Transcription
Speech-LanguagePathologists ( SLP)Role inNeurologicalInjuriesBY OLIVIA SANTANGELO M.S. CCC-SLP AND GARRETT MALLICOAT M.S. CCC-SLP
Learning Objectives SLP background/training SLP role when working with patients post neurological injury Establish guidelines for when to consult SLP Bedside swallow evaluation vs. nursing swallow screen Discrediting myths regarding dysphagia
Who are we? An SLP has to go through a minimum of 6 years of advancededucation 4 year bachelor’s degree 2 year master’s degree 1 year clinical fellowship (CFY) PHD programs are an additional 2 years and some SLPs go on to pursueboard certification in specific disorders such as dysphagia, voice etc.An SLPs scope of practice covers 9 components across adults andpediatrics: dysphagia, voice, cognition, language, motor speech,aural rehab, fluency, augmentative alternative communication(AAC), and social-pragmatic communication While we are a key member of the therapy team, we are unique in thatwe diagnose AND treat all the above parameters
Dysphagia Our role is to assess patients and their risk for aspiration, establish safestdiet consistency, and determine treatment plan for rehabilitation.Dysphagia can occur in relation to: Neurological Injury Compromised respiratory status Difficulty coordinating respiration/swallowing Post-op dysphagia e.g. ACDF Significant deconditioning Recurrent laryngeal nerve (RLN) damage Prolonged intubations with vocal cord dysfunction Tracheostomy Brain stem intracranial abnormalities Post-op delirium
Aphasia and ApraxiaSpeech vs. Language: Speech – the quality, clarity and intelligibility of verbal output Dysarthria – changes in timing, strength and coordination of oral musculatureand speech Apraxia of speech – changes in motor control of speech and the articulatorsLanguage – the ability to read, write and communicate wants/needsfunctionally Aphasia – can negatively impact verbal expression, auditory comprehension,written language, and/or reading
Cognition A cognitive evaluation is to determine areas of cognitive deficitssuch as memory, attention, executive function, safety awareness,problem solving, etc. We then determine how these cognitive deficits may negatively impacttheir ability to participate in finance and medication management andother instrumental activities of daily living. This also helps us guide treatment of cognitive deficits, determine thelevel of care needed upon discharge and ways to help improve theirfunctioning in current living environment. It is not within an SLPs scope of practice to determine patients capacityor ability to make decisions.
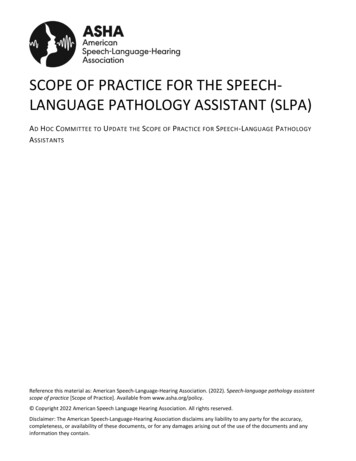
The Swallowing Mechanism 3 phases of swallowing and what they involve Oral Phase: chewing, secretion management, bolus control and transit Pharyngeal Phase: initiation of the swallow, protection of airway,passage of food/liquid into the esophagus Esophageal Phase: the passage of food into the stomach Over 50 groups of muscles andmultiple cranial nerves are initiatedduring the swallowing process!
Impairments in the SwallowMechanismWhat can go wrong: Oral phase - characterized by significant oral motor weakness, difficultychewing, fatigue from prolonged chewing, SOB can result in microaspiration of food particles. Pharyngeal phase - decreased coordination of respiration/swallowinitiation, reduced airway protection 2 weakness, physiological and/orsensory deficits of the pharyngeal musculature Esophageal phase - complaints of heart burn/acid reflux after cardiacsurgery is common, increasing risk for aspiration of reflux During a VFSS we are looking at 17 different components that contributeto functional swallowing.
Who is at an Increased Risk forAspiration? Patients with poor oral hygiene - aspiration pneumonia can occur from oralbacteria alone Those on high - flow nasal cannula (HFNC)- increased rate of forceful airflowwhile swallowing increases risk for aspiration, especially SILENT aspiration (you willnot observe a cough response) Weak/hoarse voice s/p extubation Intubation lasting longer than 48 hours Confusion/AMS/ICU delirium Weak cough response - this reduces a patient’s ability to expelpenetrated/aspirated material from airway Oral motor impairments Neurological events, especially located in the brain stem Hx of head and neck cancer Tracheostomy status
Predictors of Aspiration PneumoniaSusan Langmore (2002) listed the predictors of aspiration pneumonia tobe: 1. Suctioning 2. COPD 3. CHF 4. Feeding Tube 5. Limited mobility 6. High case mix index 7. Delirium 8. Weight Loss 9. Dysphagia 10. UTI
Pillars of Aspiration Pneumonia We know there are 3 main factors that contribute to thedevelopment of aspiration pneumonia (Ashford, n.d.): 1. Compromised Immune System 2. The Presence of Aspiration 3. Poor Oral Health Only 12% of individuals who aspirate develop aspiration pneumonia(Robbins et al., 2008). As many as 18% of healthy young adults silently aspirate regularlywithout pulmonary complications reported (Butler et al, 2018).
Dysphagia Myths True or False: Oral swabs are effective for oral care True or False: Chin tuck fixes everything Thickened liquids are not always the best solution, aspirating thickenedliquids can be more harmful than aspirating thin liquids.True or False: If a patient doesn’t cough, they don’t have dysphagia It can actually make swallowing worse, it needs to be assessed withinstrumentation such as a videofluoroscopic swallow study (VFSS)True or False: The thicker the liquid the better Toothbrushes are best, preferably a suction toothbrush, oral swabs do noteffective remove bacteria from mouthPatients can aspirate without a cough response, and multiple factors needto be considered to determine if further instrumentation is warrantedTrue or False: PEG tubes prevent aspiration and pneumonia An in depth conversation between the medical team is needed prior toplacement as it may not improve long term outcomes for certain pt.populations
Clinical Swallow Evaluation vs RNSwallow Screen Clinical swallow evaluation - to be conducted by an SLP where multiplecomponents of the swallowing process and various textures/consistencies areassessed. Oral motor structure and function Cranial nerve exam Cognition and stamina for P.O. intake Risk for aspiration Need for further instrumental assessment (i.e. video fluoroscopic swallow study)RN Swallow screen - for RN staff to complete to determine if the patient is in needof formal evaluation by SLP They may pass the screen but still have trouble with solids etc. and may need an SLPevaluation Trust your gut! If you feel like the patient is unsafe, CONSULT US!
HFNC and Dysphagia HFNC- increases the risk for aspiration, specifically silent aspiration,due to decreased ability to create adequate laryngeal vestibuleclosure and increased risk for higher air flow pressure to pushfood/liquid into the airway. There are multiple factors to consider before placing someone on adiet. E.g. FiO2 level, respiratory rate, O2 requirements, cognitivestatus, oral hygiene, etc. Eating on HFNC is a case by case basis and should be evaluated bySLP to determine risk for aspiration
Research Review on HFNC andDysphagia In a study done by Eng, Flores, and other colleagues (2019, December), in which instrumentationwas utilized on all participants, 5 out of 10 (50%) experienced silent penetration/aspiration whileon HFNC. 7 out of 10 of these participants were on thickened liquids. 4 out of 10 of these participants were cognitively impaired and minimally ambulatory. Other considerations during study: participants on lower vs high flow rates, cognitive function, andambulatory status. There are many factors which must be considered regarding po intake on HFNC, including rate ofFiO2, strength in cough response, respiratory rate, ability to manage secretions, overall strength andendurance, integrity of oral mucosa, etc. Summary: In a fairly high-functioning group, 50% had silent penetration/aspiration, regardless ofthe diet modifications/liquid viscosities. Flores and colleagues speculated that this constantpositive airway pressure from high-flow nasal cannula may lead to a “desensitization effect” atthe level of the peripheral and/or central nervous system response, leading to this aspirationbeing silent. Additionally, people need to have an adequate expiratory force to expel any matterthat enters the top of the airway (larynx and trachea). However, the high expiratory pressure fromHFNC may prevent such expectoration. Research shows that healthy and cognitively alert adults can adapt to compensate for theincreased airflow pressure when using HFNC (Allen & Galek 2020).
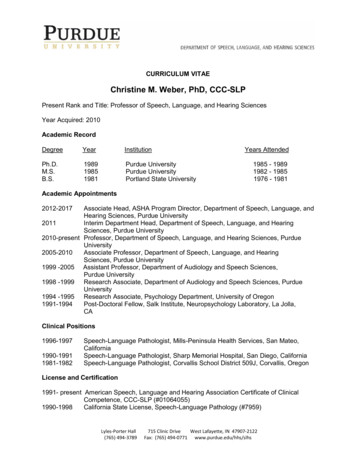
Tracheostomy and the SLP Consults can be ordered when cuff deflation trials are deemedappropriate To optimize swallowing and voice: we may recommend downsizingand/or transition to cuffless as tolerated, and coordinate placementof speaking valves with SLP and RT Speaking valves: allow the patient to breathe in from the trach, butbreathe out from nose/mouth They help restore subglottic pressure for swallowing Increase ability to coordinate voice and respirationAn inflated cuff does not mean they won’t aspirate. The cuff isbelow the VF, and anything below the VF is aspiration.
Swallowing without speaking valveSwallowing with speaking valve
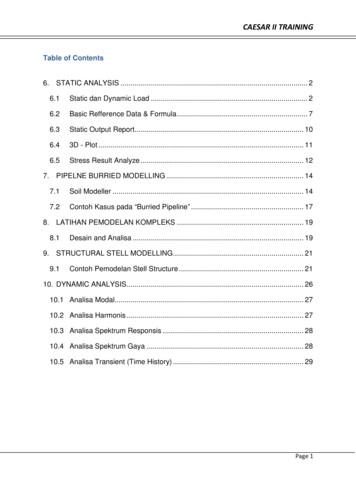
Video Fluoroscopic Swallow Study (VFSS)vs. Fiberoptic Endoscopic Evaluationof Swallowing (FEES)FEES: Can visualize vocal cords, mucosa and structuraldifferences, can be completed at bedside, with noradiation exposure- It cannot visualize oral and esophageal phasesVFSS- can look at oral,pharyngeal and esophagealphases of the swallow, pt.’sneed to be able to transfer tochair to participate
Why Instrumentation is the GoldStandard in Dysphagia The bedside eval gives us a constellation of data to inform decisionmaking for further instrumentation Instrumentation gives use the physiological impairments that wecannot detect at the bedside particularly in the pharyngeal phase Instrumentation is needed to guide our therapeutic programs forrestoration of swallow function The oropharyngeal swallow can be rehabilitated, and we can prescribean exercise program based on the deficits identified duringinstrumentationThese are not pass/fail, many different parameters are assessed andmodifications can be utilized We can repeat instrumentation as the clinical course progresses
Resources Ashford, J. R. (n.d.). Three Pillars of Pneumonia. Retrieved a/ Langmore, S. E., Skarupski, K., Park, P., & Fries, B. (2002). Predictors ofAspiration Pneumonia in Nursing Home Residents. Dysphagia, 17(4),298–307. Eng, K., Flores, M. J., Gerrity, E., Sinha, N., Imbeau, K., Erbele, L. & Yeh,C. (2019, December). Evaluation of Swallow Function on HealthyAdults While Using High-Flow Nasal Cannula. Perspectives of theASHA Special Interest Groups, 4, 1516-1524. Downloaded from:https://pubs.asha.org Allen, K. & Galek, K. (2020). The influence of airflow via high-flownasal cannula on duration of laryngeal vestibule closure. Dysphagia,published online https://doi.org/10.1007/s00455-020-10193-0
Aphasia and Apraxia Speech vs. Language: Speech -the quality, clarity and intelligibility of verbal output Dysarthria -changes in timing, strength and coordination of oral musculature and speech Apraxia of speech -changes in motor control of speech and the articulators Language -the ability to read, write and communicate wants/needs