment period andtherefore reflect the characteristics of the enrolleesduring that time frame. As shown, 83 percent ofTable 1Demographic ProfileMeasurePercentMeasureAge GroupingsPercentPayment SourceAge 210.0Dually Enrolled in Medicaid and Medicare85.1Age 21-546.7Medicaid Only14.9Age 55-6410.9Current LocationAge 65-7427.4CommunityAge 75-8430.2Hospital0.4Age 85 24.9Missing0.0GenderNursing HomeMale31.4OtherFemale68.6Living SituationRace88.710.30.6Alone34.3Black Non-Hispanic17.1With Family/Relative51.2Hispanic24.2With Other14.4Other29.4White Non-Hispanic29.3Most Frequent Diagnoses Statewide(Percent of All Members)Primary LanguageChinese12.2English41.8Missing2.4Essential Hypertension77.3Other Nervous System Disorder74.6Genitourinary Symptomsand Ill-Defined Conditions67.6Osteoarthritis66.8Other11.8Disorders of Lipid Metabolism61.7Russian10.3Esophageal Disorders51.5Spanish21.5Other Gastrointestinal Disorder51.2Continuously Enrolled 12 Months80.5Coronary Atherosclerosisand Other Heart Disease47.6Continuously Enrolled 12 Months19.5Nutritional Deficiencies42.9Diabetes Mellitus without Complications41.1Enrollment9
Utilization and Patient Safetyand congestive heart failure (CHF) (exacerbationof CHF, fluid overload, heart failure). Likewise,up to four of nine given reasons for ER visits maybe selected. Table 2 highlights the most commonclinical reasons for ER visits: respiratory (respiratoryproblems, shortness of breath, respiratory infection,tracheobronchial obstruction), cardiac (cardiacproblems, fluid overload, exacerbation of CHF, chestpain), nausea (nausea, dehydration, malnutrition,constipation, impactions), hypo/hyperglycemia,and wound problems (infection, deteriorating woundstatus, new lesion/ulcer). Please note that Table 2is based on events and not members, and not alladmission or visit reasons are presented; therefore,the total percent may not equal 100 percent.The table below shows that 12 percent of thepopulation was admitted to a nursing home, with themajority admitted for long-term placement followedby therapy services. Twelve percent of enrolleeswere admitted to the hospital at least once, with20 percent admitted for respiratory problemsand 10 percent for falls. Six percent of enrollees hadat least one ER visit, with 10 percent for respiratoryproblems and five percent for cardiac problems.The following hospital and nursing home utilizationdata were derived from MLTC CHA conducted forthe January 1, 2019 through June 30, 2019 timeperiod. Table 2 shows the statewide percentageof members who within the last 90 days or sincethe last assessment if less than 90 days ago had:1) a nursing home admission and reasons for nursinghome admissions; 2) at least one, or two or morehospitalizations and reasons for hospital admissions;and 3) at least one, or two or more emergency room(ER) visits and reasons for ER visits. For nursinghome, up to four reasons for admission may beselected. Table 2 shows nursing home admissionsstratified by those for long-term placement, therapyservices, unsafe for care at home, end of life care,and respite care. Up to four of 16 given reasonsfor hospital admission may be selected. Table 2highlights categories that represent the morecommon clinical reasons for hospital admission:respiratory (respiratory problems, shortness ofbreath, infection, obstruction, COPD, pneumonia);falls (injury caused by fall or accident at home);scheduled surgical procedure; urinary tract infection;Table 2Utilization and Patient SafetyAdmissions/VisitsAt LeastOneFacility TypeNTwo orMore%NAdmissions/Visits for Known Reasons, Percent%Nursing Home31,062 12**AdmissionsReason 1%Reason 2 %Reason 3%Long-Term66PlacementTherapy31ServicesUnsafe12at HomeReason 4%End of1Life CareReason 5%RespiteCare1Urinary CongestiveHospitalScheduled31,463 124,723 2Respiratory 20Falls 109Tract7Heart7AdmissionsProcedureInfection FailureEmergency16,390 62,282 1Respiratory 10Cardiac 5Nausea 3Room Visits*No data to report.10Hypo/Hyper2glycemiaWound1
Plan Profilescounts as of November 2019 are presented. Pleaserefer to Appendix B for a listing of counties within eachregion. Plans may not be enrolling in every countyin a region. Please verify availability with the plan.Table 3 summarizes the MLTC plans certified as ofNovember 2019 by the NYSDOH to enroll Medicaidrecipients. Regions of enrollment and enrollmentTable 3Health Plan ProfilesHealth Plan Name and WebsiteRegions of EnrollmentEnrollment(As of Nov. 2019)Partial Capitation1. Aetna Better Healthwww.aetnabetterhealth.comLong Island, New York City 8,2482. AgeWell New Yorkwww.agewellnewyork.comHudson Valley, Long Island, New York City3. ArchCare Community Lifewww.archcare.orgHudson Valley, New York City 5,0964. Centers Plan for Healthy Livingwww.centersplan.comHudson Valley, Long Island, New York City, Western37,9855. Elderplan dba Homefirstwww.elderplan.orgHudson Valley, Long Island, New York City15,1146. ElderServe dba RiverSpringwww.riverspringathome.orgHudson Valley, Long Island, New York City15,3367. E lderwood Health Planwww.elderwoodhealthplan.comWestern 9358. Empire BCBS HealthPlus MLTCmss.empireblue.com/ny/home.htmlNew York City 7,2159. EverCare Choicewww.evercare.orgHudson Valley 1,00312,34810. Extended MLTCwww.extendedmltc.orgLong Island, New York City 6,95611. Fallon Health Weinbergwww.fallonweinberg.orgWestern 96812. Fidelis Carewww.fideliscare.orgCentral, Hudson Valley, Long Island,New York City, Northeast, Western13. Hamaspik Choicewww.hamaspikchoice.orgHudson Valley 2,42414. iCirclewww.icirclecny.orgCentral, Northeast, Western 4,42515. Integra MLTCwww.integraplan.orgHudson Valley, Long Island, New York City16. Kalos Healthwww.kaloshealth.orgWestern 1,52217. MetroPlus MLTCwww.metroplus.orgNew York City 2,0771123,47423,985
Table 3 (Continued)Health Plan ProfilesHealth Plan Name and WebsiteRegions of EnrollmentEnrollment(As of Nov. 2019)Partial Capitation (Continued)18. Montefiore MLTCwww.montefiore.orgHudson Valley, New York City 1,76519. Nascentia Health Optionswww.nascentiahealthoptions.orgCentral, Northeast, Western 7,98620. Prime Health Choicewww.primehealthchoice.comHudson Valley, Northeast 54821. Senior Health Partnerswww.shpny.orgHudson Valley, Long Island, New York City22. Senior Network Healthhttps://mvhealthsystem.orgCentral 59923. Senior Whole Health Partialwww.seniorwholehealth.comHudson Valley, New York City14,96924. V illageCareMAXwww.villagecaremax.orgNew York City12,27125. VNS CHOICE MLTCwww.vnsnychoice.orgCentral, Hudson Valley, Long Island, New York City,Northeast, Western19,97026. WellCare Advocate Partialwww.wellcare.comHudson Valley, Long Island, New York City,Northeast, Western15,3945,834Program of All-Inclusive Care for the Elderly (PACE)27. ArchCare Senior Lifewww.archcare.orgHudson Valley, New York City 81128. Catholic Health – LIFEwww.chsbuffalo.orgWestern 26029. CenterLight PACEwww.centerlighthealthcare.orgHudson Valley, Long Island, New York City 2,66230. Complete Senior Carewww.hanci.comWestern 12531. Eddy Senior s-ccNortheast32. E lderONEwww.elderone.orgWestern 75733. Fallon Health Weinberg – PACEwww.fallonweinberg.orgWestern 14834. PACE CNYwww.pacecny.orgCentral 65135. Total Senior Carewww.totalseniorcare.orgWestern 12912213
Table 3 (Continued)Health Plan ProfilesHealth Plan Name and WebsiteRegions of EnrollmentEnrollment(As of Nov. 2019)Medicaid Advantage Plus (MAP)36. Centers Plan MAPwww.centersplan.comHudson Valley, Long Island, New York City 1437. E lderplanwww.elderplan.orgHudson Valley, Long Island, New York City 1,60738. Empire BCBS HealthPlus MAPmss.empireblue.com/ny/home.htmlNew York City 1339. Fidelis Legacy Planwww.fideliscare.orgNew York City, Northeast 7540. MHI Healthfirst Complete Carewww.healthfirst.orgHudson Valley, Long Island, New York City41. RiverSpring MAP*www.riverspringathome.orgHudson Valley, Long Island, New York City 042. Senior Whole Healthwww.seniorwholehealth.comLong Island, New York City 9343. VillageCareMAX Total Advantagewww.villagecaremax.orgNew York City 1,71044. VNS CHOICE Totalwww.vnsnychoice.orgHudson Valley, Long Island, New York City 2,32811,860 Fully Integrated Duals Advantage (FIDA)45. Elderplan FIDA Total Carewww.elderplan.orgLong Island, New York City 28046. FIDA Care Completewww.centersplan.comNew York City 1247. Healthfirst AbsoluteCare FIDAwww.healthfirst.orgHudson Valley, Long Island, New York City 93748. RiverSpring FIDAwww.riverspringathome.orgHudson Valley, Long Island, New York City 1349. SWH Whole Health FIDAwww.seniorwholehealth.comNew York City 9950. VNSNY CHOICE FIDA Completewww.vnsnychoice.orgHudson Valley, Long Island, New York City 1,027*Plan not operational during time of data collection.13
Enrollee Attributesenrollment. Assessments conducted by Adult DayHealth Care were excluded from all measures.Some members may have had multiple assessmentsduring the enrollment period; therefore, only themost recent assessment related to a plan enrollmentis included in the measures.Measures are reported as percentages of theeligible population. Variation and/or extremes inresults are difficult to interpret for plans with lowenrollment. Therefore, plans with fewer than 30eligible members are excluded from the plan-levelcalculations and reported in the tables as SS(Small Sample), but their data are still includedin the calculation of statewide averages.The tables on the following pages describe thefunctional and health status of the MLTC population.Within this section, the measures are combined intothe following domains of care: 1) Overall Functioningand Activities of Daily Living, 2) Continence, Neuro logical, and Behavioral Status, and 3) Living Arrange ment and Emotional Status. Appendix C describesthe measures used for each type of analysis.Measures are based on the January 1, 2019, throughJune 30, 2019, enrollment period. Assessmentsconducted for any reason other than “first assess ment” must occur within the enrollment period.Assessments specified as first assessments mayoccur up to 45 days
to the Partnership Plan Medicaid Section 1115 Demonstration waiver required all dual-eligible individuals (persons in receipt of both Medicare and Medicaid benefits) ages 21 or older and in need of community-based long-term care services for more than 120 days to be mandatorily enrolled into Managed Long-Term Care Plans. The transition to MLTC .