Transcription
200 Hour Teacher Training November 2016MANUAL 3ANATOMY
1CONTENTS1 FUNCTIONAL ANATOMY31.1 Anatomical Position41.2 Anatomical Terms51.3 Muscles and Action7Upper ExtremityDeltoidPectoralis MajorBiceps BrachiiTriceps BrachiiRotator CuffSupraspinatusInfraspinatusTeres MinorLower nosus & Semi-tendinosusBiceps FemorisGluteus MaximusCalf MusclesHip AdductorsIliopsoasTrunk MusclesLatissmus DorsiTrapeziusAbdominal MusclesRectus Abdominus ActionExternal Oblique ActionInternal Oblique ActionTransversus Abdominus ActionErector Spinae1.4 Muscle PropertiesOrigin and InsertionReverse Origin and InsertionReverse Origin and InsertionReciprocal 1919202021212324242525Co-contractionStretch ReflexGolgi Tendon ReflexPNFPNFSlow Reversal Contract RelaxSlow Reversal Contract Relax1.5 Vertebral ColumnVertebral ColumnFunction of Vertebral ColumnSpinal CurvesCervical VertebraeThoracic VertebraeLumbar VertebraeSacrumCoccyxIntervertebral DiscSpinal CanalYoga Pose ImplicationAnatomical Concept to Yoga1.6 Knee Joint ComplexKnee Joint ComplexPatello-Femoral jointFemoro-Tibial JointKnee ComplexPatello-femoral Joint SyndromeMeniscusLigaments of the Knee ComplexAnterior Cruciate LigamentPosterior Cruciate LigamentCollateral LigamentsUnhappy TriadYoga Pose Implication1.7 Hip JointHip JointHip JointHip JointHip Joint Stability VIKASA YOGA - Foundation Teacher Training Manual - 040414142434344444545464748484949
2CONTENTS CONTINUED.Hip MovementQ AngleQ AngleQ AngleQ Angle Yoga Pose Implication50505151521.8 Shoulder Girdle53Shoulder GirdleShoulder GirdleGlenohumeral JointGlenohumeral JointGlenohumeral Joint MovementGlenohumeral Joint CapsuleGlenohumeral Joint MovementShoulder StabilisersAcromoclavicular JointAcromoclavicular Joint FunctionSternoclavicular JointScapulohumeral jointScapula MovementYoga Pose Implication54545555565657575858595960601.9 Pelvic Girdle61Pelvic Girdle FunctionWeight transmissionDifference between male and female PelvisPelvic MovementSacro-iliac JointSacro-iliac JointSacro-iliac Joint ligamentsSacro-iliac Joint FunctionSacro-iliac Joint Dysfunction2 DIGESTIVE ANATOMYDigestive SystemBasic Division of Digestive SystemGI TractAccessory OrgansProcess of DigestionTypes of DigestionEsophagusGall iverPancreasStomachSmall IntestineLarge IntestineCecum and ColonColonRectum and Anal Canal3 RESPIRATORY ANATOMYRespiratory SystemRespiratory TractBreathing MechanismInhalationExhalationGaseous Exchange4 APPLIED ANATOMY73737474757576767778797980808183Method of Analysis84Trikonasana - Triangle Pose85Anjaneyasana - Crescent Pose86Vasisthasana - Side Plank87Parsvakonasana - Side Angle Pose88Parivrtta Parsva Konasana - Revolved Side Angle Pose 89Ardha Matsyendrasana - Half Spine Twist90Navasana - Boat Pose91Salabhasana - Locust Pose92Jathara Parivartanasana - Revolved Abdomen Pose93Dhanurasana - Bow Pose94Ustrasana - Camel Pose95Urdhva Dhanurasana - Upward Bow (Wheel) Pose96Eka Pada Kapotasana - One-Legged King Pigeon Pose 97Sarvangasana - Shoulder Stand98Sirsasana - Head Stand99The art of observation100 VIKASA YOGA - Foundation Teacher Training Manual - Anatomy
31 FUNCTIONAL ANATOMY VIKASA YOGA - Foundation Teacher Training Manual - Anatomy
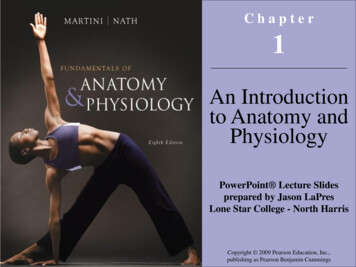
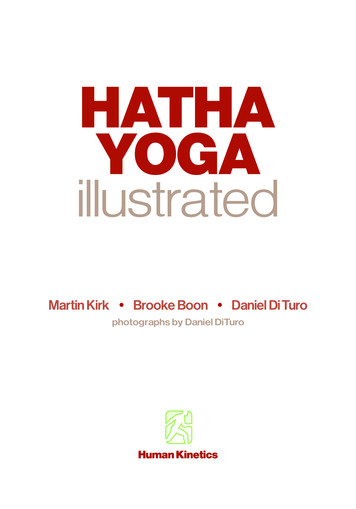
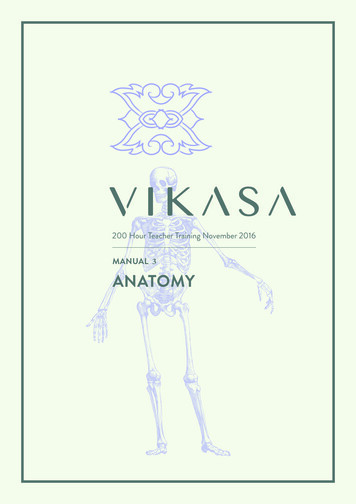
41.1 ANATOMICAL POSITIONAnatomical PositionStanding erect, facing the observer, arms are at the sides withpalms facing forward.Figure 1: Anatomical Position VIKASA YOGA - Foundation Teacher Training Manual - Anatomy
51.2 ANATOMICAL TERMSFlexionSupinationAway from an anatomical position in sagittal planeExternal rotation of the radiohumeral jointExtensionInversionReturn to anatomical position from flexed positionTurn sole of foot until it faces inwardHyper-extensionEversionMovement past midline in sagittal planeTurn sole of foot until it faces outwardLateral flexionAnterior Pelvic TiltMid line structure flexes either wayASIS moves anterior to the PSAbductionPosterior Pelvic TiltMovement away from mid line in frontal planeASIS moves posterior to the PSAdductionMovement toward mid line in frontal plane* ASIS Anterior Superior Iliac Spine** PS Pubic SymphysisElevationMedial / internal rotationPart of body (scapula) moves superiorMovement toward mid line along the longitudinal axisLateral / external rotationDepressionPart of body (scapula) moves inferiorMovement away from mid line along the longitudinal axisDorsi-flexionProtractionPart of body (scapula) moves anteriorFlex ankle until toes point upwardRetractionPlantarflexionPart of body (scapula) moves posteriorPoint toes downwardCircumductionPronationInternal rotation of the radiohumeral jointConsists of flexion, abduction, adduction, extensionperformed in succession VIKASA YOGA - Foundation Teacher Training Manual - Anatomy
6ANATOMICAL TERMS CONTINUED.SuperiorMedialToward the headToward the mid line that divides left and rightInferiorLateralAway from the headTo the side away from the mid lineAnteriorProximalThe front of the body or body partCloser to the torsoPosteriorDistalThe back of the body or body partFarther away from the torsoNOTES VIKASA YOGA - Foundation Teacher Training Manual - Anatomy
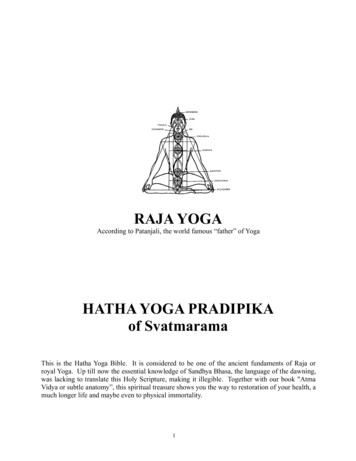
71.3 MUSCLES AND ACTIONLEARN MUSCLE GROUPS AND THEIR ACTIONSFigure 2: Anterior and Posterior View VIKASA YOGA - Foundation Teacher Training Manual - Anatomy
8Upper Extremity Deltoid Pectoralis major Biceps brachii Triceps brachii Rotator cuffFigure 3: Upper ExtremityDeltoidAnterior portion Flex and medially rotate armat shoulder jointMiddle portion Abduct armPosterior portion Flex and laterally rotate armat shoulder jointFigure 4: Deltoid VIKASA YOGA - Foundation Teacher Training Manual - Anatomy
9Pectoralis Major Clavicular head flexes humerus Sternocostal head extendshumerus 2 heads together flex, horizontallyflex and adduct arm Elevate rib cage if arms andscapulae are fixedFigure 5: Pectoralis MajorBiceps Brachii Long head flex arm atshoulder joint Long and short head - supinatesforearm and, when it is supine,flexes forearmFigure 6: Biceps Brachii VIKASA YOGA - Foundation Teacher Training Manual - Anatomy
10Triceps Brachii 3 heads 1 long head, 2 shortheads Chief extensor of forearm; longhead steadies head of abductedhumerusFigure 7: Triceps BrachiiRotator Cuff Supraspinatus Infraspinatus Subscapularis Teres MinorA.B.Figure 8 A & B: Rotator Cuff VIKASA YOGA - Foundation Teacher Training Manual - Anatomy
11Supraspinatus Initiates and assists deltoid inabduction of arm and acts withother rotator cuff musclesB.Figure 9 A & B: SupraspinatusA.Infraspinatus Laterally rotate arm; helps to holdhumeral head in glenoid cavity ofscapulaFigure 10: Infraspinatus VIKASA YOGA - Foundation Teacher Training Manual - Anatomy
12Teres Minor Laterally rotate arm; helps to holdhumeral head in glenoid cavity ofscapulaFigure 11: Teres MinorLower Extremity Quadriceps Hamstrings Gluteus Maximus Calf muscles Hip Adductors IliopsoasFigure 12: Lower Extremity VIKASA YOGA - Foundation Teacher Training Manual - Anatomy
13QuadricepsMade up of 4 muscles: Vastus Lateralis Vastus Medialis Vastus Intermedialis Rectus FemorisRectus Femoris hidden to revealVastus IntermediusFigure 13: Quadriceps - 4 musclesQuadricepsKnee extension Vastus Lateralis Vastus Medialis Vastus IntermedialisHip flexion and knee extension Rectus FemorisFigure 14: Quadriceps VIKASA YOGA - Foundation Teacher Training Manual - Anatomy
14HamstringsComprises of 3 muscles: Semi-membranosus Semi-tendinosus BicepsfemorisFigure 15: Hamstrings - 3 musclesSemi-membranosus & Semi-tendinosus Extends the thigh, flexes theknee, and also rotates thetibia medially, especially whenthe knee is flexedFigure 16: Semi-membranosus & Semi-tendinosus VIKASA YOGA - Foundation Teacher Training Manual - Anatomy
15Biceps Femoris Long head and short head Flexes the knee, and alsorotates the tibia laterally;long head also extends thehip jointFigure 17: Biceps FemorisGluteus Maximus Major extensor of hip jointFigure 18: Gluteous Maximus VIKASA YOGA - Foundation Teacher Training Manual - Anatomy
16Calf Muscles Gastrocnemius (2 joint muscle) knee flexion and plantar flex ankle Soleus (single joint muscle) plantar flex ankleFigure 19: Calf MusclesHip Adductors Adductor Magnus Adductor Longus Adductor BrevisFigure 20:Hip Adductors VIKASA YOGA - Foundation Teacher Training Manual - Anatomy
17Iliopsoas Flex the torso and thigh withrespect to each otherFigure 21: IlliopsoasTrunk Muscles Latissmus Dorsi Trapezius Abdominal muscles Erector SpinaeA.B.C.Figure 22: Trunk Muscles, A. Abdominal, B. Latissimus Dorsi & Trapezius, C. Erector Spinae VIKASA YOGA - Foundation Teacher Training Manual - Anatomy
18Latissmus Dorsi Extends, adducts, and mediallyrotates humerus; raises bodytoward arms during climbingFigure 23: Latissmus DorsiTrapezius Upper Trapezius elevate scapula Middle Trapezius retract scapula Lower Trapezius depress scapulaFigure 24: Trapezius VIKASA YOGA - Foundation Teacher Training Manual - Anatomy
19Abdominal Muscles (A) Rectus Abdominus (B) External Oblique (C) Internal Oblique (D) Transverse AbdominusA.B.C.D.Figure 25 A, B, C & D: Abdominal MusclesRectus Abdominus Action Flexion of the trunkFigure 26: Rectus Abdominus Action VIKASA YOGA - Foundation Teacher Training Manual - Anatomy
20External Oblique Action Pull the chest downwards andcompress the abdominal cavity,which increases the intraabdominal pressure Flexion and rotation of thevertebral columnFigure 27: External Oblique ActionInternal Oblique Action Rotates and side-bends the trunkby pulling the rib cage and midlinetowards the hip and lower back, ofthe same side Acts with the external obliques ofthe opposite side to achieve thistorsional movement of the trunkFigure 28: Internal Oblique Action VIKASA YOGA - Foundation Teacher Training Manual - Anatomy
21Transversus Abdominus Action Provides core stability Creates Intra- abdominal pressureFigure 29: Transversus Abdominus ActionErector Spinae Major extensorof the trunkA.B.C.Figure 30: Erector Spinae. A: Spinalis Group, B: Longissimus Group, C: Iliocostalis Group VIKASA YOGA - Foundation Teacher Training Manual - Anatomy
22NOTES VIKASA YOGA - Foundation Teacher Training Manual - Anatomy
231.4 MUSCLE PROPERTIESORIGIN AND INSERTIONREVERSE ORIGIN AND INSERTIONRECIPROCAL INHIBITIONCO-CONTRACTIONSTRETCH REFLEXGOLGI TENDON REFLEX VIKASA YOGA - Foundation Teacher Training Manual - Anatomy
24Origin and Insertion The origin of a muscle is the point at whicha muscle is attached to a fixed bone, whilethe insertion of a muscle is the point atwhich a muscle is attached to a bonemoved by that muscle All voluntary muscles have an origin andinsertion An example is the bicep, which originatesat the scapula and inserts at the radialtuberocity on the radiusOriginInsertionFigure 31: Origin and Insertion of the BicepsReverse Origin and Insertion34 A: Reverse Origin & Insertioncan happen when theinsertion point becomesrelatively fixed This usually occurs at aclosed chain situationwhere the insertion pointis in contact of a surface34 B:33:Figure 33: Insertion point at contact of a surfaceFigure 34 A & B: Insertion towards origin VIKASA YOGA - Foundation Teacher Training Manual - Anatomy
25Reverse Origin and InsertionAllows body deeper into the pose Isometric anterior deltoidengagement in reverse origin andinsertion patternA:Allows body deeper into the pose Isometric TFL and gluteus medius inreverse origin and insertion patternB:Figure 35 A & B : Origin and InsertionReciprocal Inhibition When main movers (agonist)contracts, the opposing muscle(antagonist) will relax This principle is used in a facilitatedstretching technique called“Proprioceptive NeuromuscularFacilitation”, PNFFigure 36: Reciprocal Inhibition VIKASA YOGA - Foundation Teacher Training Manual - Anatomy
26Co-contraction For every muscle (agonist), there isan opposing muscle (antagonist) When both the main mover(agonist) and its opposing muscle(antagonist) are contracting, “cocontraction” is achieved The end result is “no movement”visible but maximum stability acrossa jointFigure 37: Co-contractionA: Contraction Co-contraction is very usefulto avoid hyperextension inknees and elbowsFigure 38: Hyperextension of the knee VIKASA YOGA - Foundation Teacher Training Manual - AnatomyB: Co-contraction
27Stretch Reflex When a muscle is stretched, the mechanical receptors inthe muscle called “muscle spindle” will be stimulated A reflex response will then be triggered, causing thestretched muscle to contract This “Stretch reflex” is inborn and therefore doesnot require the participation of the higher brain forinterpretation; the same stimulation will cause sameresponse every time The “Stretch reflex” helps to protect the muscle againstbeing pulled apart but it also reduces the effectiveness oftraditional stretch (passive stretch)Golgi Tendon Reflex Golgi tendon is another mechanicalreceptors present in the tendon ofa muscle When stretched, the golgi tendonwill be stimulated and triggers the“Golgi Tendon Reflex”, causingthe attached muscle to relax andthereby being elongatedFigure 39: Golgi Tendon Reflex VIKASA YOGA - Foundation Teacher Training Manual - Anatomy
28PNF PNF stretching, or “Proprioceptive Neuromuscular Facilitation” stretching,is commonly used in clinical environments to enhance both active andpassive range of motion in order to improve motor performance and aidrehabilitation PNF is considered an optimal stretching method when the aim is to increaserange of motion, especially as regards short-term changes Generally an active PNF stretch involves a shortening contraction of theopposing muscle to place the target muscle on stretch. This is followed byan isometric contraction of the target muscle PNF can be used to supplement daily stretching and to make quick gains inrange of motion – for example, to help athletes improve performancePNFTwo Principles: Reciprocal Inhibition Golgi Tendon Reflex Since there are two principles, there are severalways to conduct PNF One of the ways is to use both principles,“Slow reversal contract relax” VIKASA YOGA - Foundation Teacher Training Manual - Anatomy
29Slow Reversal Contract RelaxMethod 1:1. First bring the muscle to a stretchedposition2. Apply tension so that the target muscle iscontracting isometrically (no movement)for 6 seconds (trigger Golgi tendon reflex)3. Relax the target muscle4. Contract its antagonist muscleconcentrically and stretch out the targetmuscle5. Repeat the above processes (2 – 4) untilthe end range is achieved6. Stay in the new range for at least 10seconds before coming out of the pose1. Dig heels into mat andengage hamstrings2. Engage quadriceps tostraighten the kneeFigure 40: Slow Reversal Contract Relax 1Slow Reversal Contract RelaxMethod 2:1. Press knees against elbows oneither side to engage hip adductormuscles2. Push knees towards matFigure 41: Slow Reversal Contract Relax 2 VIKASA YOGA - Foundation Teacher Training Manual - Anatomy
30NOTES VIKASA YOGA - Foundation Teacher Training Manual - Anatomy
311.5 VERTEBRAL COLUMNCONSISTS OF A SERIES OF 33IRREGULARLY SHAPED BONES,CALLED VERTEBRAE, 26 OFWHICH ARE MOVABLE.THESE VERTEBRAE ARE DIVIDEDINTO FIVE CATEGORIES:1. CERVICAL (7)2. THORACIC (12)3. LUMBAR (5)4. SACRUM (5 FUSED)5. COCCYX (4) VIKASA YOGA - Foundation Teacher Training Manual - Anatomy
32Vertebral Column These bones compose thevertebral column, resulting in atotal of 26 movable parts in anadult In between the vertebrae areintervertebral discsFigure 42: Vertebral ColumnFunction of Vertebral Column Support the head and arms Permit freedom of movement Provides attachment for many muscles, theribs, and some of the organs Protects the spinal cord (extension from theBrain) VIKASA YOGA - Foundation Teacher Training Manual - Anatomy
33Spinal CurvesWhen looked at from the side, thespine forms four curves: cervical,thoracic, lumbar, and pelvic curvesThe cervical curve: at the top of the spine composed of cervical vertebraeThe thoracic and lumbar curves: composed of thoracic and lumbarvertebraeThe pelvic or sacral curve: formed by the sacrum and coccyxThe spinal column: Allows human beings to stand upright Help to maintain the balance of theupper body The thoracic and pelvic curves aretermed primary curves, because theyalone are present during fetal life The cervical and lumbar curves arenot present in an infant The cervical curves forms aroundthe age of 3 months (when the babybegins to hold its head up) and thelumbar curve develops when a childbegins to walk (twelve or eighteenmonths)Cervical CurveThoracic CurveLumbar CurveSacral CurveFigure 43: Vertebral Column VIKASA YOGA - Foundation Teacher Training Manual - Anatomy
34Cervical Vertebrae The first seven vertebrae (C1-7) Located at the top of the spinalcolumn Supportive framework for the neckand support the head The first cervical vertebrae is calledthe atlas and the second is calledthe axis (responsible for rotation ofcervical spine) Possesses bifid spinous processes,which is absent in C7 Small-bodiedFigure 44: Cervical VertebraeThoracic Vertebrae Twelve vertebrae with ribs anchor atthe rear to form rib cage (T1-12) Thoracic vertebrae are larger thancervical vertebrae and increase insize from top to bottom Distinguished by the presence ofcostal facets for the articulation ofthe heads of ribs Body is intermediate in size betweenthe cervical and lumbar vertebraeFigure 45: Vertebral Column VIKASA YOGA - Foundation Teacher Training Manual - Anatomy
35Lumbar Vertebrae Five bones below thoracic spine (L1-5) Largest vertebrae in the spinal column Support most of the body’s weight Form attachments to many of theback muscles Has a large body Does not have costal facets nortransverse process foraminaFigure 46: Lumar VertebraeSacrum Triangular bone located just belowthe lumbar vertebrae (S1-5) Consists of four or five sacralvertebrae in a child Become fused into a single boneafter age 26 The sacrum forms the back wall ofthe pelvic girdle and moves with itB.A.Figure 47 A & B: Sacrum VIKASA YOGA - Foundation Teacher Training Manual - Anatomy
36Coccyx Forms the bottom of the spinalcolumn (Co1-5) Consists of 3-5 bones that arefused together in an adult Many muscles connect to thecoccyxFigure 48: CoccyxIntervertebral Disc Made of fibrous cartilage Act as shock absorbers and allowthe back to move As a person ages, these discscompress and shrink, resulting ina distinct loss of height (generallybetween 0.5 and 2.0cm) betweenthe ages of 50 and 55Figure 49: Intervertebral Disk VIKASA YOGA - Foundation Teacher Training Manual - Anatomy
37Spinal Canal Spinal canal vertebral canal spinalcavity The space in vertebrae through which thespinal cord passes. Enclosed within the intervertebral foramenof the vertebraeFigure 50: Spinal CanalYoga Pose Implication Cat Stretch Back BendFigure 51: Cat PoseFigure 52: Urdhva Dhanurasana/Chakrasana VIKASA YOGA - Foundation Teacher Training Manual - Anatomy
38Anatomical Concept to Yoga Compression Tension ProportionNOTES VIKASA YOGA - Foundation Teacher Training Manual - Anatomy
391.6 KNEE JOINT COMPLEXTHE KNEE IS A COMPLEX, COMPOUND JOINTCOMPRISING OF TWO SEPARATE JOINTS:1. THE PATELLO-FEMORAL JOINT2. THE FEMORO-TIBIAL JOINT THAT LINKS THEFEMUR WITH THE TIBIA. VIKASA YOGA - Foundation Teacher Training Manual - Anatomy
40Knee Joint Complex Connecting the femur andthe tibia Since in humans the kneesupports nearly the entireweight of the body, it isthe joint most vulnerableboth to acute injury andto the development ofosteoarthritisFigure 53: Knee Joint ComplexPatello-Femoral joint Consists of the patella (asesamoid bone) which sits withinthe quadriceps tendon and thepatellar groove on the front ofthe femur through which it slidesFigure 54: Patello-Femoral Joint VIKASA YOGA - Foundation Teacher Training Manual - Anatomy
41Femoro-Tibial Joint Links the femur with the tibiaFigure 55: Fibro-Tibial JointKnee ComplexMovement: Flexion Extension Rotation (Knee bent) VIKASA YOGA - Foundation Teacher Training Manual - Anatomy
42Patello-femoral Joint Syndrome The patella and its tendon transmitpower from the quadriceps to thelower leg. Normally, as the kneebends, the patella slides smoothlyalong a groove in the thigh bone.However, under certain conditionsthe patella may experience forceswhich push it against the sides ofthe groove, causing pain Additionally, inflammation androughening of the smoothunderside of the patella mayoccur. Collectively, this processis referred to as patello-femoralsyndrome (PFS) The pain is usually located in thefront part of the knee, but may beon the inside, outside, or vaguelylocated. The pain can feel eithersharp or dull, and is often madeworse by squatting or walking downstairs. Sometimes there is grindingor clickingFigure 56: Patello-Femoral Joint SyndromePredisposing factors include:1. Training errors - excess hill work,stairs, or too much distance2. Biomechanical abnormalities overpronation, “knock knees”,poor pelvic control3. Muscle tightness - calf,hamstrings, iliotibial band, orvastus lateralis4. Muscle weakness - vastus medialisobliquus (VMO), gluteus VIKASA YOGA - Foundation Teacher Training Manual - Anatomy
43Meniscus Cartilaginous elements within theknee joint Serve to protect the ends of thebones from rubbing on each otherand to effectively deepen thetibial sockets into which the femurattaches Plays a role in shock absorption There are two menisci in each knee,the medial meniscus and the lateralmeniscus Either or both may be cracked, ortorn, when the knee is forcefullyrotated and/or bentFigure 57: A & B MeniscusLigaments of the Knee Complex The integrity of the Knee complex is maintainedby the 4 ligaments and the muscles surroundingthe joint The 4 ligaments are:- Anterior Cruciate Ligament- Posterior Cruciate Ligament- Medial Collateral Ligament- Lateral Collateral Ligament VIKASA YOGA - Foundation Teacher Training Manual - Anatomy
44Anterior Cruciate Ligament It connects from a posterio- lateralpart of the femur to an anterio-medialpart of the tibia. These attachmentsallow it to resist forces pushing the tibiaforward relative to the femur The ACL is often torn during suddendislocation, torsion, or hyperextensionof the knee. It is a very common injuryin hockey, skiing, skating and footballdue to the enormous amount ofpressure, weight and number of blowsthe knee must withstandFigure 58: Anterior Cruciate LigamentPosterior Cruciate Ligament It connects the posteriorintercondylar area of the tibia tothe medial condyle of the femur.This configuration allows the PCLto resist forces pushing the tibiaposteriorly relative to the femurFigure 59: Posterior Cruciate Ligament VIKASA YOGA - Foundation Teacher Training Manual - Anatomy
45Collateral Ligaments The Medial Collateral Ligaments ison the medial side of the joint. Itis a broad, flat, membranous band,situated slightly posterior on themedial side of the knee joint It resists forces pushing the kneemedially (towards the body), whichwould otherwise produce valgus(knock knee) deformity The Lateral Collateral Ligaments is onthe lateral side of the joint. It resistsforces pushing the knee laterally(away from the body)Figure 60: Collateral LigamentsUnhappy Triad The injuries of anterior cruciateligament, the medial meniscus andthe medial collateral ligament areclosely connected together The close association between thesestructures is the main cause of the“unhappy triad”Figure 61: Unhappy Triad VIKASA YOGA - Foundation Teacher Training Manual - Anatomy
46Yoga Pose Implication Warrior PoseFigure 62: Virabhadrasana - Warrior IINOTES VIKASA YOGA - Foundation Teacher Training Manual - Anatomy
471.7 HIP JOINTFORMED BY: HEAD OF THE FEMUR AND THE CUP-LIKEACETABULUM OF THE PELVIS. IT IS A BALL AND SOCKETJOINT.THE HIP JOINT FORMS THE PRIMARY CONNECTIONBETWEEN THE BONES OF THE LOWER LIMB AND THEAXIAL SKELETON OF THE TRUNK AND PELVIS.THE DEPTH OF THE ACETABULUM IS INCREASED BY AFIBROCARTILAGINOUS RIM CALLED A LABRUM THATGRIPS THE HEAD OF THE FEMUR AND SECURES IT INTHE JOINT. VIKASA YOGA - Foundation Teacher Training Manual - Anatomy
48Hip Joint The large head of the femur iscompletely covered in hyalinecartilage except for a small areacalled the fovea or pit. This isthe site of attachment for anintracapsular ligament (called theligamentum teres) that attachesdirectly from the head of the femurto the acetabulumFigure 63: Fevora & Ligamentum TeresHip Joint The head of the femur is attachedto the pelvis by a thin neck regionthat is often prone to fracturein the elderly, mainly due tothe degenerative effects ofosteoporosisFigure 64: Head of the Femur VIKASA YOGA - Foundation Teacher Training Manual - Anatomy
49Hip Joint The strong but loose fibrous capsuleof the hip joints permits the hipjoint to have the second largestrange of movement (second onlyto the shoulder) and yet supportthe weight of the body, arms andheadFigure 65: Hip Joint CapsuleHip Joint Stability In the healthy hip joint the femoral headis continually in close and stable contactwith the socket during all movements The stability of the healthy hip joint isprovided by:- thick joint capsule- a system of joint ligaments built in thejoint capsule- ligament inside the hip joint itself(ligamentum teres) These joint structures create a passiveresistant force on the hip joint that keepsthe femoral head in close contact with thehip joint socket during all movements Moreover, the 19 muscles surrounding thehip joint provide further dynamic stabilityto the hip joint VIKASA YOGA - Foundation Teacher Training Manual - Anatomy
50Hip Movement Flexion Extension Abduction Adduction InternalRotation ExternalRotation CircumductionQ AngleASIS The Q Angle (or quadriceps angle) isformed in the frontal plane by two linesegments: from tibial tubercle to the middle of thepatella from the middle of the patella to theASIS The typical Q-angle for men is 14degrees and for women is 17 degrees. Women usually have a higher Q angledue to their naturally wider pelvis. If measured laying down the angle willbe 1-3 degrees lower.Q-angleMidPatellaeTibialTubercleFigure 66: Q Angle VIKASA YOGA - Foundation Teacher Training Manual - Anatomy
51Q Angle An abnormally high Q Angle cancause stress on the entire kineticchain of the lower extremitycausing many conditions from lowback pain to foot painFigure 67: Q Angle - HighQ AngleIncreases in Q Angle are associated with: femoral anteversion external tibial torsion laterally displaced tibial tubercle genuvalgus VIKASA YOGA - Foundation Teacher Training Manual - Anatomy
52Q Angle Yoga Pose Implication Triangle Pose Lotus PoseFigure 68: Trikonasana - Triangle PoseFigure 69: Padmasana - Lotus PoseNOTES VIKASA YOGA - Foundation Teacher Training Manual - Anatomy
531.8 SHOULDER GIRDLETHE MOST MOBILE JOINT IN THE HUMAN BODY.THE SHOULDER GIRDLE IS ABLE TO CIRCUMDUCTTHROUGH A FULL 360 IN THE SAGITTAL PLANE.THIS TREMENDOUS RANGE OF MOTION HOWEVERMAKES THE SHOULDER EXTREMELY UNSTABLE, ANDFAR MORE PRONE TO DISLOCATION AND INJURYTHAN OTHER JOINTS. VIKASA YOGA - Foundation Teacher Training Manual - Anatomy
54Shoulder Girdle The most mobile joint in thehuman body Able to circumduct through a full360 in the sagittal plane This tremendous range of motionhowever makes the shoulderextremely unstable, far moreprone to dislocation and injurythan other jointsFigure 70: Shoulder Girdle - musclesShoulder Girdle4 different joints: Sternoclavicular joint Glenohumeral joint Acromoclavicular joint Scapulohumeral jointExploded viewFigure 71: Shoulder Girdle - 4 different Joints VIKASA YOGA - Foundation Teacher Training Manual - Anatomy
55Glenohumeral Joint Commonly known as theshoulder joint A synovial ball and socket JointFigure 72: Glenohumeral (shoulder) Joint front viewGlenohumeral Joint Articulation between glenoid fossaof the scapula (shoulder blade) andhead of humerus A ball and socket joint that allowsfor big range of movementFigure 73: Glenohumeral (shoulder) Joint rear view VIKASA YOGA - Foundation Teacher Training Manual - Anatomy
56Glenohumeral Joint Movement The glenoid fossa is shallow andcontains the glenoid labrum whichdeepens it and aids in stability 120 degrees of unassisted flexion,the glenohumeral joint is the mostmobile joint in the bodyFigure 74: Glenohumeral joint MovementGlenohumeral Joint Capsule A loose capsule (lax inferiorly) and therefore is at riskof dislocation inferiorly The long head of the biceps brachii muscle travelsinside the capsule A number of bursas in the capsule aid mobility The bursa are formed by the synovial membrane of thejoint capsule It is important to note that the shoulder joint is amuscle dependent joint as it lacks strong ligaments VIKASA YOGA - Foundation Teacher Training Manual - Anatomy
57Glenohumeral Joint Movement Flexion Extension Abduction Adduction Internal rotation External rotation CircumductionShoulder Stabilisers The rotator cuff is ananatomical term givento the group of musclesthat act to stabilize theglenohumeral joint The rotator cuff musclesof the shoulder producean inward pulling force,and help to pull the headof the humerus into theglenoid fossaFigure 75: Shoulder Stabiliser muscles VIKASA YOGA - Foundation Teacher Training Manual - Anatomy
58Acromoclavicular Joint Located between the acromialprocess of the scapula (tip of theshoulder) and the distal end of theclavicle The capsule is reinforced by t
VIKASA YOGA - Foundation Teacher Training Manual - Anatomy 1 FUNCTIONAL ANATOMY 3 1.1 Anatomical Position 4 1.2 Anatomical Terms 5 1.3 Muscles and Action 7 Upper Extremity 8 Deltoid 8 Pectoralis Major 9 Biceps Brachii 9 Triceps Brachii 10 Rotator Cuf 10 Supraspinatus 11 Infraspinatus 11 Teres Minor 12 Lower Extremity 12