Transcription
Health PolicyLessons learnt from easing COVID-19 restrictions: an analysisof countries and regions in Asia Pacific and EuropeEmeline Han*, Melisa Mei Jin Tan*, Eva Turk, Devi Sridhar, Gabriel M Leung, Kenji Shibuya, Nima Asgari, Juhwan Oh, Alberto L García-Basteiro,Johanna Hanefeld, Alex R Cook, Li Yang Hsu, Yik Ying Teo, David Heymann, Helen Clark, Martin McKee, Helena Legido-QuigleyThe COVID-19 pandemic is an unprecedented global crisis. Many countries have implemented restrictions onpopulation movement to slow the spread of severe acute respiratory syndrome coronavirus 2 and prevent healthsystems from becoming overwhelmed; some have instituted full or partial lockdowns. However, lockdowns and otherextreme restrictions cannot be sustained for the long term in the hope that there will be an effective vaccine ortreatment for COVID-19. Governments worldwide now face the common challenge of easing lockdowns andrestrictions while balancing various health, social, and economic concerns. To facilitate cross-country learning, thisHealth Policy paper uses an adapted framework to examine the approaches taken by nine high-income countries andregions that have started to ease COVID-19 restrictions: five in the Asia Pacific region (ie, Hong Kong [SpecialAdministrative Region], Japan, New Zealand, Singapore, and South Korea) and four in Europe (ie, Germany, Norway,Spain, and the UK). This comparative analysis presents important lessons to be learnt from the experiences of thesecountries and regions. Although the future of the virus is unknown at present, countries should continue to sharetheir experiences, shield populations who are at risk, and suppress transmission to save lives.IntroductionThe COVID-19 pandemic is an unprecedented globalcrisis. By mid-September, 2020, over 22 million confirmedcases of COVID-19 had been reported worldwide, withalmost 930 000 deaths.1 At least 186 countries haveimplemented varying degrees of restrictions on popula tion movement to slow the spread of the severe acuterespiratory syndrome coronavirus 2 and prevent healthsystems from becoming overwhelmed; these restrictionshave amounted to lockdowns in 82 countries.2 Althoughsuch measures might have saved lives, they have come ata heavy socioeconomic cost. The World Bank’s projectionspoint to the deepest global recession since World War 2,with millions of people falling into unemployment andpoverty.3 Lockdowns and other extreme restrictions cannotbe sustained for the long term in the hope that there willbe an effective vaccine or treatment for COVID-19. Rather,these restrictions give time for countries to reduce theincidence of disease and put in place robust, yet sus tainable, measures to prevent and control transmission.When and how a country should ease restrictions arethe common challenges that governments worldwide nowface as they seek to balance various health, social, andeconomic concerns. WHO has warned that a prematurelifting of lockdowns could spark a resurgence of infectionsand cause even more severe, longer-term damage to theeconomy than exists as a result of lockdowns.4 Rawaf andcolleagues5 have outlined four public-health principlesthat should be considered in each country’s exit strategy:infection status, community acceptance, public-healthcapacity, and health-system capacity. Adapting andbuilding on these prin ciples, we developed a frameworkwith add itional components and subcomponents (panel).Using this comparative framework, we examined themeasures taken in nine high-income countries andregions that have started to ease restrictions that wereimposed in response to COVID-19, which were selected toprovide a range of epidemiological experiences and policyresponses. Five countries or regions were in the AsiaPacific region (ie, Hong Kong [Special AdministrativeRegion], Japan, New Zealand, Singapore, and SouthKorea) and four were in Europe (ie, Germany, Norway,Spain, and the UK). In Asia Pacific, they include countriesand regions with and without experience of severe acuterespiratory syndrome (SARS) or Middle East respiratorysyndrome (MERS). In Europe they include countries that,in the initial wave of COVID-19, were (ie, Spain andthe UK) or were not (ie, Germany and Norway) severelyaffected. In reviewing international experiences, we havebeen concerned about an apparent absence of clear andPanel: Comparative framework for COVID-19 lockdownexit strategiesKnowledge of infection status Indicators to monitor the epidemiological situationCommunity engagement Safe policies for physical distancing and mask wearing Precautionary measures in schools and workplaces Communication to secure public trust and cooperation Protecting vulnerable populations Providing socioeconomic supportPublic-health capacity Testing, tracing, and isolating Role of expertsHealth-system capacity Treatment facilities Medical equipment Health-care workforceMeasures for border control Inbound travel restrictionswww.thelancet.com Published online September 24, 2020 shed OnlineSeptember 24, Joint first authorsSaw Swee Hock School of PublicHealth, National University ofSingapore, Singapore(E Han MSc, M M J Tan MSc,A R Cook PhD, L Y Hsu MBBS,Y Y Teo PhD,H Legido-Quigley PhD);Department of Nursing andHealth Sciences, University ofSouth East Norway, Drammen,Norway (E Turk PhD); MedicalFaculty, University of Maribor,Maribor, Slovenia (E Turk);College of Medicine andVeterinary Medicine, Universityof Edinburgh, Edinburgh, UK(D Sridhar PhD); LKS Faculty ofMedicine, The University ofHong Kong, Hong Kong SpecialAdministrative Region, China(G M Leung MD); Institute forPopulation Health, King’sCollege London, London, UK(K Shibuya DrPH); Asia PacificObservatory on Health Systemsand Policies, World HealthOrganization Regional Officefor South-East Asia, New Delhi,India (N Asgari MD); College ofMedicine, Seoul NationalUniversity, Seoul, South Korea(J Oh PhD); ISGlobal, HospitalClÍnic, Universitat de Barcelona,Barcelona, Spain(A L García-Basteiro PhD); Centrode InvestigaÇão em SaÚde deManhiÇa, Maputo,Mozambique(A L García-Basteiro);Department of Global Healthand Development(J Hanefeld PhD,H Legido-Quigley), Departmentof Infectious DiseaseEpidemiology(D Heymann DTM&H), andDepartment of Health ServicesResearch and Policy(M McKee DSc), London Schoolof Hygiene & Tropical Medicine,London, UK; Centre forInternational HealthProtection, Robert KochInstitute, Berlin, Germany(J Hanefeld); and The Helen ClarkFoundation, Auckland,New Zealand (H Clark MA)1
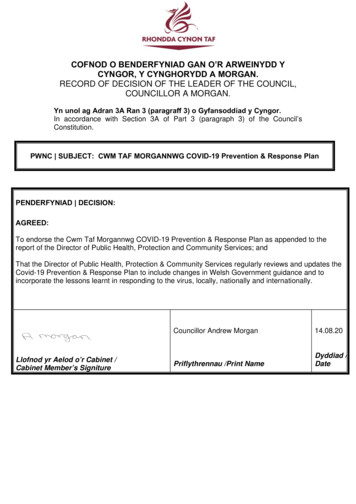
Health PolicyCorrespondence to:Dr Helena Legido-Quigley, SawSwee Hock School of PublicHealth, National University ofSingapore, Singapore 117549ephhlq@nus.edu.sgconsistent strategies for exiting restrictions. We haveidentified five prerequisites for easing COVID-19 lock downs and restrictions: knowledge of infection status,community engagement, adequate public-health capacity,adequate health-system capacity, and border controls. Wedescribe how each of these nine countries and territorieshave addressed these issues. Although it might not bepossible or beneficial to replicate the exact same measuresin different countries due to varying socioeconomiccontexts, countries can consider policy alternatives andnovel solutions developed by other countries and calibratethem according to their domestic circumstances andresources.Overall approachesThe timing of the imposition and easing of restrictions ineach country has varied (figure 1), as have nationalresponses (table). Countries will, ideally, base decisionsregarding easing restrictions on some combination of theepidemiology of infections and the social and economicconsequences of restrictions. Whichever combination ischosen, governments should be explicit about their goalsand transparent in their decision making, and themeasures taken should be parts of a clear overall strategy;however, this is not always the case.Several countries have produced dashboards of indi cators of the factors being considered, such as Japan,which considers the infection situation, the medicalservice system, and the surveillance system.6 Spain haspublished a panel of indicators, including epidemi ological, mobility, social, and economic parameters,7although without any explicit weighting in the decisionmaking process.There are two broad approaches to decision making. InSingapore, Norway, Spain, and (now for local outbreaks)the UK, politicians, drawing on expert advice, decidewhen and which restrictions to relax but without explicitJanuary115February3111529March1Lockdown ormovementcontrolorderedLockdown ormovementcontroleasedOn thebasis ofdistinctphasesOn thebasis ofa setthresholdCountry or regionGermanyHong KongJapanNew ZealandNorwaySingaporeSouth KoreaSpainUnited KingdomFigure 1: Timeline for imposing and easing of restrictions215April31115May30115and public criteria. In some cases, the activities to bepermitted are set out in advance, as in the SingaporeGovernment’s three phases of reopening, movingprogressively from lower to higher risk activities.8However, the basis on which risk is estimated is oftenunclear, with little evidence that the growing under standing of aerosol-related transmission has beenconsidered. The four nations of the UK aligned in theirstrategy until mid-March, when each nation (England,Wales, Northern Ireland, and Scotland) diverged in theirspecific approaches and exit from lockdown.Japan, Germany, South Korea, and, in some cases,the UK are lifting or reimposing restrictions on the basisof epidemiological thresholds. For example, Germany’sFederal Government has placed local authorities incharge of lifting lockdowns in individual states, subjectto a so-called emergency brake mechanism that requiresany region to consider reimposing a lockdown, if thereare more than 50 new daily cases per 100 000 residentsfor 7 consecutive days. This mechanism has alreadybeen triggered in a few districts that had spikes in thenumber of new cases, many of which were linked tooutbreaks in meatpacking plants.9 Hong Kong adopteda similar supress and lift strategy since the start ofthe outbreak, under which restrictions are tightenedand relaxed in accordance with the epide miologicalsituation.10 However, this approach risks reimposingrestrictions for an entire region even when the outbreakis limited to a single factory or small community. Theimportance of continued surveillance is clear fromNew Zealand, with its four-level alert system. Havingprogressed from a full nationwide lockdown at levelfour in late March, 2020, to minimal restrictions atlevel one in early June, 2020, New Zealand has nowhad to revert to level two nationwide and level threein Auckland.11 Although Singapore, South Korea, andthe UK also have alert-level systems, the link to particularcountermeasures has not been equally explicit, and it isnot clear that the UK’s system is being used.June31115Knowledge of infection statusIt seems intuitive that a country should not open up untilit has a surveillance system of high quality in place andhas confirmed that infections are being suppressed.Unfortunately, as shown in several countries, thisprinciple has often been disregarded.This principle involves more than producing a nationalpicture; real-time data of high quality are essential tocalculate the reproduction number (R) and to ascertainwhere the disease continues to spread, thereby enablingtargeted responses. Authorities in Hong Kong, Japan,Germany, Norway, Spain, and the UK have beenreporting estimates of R, which should be safely lessthan 1 to allow relaxation of restrictions. SinceFebruary, 2020, Hong Kong has been estimating its realtime R, the actual transmission rate of the virus, andminimising inaccuracies arising from time lags.12www.thelancet.com Published online September 24, 2020 https://doi.org/10.1016/S0140-6736(20)32007-9
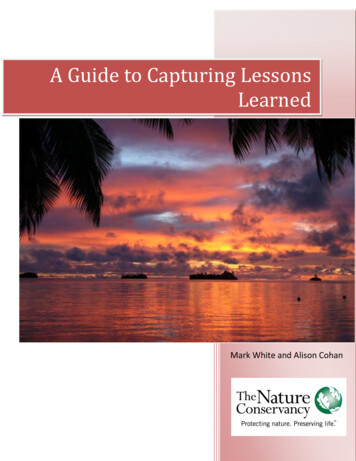
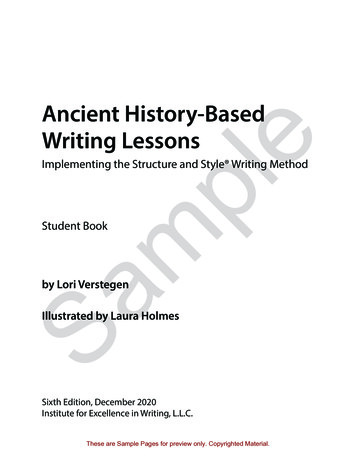
Health PolicyCountries and regions have varied in their ability toimplement effective find, test, trace, isolate, and supportsystems. Some locations in Asia, such as South Koreaand Hong Kong, had systems that functioned well at thebeginning of the pandemic, and other countries, such asGermany, were able to redeploy resources, whereas somecountries, such as the UK and Spain, have struggled.Community engagementFor societies to reopen safely, communities should befully engaged and empowered to protect themselvesfrom the virus and the effect of the crisis, especiallythe most vulnerable populations (figure 2). Ideally,authorities should ensure that they fully understand thereality of the situation faced by the people affected bytheir decisions, drawing on principles of coproduction ofpolicy. Advice should also be consistent and credible.Messaging around what is considered a safe physicaldistance between people has been confusing and incon sistent, seemingly drawing on a range of biological andother considerations, such as whether a large distancewould preclude reopening of some facilities. Thus, a 1 mdistance is recommended in Hong Kong, Singapore, andNorway; 1·5 m in Germany and Spain; and 2 m in Japan,South Korea, and, until late June, 2020, England. InEngland, the recommended distance is now at least 1 m,whereas 2 m distance is still recommended in otherparts of the UK.13 In New Zealand, 2 m distance betweenpeople is recommended in public spaces and 1 m isrecommended in schools and workplaces at high alertlevels, but there are no distancing requirements atlevel one. New Zealand also pioneered a social bubblemodel that allows a defined group of people to haveclose physical contact with each other while practisingphysical distancing rules with others outside that group.11According to this approach, what started off as householdbubbles under lockdown were slowly allowed to extendto small and exclusive groups of family and friends, andthen further allowed to expand and merge with otherbubbles. The UK nations have endorsed this idea andstarted a similar support bubble arrangement sinceJune, 2020.14OverallstrategyKnowledge ofinfection statusCommunity engagementPublic-health capacityHealth-system capacityMeasures for border controlHong KongSuppress andlift strategyReal-time Restimated andreported sinceFebruary, 20201 m physical distancing and maskwearing practised; despite seriousmistrust in government,community has shown a highrate of adherence and built theirown collective response to thepandemicDaily PCR-testing capacity beingincreased from 4500 to 10 000;police supercomputer system usedfor contact tracing and electronicwristbands paired with mobilephone apps used to monitorpeople under quarantineSecond-tier isolation beds andcommunity isolation facilitiesadded to public hospitals; safetymeasures have been effective inprotecting health-care workersfrom infectionBorder closed to visitors;all arrivals must submit ahealth declaration formonline, have temperaturescreening and testing onarrival, and serve a 14-dayquarantineJapanTrigger-based One indicator is anapproachincidence rate of 0·5 cumulativeinfections per100 000 people inthe past week2 m physical distancing and maskwearing practised; citizens areencouraged to avoid so-called3Cs (ie, closed spaces, crowdedplaces, and close contact);adherence aided by existingsocial etiquetteDaily PCR-testing capacity is lowbut is being increased from 6000tests per day in May to more than22 000 tests per day; manualtracing done and new mobilephone app introduced inJune, 2020Initially, all patients wereadmitted but, due to lowcapacity, hospitals now focuson caring for people who arevulnerable or have moderate orsevere disease; people with milddisease and people who areasymptomatic supported athome or at lodging facilitiesAll arrivals are subject to14-day quarantine, andtravellers from selectedcountries are denied entry or,if allowed for exceptionalreasons, subject to testingAsia PacificNew Zealand Four-levelalert systemNo publicly specified So-called social bubble approach Testing capacity being increased;manual and app-based tracingindicatorallowed gradual expansion ofsmall and exclusive social groups; being doneno physical distancing required atalert level oneEfforts being made to increasenumber of ICU beds andnumber of staff trained to useICU equipmentBorder closed to most visitors;all arrivals are tested andquarantined for 14 daysSingaporeThree-phaseplanNo publicly specified 1 m physical distancing and faceindicatorcovering required; governmentmessages have consistentlyemphasised individualresponsibility, although policychanges have generated someinitial public confusionMore than 13 000 PCR tests perday done in June, 2020, with plansto increase to 40 000 tests per day;manual and app-based tracingdoneICUs are well under capacity; toreduce pressure on publichospitals, patients with mildsymptoms are transferred toprivate hospitals or communityfacilities for monitoringBorder closed to most visitors;all arrivals must submit ahealth declaration form, servea 14-day Stay Home Notice,and be testedSouth ancingschemeLevel one applies ifnumber of daily newcases is 50,level two for50–100 cases, andlevel three for 100 casesMass testing at a rate of20 000 PCR tests per day, includingat drive-through and walk-throughstations; records from medicalfacilities, global positioningsystem, credit card transactionhistory, and closed-circuittelevision used to supplementmanual contact tracingOn the basis of a triage system,people with mild disease or whoare asymptomatic aremonitored at residentialtreatment centres; people withmoderate or severe disease arecared for at governmentdesignated hospitalsAll arrivals must submit ahealth declaration form,install a mobile phone app,have temperature screening,testing, and 14-dayquarantine2 m physical distancing and maskwearing practised; governmenthas used transparentcommunication methods tosecure public cooperation,including detailed reporting ofnew cases via websites, mobilephone apps, and text alerts(Table continues on next page)www.thelancet.com Published online September 24, 2020 https://doi.org/10.1016/S0140-6736(20)32007-93
Health PolicyOverallstrategyKnowledge ofinfection statusCommunity engagementPublic-health capacityHealth-system capacityMeasures for border controlAt least 1 m physical distancingrequired, and face coveringrequired in many indoor settings;some controversies haveundermined public support for thegovernmentIn theory, capacity exists to do 200 000 PCR tests per day butthere are major logisticalproblems; centralised testing andtracing systems heavily criticisedand local public-health teamstaking over some tracing; initialattempt to develop an app failed;Scotland and Northern Irelandhave implemented their own appsTemporary hospitals onstandby; routine health servicesgradually resuming whilemaintaining capacity forpatients with COVID-19Arrivals from particularcountries must provide theirjourney and contact details,and self-isolate at home for14 days1·5 m physical distancingrequired, and face coveringrequired where safe distancingnot possible; despite initial publicsupport, some fatigue has set in;inconsistent messages andpolicies across different stateshave caused public confusionContinuous scale up of testingcapacity to over 150 000 PCR testsper day; manual tracing done andnew mobile phone app introducedin June, 2020ICUs are under capacity; initially, People entering or returningto Germany from a countrythere was a scarcity ofdesignated as a risk area areprotective equipmentrequired to quarantine1 m physical distancing requiredand masks recommended foradults and young peopletravelling by public transportwhere safe distancing is difficult;citizens have generally compliedwith government advice andrequirements; the call to join thecollective effort has created ateam spirit that is strongWidespread testing not done;testing reserved for people withsymptoms, health-care workers,and vulnerable populations;manual and app-based tracingdoneSpare capacity varies betweenmunicipalities and hospitals,but the country has hadsufficient health-care personnelto manage the local infectionsituationReopened borders to specifiedNordic regions with low ratesof transmission; arrivals fromoutside these regions aresubject to 10-day quarantineAs of April, 2020, PCR-testingcapacity reached 40 000 tests perday, and capacity has continued toincreaseICUs were over their capacities inmany hospitals at the end ofMarch and April, 2020; otherhospital wards and spaces havebeen adapted to accommodatecritically ill patients; healthworkforce has decreased due tohigh infection ratesFully reopened borders to allcountries from July 1, 2020(inbound travellers will not bequarantined)(Continued from previous page)EuropeEnglandThree-phaseplanR estimated andreportedGermanyTrigger-based Uses R and 7-dayapproachincidence rate per100 000 inhabitantsas indicatorsNorwayLong-termtimetablewith sets ofchanges onspecifieddatesR estimated andreportedSpainFour-phaseplanNo publicly specified 1·5 m physical distancingindicatorrequired, and face coveringrequired where safe distancingnot possibleData have been organised according to the four public-health principles developed by Rawaf and colleagues5 and modified to include additional components suggested in this Health Policy paper. Countries aregrouped by region and organised alphabetically. A more detailed table and full data sources are available in the appendix (appendix pp 1–16). ICU intensive care unit. R reproduction number.Table: Overview of approaches to easing COVID-19 restrictions in nine countries and regions as of September, 2020See Online for appendix4An absence of international consensus is especiallyapparent with respect to face coverings. This differencereflects a combination of cultural norms and evolvingevidence for the effectiveness of face coverings, althoughnot helped by scientific inertia in some countries and inWHO. In Hong Kong, Japan, and South Korea, the habitof mask wearing by people with respiratory conditionswas already widespread before the pandemic (ie, mainlyto protect others from seasonal viruses or as a reaction toair pollution). Other countries have been slower to adoptthis practice. After months of counselling the publicagainst wearing face coverings unless they were unwell,Singapore’s Government made it mandatory for everyoneto wear one outside from April, 2020, and providedreusable cloth masks to the entire population.15 Duringthe past 5 months, Germany and Spain have made itcompulsory to wear a face covering where physicaldistancing is not possible, such as on public transport orin shops. In the UK, face coverings are required in manyindoor settings, such as in community centres.16 Norwayhas recommended face coverings for adults and youngpeople travelling by public transport where safe distancingis difficult. New Zealand has not recommended facecoverings for the general public. Mixed messages andpolicy U-turns regarding face coverings have unfor tunately generated public confusion and challenges toadherence in many countries and regions.Various precautionary measures have been suggestedfor schools and workplaces. In all countries and regions,there was, at least initially, a push toward working fromhome as far as possible, while promoting com pliancewith distancing and hygiene rules for workers whoneeded to be physically present. In Singapore andSouth Korea, workplaces must appoint a manager who isresponsible for implementing precautionary measuresand monitoring employees’ health. In Asian countrieswww.thelancet.com Published online September 24, 2020 https://doi.org/10.1016/S0140-6736(20)32007-9
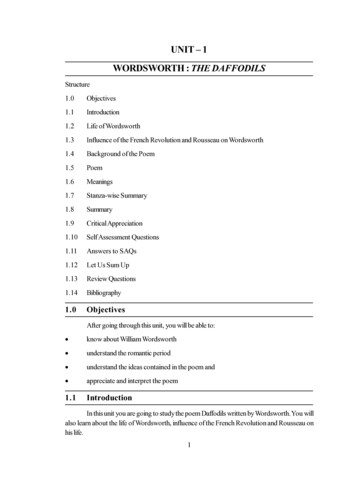
Health Policy2·0 mSafe physical-distancingmeasures1·5 m*1·0 mCommunity engagementand regions, workplaces and schools also practise maskwearing and temperature checking. Schools have largelyfacilitated a staggered return of students, with differentcountries and regions prioritising different groups ofstudents. Singapore, South Korea, and Germany startedwith graduating students attending high schools (eg,aged approximately 15–18 years) to minimise disruptionto education. New Zealand, Norway, and England startedwith younger children, such as children attendingprimary schools (eg, aged approximately 5–12 years).However, it was not always clear whether the primaryfocus was the interests of the child or the desire to enableparents to return to work. Hong Kong and Spain alsostarted with older students, such as students attendinghigher secondary schools (eg, aged approximately15–18 years), as they are presumably better able to followcomplex rules on physical distancing and personalhygiene than are young children. Japan has staggeredattendance, starting with graduating cohorts. Countriesvaried considerably in the extent to which they used thelockdown to prepare schools for reopening and providedresources for online learning.With few exceptions, such as Germany, New Zealand,Norway, Scotland, and South Korea, political leaders havestruggled to secure public trust and thus support forcontinued lifestyle changes. More generally, countrieswith female leaders have done better at securing publicconfidence and adherence to new measures than havecountries with male leaders.17 In England, con troversy sur rounding a trip made during lockdown by a close adviser tothe prime minister has substantially undermined publicconfidence in the government and support for themeasures that it was taking.18 In Hong Kong, continuingpolitical unrest has substantially eroded public trust inthe government, although the community has generallyshown a high level of adherence that could be attributableto lessons learnt from the previous outbreak of SARSin 2003.19 Conversely, the South Korean Government hasadopted a highly transparent communication strategy togain public par ticipation by disclosing detailed infor mationof patients who are infected via government websitesand text alerts, drawing on the country’s past experiencewith MERS.20 The prime minister of New Zealand and thedirector general of health have also won national and inter national praise for communicating firmly yet empa thetically, as shown in formal televised briefings and casuallivestreaming sessions on social media.21COVID-19 has been a reminder of the importance ofprotecting vulnerable populations and addressing healthinequalities, especially in countries that have previouslypaid little attention to these factors. In the UK, as in someother countries, COVID-19 mortality has been dispro portionately high among residents of care homes, Black,Asian, and minority ethnic groups, socioeco nomicallydeprived populations, and workers on low wages.22 Theseinequalities are likely to exist elsewhere, but in manycountries, such as Germany, data are not collected. InIn practice beforeCOVID-19Mask wearing for generalpublicMeasures for reopeningschoolsCountry or regionGermanyHong KongJapanNew ZealandNorwaySingaporeWHO recommends maintaining adistance of at least 1 m (as of April, 2020).However, this recommendation is subjectto interpretation. Countries and regionshave set different standards of what isconsidered a safe distance.Mandated dueto COVID-19Not advised forgeneral public*The purpose of mask wearing differs for two groups of the population:General public and people who cannot physically distance (eg, carers) wearmasks to protect others and prevent asymptomatic spread.Health workers wear masks as part of personal protective equipment forhealth-care service delivery.Starting withyounger childrenStarting witholder studentsStarting withgraduatingcohortsStaggeredattendancestarting withgraduating cohortsSouth KoreaSpainUnited KingdomFigure 2: Key measures in place to allow safe easing of restrictionsDetailed data sources are available in the appendix (appendix pp 1–16). *New Zealand adopts a so-called socialbubble model that allows defined groups of people to have close contact with each other while maintaining safedistancing with other groups.Singapore, migrant workers living in overcrowdeddormitories have constituted almost 95% of close to58 000 confirmed cases.23 In response, the governmenthas improved disinfection regimens, established medicalfacilities onsite, and shielded workers older than 45 yearsby moving them to less dense accommodation than theywere living in.24 All nine countries and regions have alsoheightened practices for infection prevention and controlin care homes, including active testing and isolating ofsymptomatic residents and staff, decreasing or banningvisitors, promoting compliance with hand hygiene, andsupplying protective equipment to these facilities.Economic support to mitigate the effect of the pandemicon communities has been provided by the governmentsof all nine countries and regions, who have announcedsubstantial emergency budgets to help businesses to stayviable, preserve jobs, and alleviate financial burdens onindividuals and households. In the five Asian Pacificcountries and regions, this financial assistance hasincluded one-off cash handouts to the public. Japan, withthe highest emergency spending, amounting to 42% of itsgross domestic product (appendix p 17),25 has handed out 100 000 (approximately US 930) to every resident inthe country. However, unclear legal grounds for payingleave allowance and delayed introduction of the expandedemployment adjustment subsidy scheme have beenheavily criticised. By contrast, the European countrieshave opted for long-term support programmes throughstrengthening their existing social safety nets. In Spain,the COVID-19 crisis has accelerated the approval of ascheme designed to provide a guaranteed minimummonthly income of 462 ( 500) for its poorest citizens.www.thelancet.com Published online September 24, 2020 https://doi.org/10.1016/S0140-6736(20)32007-95
Health PolicyThis scheme is expected to benefit 2·5 million individualsand cost 3 billion annually.26 The UK has also incr
Department of Nursing and Health Sciences, University of South East Norway, Drammen, Norway (E Turk PhD); Medical Faculty, University of Maribor, Maribor, Slovenia (E Turk); College of Medicine and Veterinary Medicine, University of Edinburgh, Edinburgh, UK (D Sridhar PhD) . identified five prerequisites for easing COVID-19 lock-downs and .