Transcription
Trauma Performance Improvement:Simple Steps to Improve OutcomesKathleen D. Martin, MSN, RNRegional Director, Trauma ServicesUCHealth Northern Colorado
Objectives1. Be able to define the components of an Optimal Trauma PIPlan and implement the plan in their trauma center to attainsuccessful verification/accreditation.2. Integrate the new taxonomy classification system as it relatedto PI Events in Iowa trauma centers3. Develop targeted corrective action plans which will result insuccessful resolution Events or identified opportunities forimprovement while enhancing patient outcomes.2
Outline1. Components of an Optimal PI Plan2. Process of identifying PerformanceImprovement Events anddeveloping corrective action plans.3. Categorizing PerformanceImprovement Events in order totarget improvements4. Process to decrease complicationsand unplanned Events.
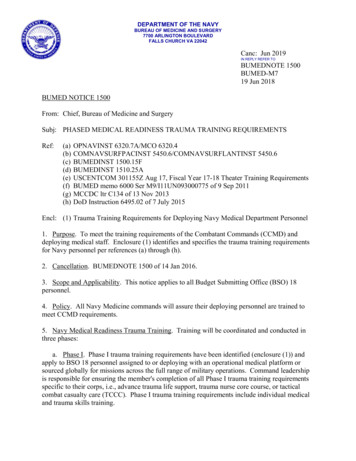
Top 25 WeaknessesHelipadDiversion By lingRegistryOperating RoomsICU/Step DownVolume PerformanceDwell TimeCPG-Clinical Practice GuidelinesDocumentation-EMS run sheetResearchNon Surgical AdmissionED Workup, Resuscitation CareStaffing PhysiciansAutopsyStaffing Trauma ProgramStaffing NursingMassive Transfusion Protocol, Blood BankSolid Organ Injury GradingNursing Trauma CEU certifcation courses and educationTrauma Flow SheetTriage-TTA and ResponseDocumentationPI050100150200250
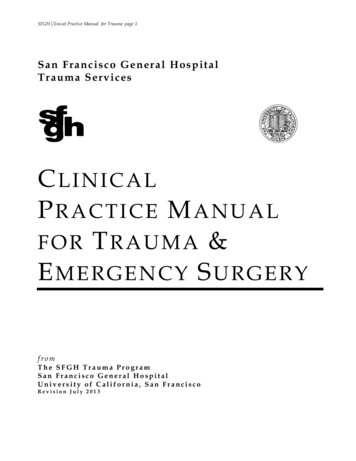
PIPSPI-State/System PIPI-Radiology response timePI-Bench MarkingPI-Dissemenation of PI informationPI-Frequency of MeetingsPI-TimelinessPI-Categorization of DeathPI-PediatricPI-StructurePI-Recognition of issues/ProblemsPI-Pre Hospital PIPI-Documentation/MinutesPI-Loop ClosurePI-Attendance at PI and System PI PI-Process010203040506070
Trauma Outcomes and PerformanceImprovement Course6
Components of an Optimal PI Plan7
Components of Plan1. Goals2. Mission, Vision, Scope, Authority3. Trauma Team Credentialing4. PI Team Members5. Identification of Trauma Patients6. Data Collection7. Sources8. Data Analysis9. Data Management10.Data Validation11.Interrater Reliability12.Concurrent & Retrospective Review8
Components of Plan14.Levels of Review15.Corrective Action Plan16.Event Resolution/Loop Closure17.Multidisciplinary Peer Review Comm18.Trauma Systems/Operations Comm19.Trauma M&M Committee20.References21.Glossary Terms22.Appendix: NTDB Inclusion Criteria23.Appendix: Trauma PI Event Review Form24.Appendix: Level of Review/Determination of Harm25.Appendix: Information Flow and Integration into Hospital PI9
Overview of Trauma PIPS ProcessWhat: Events identification- Audit Filter/Audit Question- Complication/Occurrence- Practice Guideline VariancesWho: (Domain) Patient demographics Source of reported EventWhere: (Domain) Location/Setting Phase/TargetWhen: Date identified and/or Occurred Date of loop closureWhy: (Cause, Impact, Type) Factors Impact (Harm) TypeHow (to fix it):(Mitigation/Prevention) Corrective Actions Levels of Review Mitigation/Prevention Loop Closure
Process of Identifying Trauma PerformanceImprovement and Patient Safety EventsPre-Hospital referralsTransfer CenterEMRHallway communicationEmail referralsMorning reportDaily roundsConcurrent abstractionRegistry data trendsIncident reportsHospital Quality DepartmentAutopsies/ME/CoronerPatient/Family FeedbackRegion/state forumsState or National DesignatingauthorityTQIP reports11
Effective Concurrent Trauma PIPS ProcessImpacts Patient Outcomes at the Point of Care21st centuryConcurrent Point of Care PIIdeally a paperless systemStandard terminologyStore, review, request data at fingertipsEffective user interface and designLaptop wireless entry decreases duplication ofefforts
Process for Monitoring ComplianceComplications: NTDB defined complications whichoccur in the trauma patient, are recorded in the TraumaRegistry. The Trauma PI Program will reviewcomplications for injury or treatment that significantlyaffect patient outcome. The Trauma PI Committeemakes appropriate referrals and recommendations andwill be monitored for trend analysisAudit Filters/Systems Events: All identified Events thatare not provider related are reviewed in the TraumaPerformance Improvement Committees
“Event”Any type of error, mistake, incident, accident,deviation, non compliance, regardless of whether ornot it resulted in patient harm.The goal of the PI process is to identify problems inthe care delivery system that could potentially resultin harm to a patient and resolve them before theyactually result in harm to a patient.
ComplicationsComplications are patient specificDefined across the continuum Deep Vein Thrombosis Myocardial Infarction Pulmonary Embolus Sepsis Ventilator Associated Event Wound infections
Audit Filters Tools that beg the question Not in-and-of-itself evidence that care was sub-optimal A Red Flag that requires you to answer the question“Why was the standard not met?” and “Is there anopportunity for improvement here?” Deviation is either acceptable or unacceptableFilters should make sense for your facility. Theyshould represent circumstances that are likely to beencountered at your hospital and they shouldrepresent Events you know or suspect exist andwould like to improve.
Trauma System Events Absence of EMS recordInadequate pre-hospital airwayNo documentation of FAST examInaccurate FAST exam resultsMissing Trauma Flowsheet/H&PED LOS 2 hours at referring hospitalED dwell time 180 minutesTimely initiation of Massive Transfusion ProtocolClinical practice guideline variation (identify guideline)Tertiary Survey not documented17
Trauma System Events Craniotomy 4 hours of ED arrival for acute/expanding EDH/SDH Administration of antibiotics for an open fracture greater than 1hour after arrival * Positive head CT of patient on anti-coagulation, anti-platelets oraspirin without reversal within 2 hours of arrival Reintubation within 48 hours of extubation (excludes planned return trips to the OR) Unplanned return to the ORUnplanned admission to ICUDelay in DiagnosisMissed InjuryComplications* hospital defined18
Orange Book: Chapter 1619
Trauma Center Events: Orange Book Core Measures Mortality Review (CD16-6)Trauma surgeon response to the emergency department (CD 2-9)Trauma team activation (TTA) criteria (CD 5-13)All TTAs must be categorized by the level of response and quantified bynumber or percentage (CD 5-14, 5-15)Response times, ideally from trauma registry data, for imaging andprocedures, arrival of critical personnel must be monitored.Potential overtriage and undertriage cases should be identified andreviewed monthly (CD 16-7)Trauma patient admissions (NTDS definition) to nonsurgical serviceshould be no higher than 10 percent and must be reviewed monthly(CD 5-18)Direct admission of trauma patients with no trauma consult.Acute transfers outMultidisciplinary trauma peer review committee attendance (CD16-15)20
Trauma Center Events: Orange Book Core Measures Trauma center diversion-bypass hours must be routinely monitored,documented and reported, including the reason for initiating the diversionpolicy, and must not exceed 5 percent (CD3-6) Availability of the anesthesia service (CD 11-4, 11-7, 11-16, 11-18) Delay in operating room availability must be monitored (CD 11-16, 11-18) Rate of change in interpretation of radiologic studies should becategorized by RADPEER or similar criteria (describe theprocess/scoring system used) (CD 11-32, 11-37) Transfers to a higher level of care within the institution (CD 16-8) Solid organ donation rate (defined as number of organ donations dividedby number of potential donors)(CD 16-9) Trauma registry- percentage of completed registry records within 2months of discharge should be determined (the threshold is 80percent).(CD15-6)21
Trauma Center Events: Orange Book CPG Tracking22
Trauma System Performance Improvement23
Trauma System Performance ImprovementA System Performance Improvement Plan in an organizedtrauma care system consists of internal and externalmonitoring and evaluation of care provided through thephases of care and continuum of care.The goal of monitoring is to identify opportunities to reduceinappropriate variations in care and to develop correctiveaction strategies. The effectiveness of the corrective action ismonitored and measured through progressive review cycles.24
Trauma System Performance Improvement:Opportunities for Improvement (OFI) Identify cases for closer review Meant to be helpful Not a judgment of care 25Regional or State metricsUndertriageTime at facility prior to transferCommunication between referringand accepting facilitiesNeed for intubation enroute or onarrival at receiving facilityNeed for chest tube at receivingfacilityMissed injuries at referring facilityInappropriate splinting or C-spinestabilizationCommunication back to referringfacility
Performance Improvement Audits
Levels of ReviewLevels of review can be determined by degree of harm to thepatientA few general definitions to be taken into consideration whenchoosing the highest level of review needed for an Event include:Missed injury - An injury discovered after the patient isdischarged or after death (includes those found on autopsy).Delayed diagnosis - An injury found after completion of the firsttrauma tertiary survey, but before the patient leaves the hospital.27
Impact (Degree of Harm) of EventHarm is defined as injury, suffering, disability or death.The patient safety incident can have an impact on thepatient at various levels, from Mild right through tothe Death of one or more t/help/ALL/Dataset Question References/Patient details/Individual patient/Impact on patient/PD09.htm
Impact/Degree of HarmTemporary - Condition resolves prior to discharge fromthe trauma admission or there is an expectation that it willresolve within 6 months of the EventPermanent - Condition is present at discharge and doesnot resolve within 6 months of the complication or Event, isnot expected to resolve, and may or may not be lifelong.29
Degree of HarmNo Harm – Standard of care provided with some deviationswith no impact to the patientNo Detectable Harm – Event occurred but did not reach orimpact patient; no treatment
Degree of HarmMinimal Harm – Impact to patient, is symptomatic,symptoms are mild, loss of function is minimal orintermediate but short term, and no or minimal intervention(extra observation, investigation review, minor treatment) isrequired
Degree of HarmModerate Harm – Patient outcome is symptomatic,requiring an intervention (e.g. operative intervention,therapeutic treatment), and increase in the length of stay, orcausing long term loss of function; requires high level ofcare; expected to resolve prior to discharge
Degree of HarmSevere Harm – Patient is symptomatic, requiring life-savingintervention or major surgical/medical critical careintervention, shortening life expectancy or causing majorpermanent or long term harm or loss of function; error injudgment, deviation from practice, system delays; impactquality of care; quality of life
Degree of HarmDeath – death was caused or brought forward by the Event
Trauma Performance ImprovementPrimary ReviewEvent Identification Referral Facility Care Transport Team ICU/Acute CareComplication/Audit FilterReviewSecondary Review Rehab or post dischargeTMD, TPM, TPIC, TRN, TREventsElevated toHospital PICMonthlyTertiary ReviewTraumaPeer ReviewMonthlyTrauma Systems/CommitteeMonthlyTrauma M&MWeeklyPre-Hospital elingTrend for FutureReportingGuideline/Policy DevelopmentPI Team Project
Levels of ReviewPrimary Review Event identification Validation of Event Drill down on contributing factors System Event or patient Event Degree of harm Immediate resolution Feedback to those involved Management Process Written in PIPS Plan- System Events with No Harm to Patient-TPM Manages- Patient Impact with Harm–TMD Must Address- Physician Events–TMD Must Address
Levels of ReviewSecondary Level of Review TMD Screening – Triage Review Impact, Level of Harm, Type of Event, Domain TMD confirms level of harm Triage Events for review Referrals PI Workgroup Request additional data CloseALWAYS SCREENED BY TMD
Levels of Performance ReviewSecondary Review Review by TPD or TPM/PI Coordinator concurrently- (weekly or biweekly) Triage Events to the next level:- Refer to Trauma Multidisciplinary Review- Refer to Trauma M & M (clinical non-death)- Refer to Trauma Mortality Review (death)- Refer to Hospital PI Committee(s)Trauma PI can set the tone for PI in the entire health care facility
Levels of ReviewTertiary Level of Review Trauma Multidisciplinary Peer Review Trauma M & M Clinical Management Guidelines- Compliance tracking- Concurrent tracking in registry- Variance analysis reports- Provider specific Financial Outcome Review with Hospital Finance
Levels of ReviewTertiary Review Provider peer discussion Reason for event referral – Capture in minutes Capture essence of the discussion Discussion of how to prevent Contributing factors Corrective actions recommended Review with TMD Implement action plan
Levels of ReviewQuaternary Review External Care Forums- External Peer Reviewo Region, State, Expert- Hospital Medical Staff Peer Review- Other Hospital Review- Affiliate Hospital Review Mock Site Surveys by subject matter experts
Performance Improvement Audits
Patient Safety Taxonomy: Impact/Degree of Harm
Patient Safety Taxonomy: Type
Patient Safety Taxonomy: Domain
Patient Safety Taxonomy:Cause/Contributing Factors
Patient Safety Taxonomy: Prevention Strategy
Performance Improvement Audits
Developing Corrective Action Plans Provider-related Events actions: Education Counseling Change in privileges System-related Events actions: Guidelines & protocols Education Enhanced resources ( )49
Mitigation Action VS Preventive ActionMitigation Action50
Corrective Action Mitigation5 Step ProcessIDENTIFY Identify the Opportunity for Improvement and enter into *PI tracking system Associate system related Event to a patient; link the Corrective Actions to future patientsANALYZE Document and analyze the current state of the ‘Event’ using registry data, benchmarks Identify contributing factors: System, Provider, PatientACTION Appoint a PI Team ( 5) and SME to brainstorm corrective actions & mitigation strategies Document PI Team Charge (goals) and present recommendation on specific trouble areasIMPLEMENT Design a roadmap to support implementation with timeline for improvement Mange the implementation across the continuumEVALUATE Evaluate loop closure with metric driven criteria Monitor for set time (really depends on how often the Event occurs: 1x/day, month, yearDOCUMENT Enter ALL follow up actions in the Corrective Action area, with date of completion Attach all Emails, letters, draft or completed CPGs, copies of Evidence Base Practice
Failed Corrective Action Did the corrective action address only the symptoms of a problemand fail to address the root cause? Was a corrective action for a known deficiency not implemented ordisregarded? (Inaction when addressing safety is not acceptable) Did management decide to implementlower cost or otherwise differentcorrective actions that didn’tadequately fix the previouslydiscovered Event?
Opportunities for Improvement ED Nursing DocumentationIntegration of Trauma PI into Hospital PIPhysician Attendance at Peer ReviewUndertriageGeriatric TraumaOB Trauma ActivationPediatric Trauma Activation (adult trauma center)Inter-rater Trauma Registry validationF.A.S.T. ultrasound validation processSimulated Trauma Activation TrainingPTSD trainingDecrease direct admits from referring facilities53
Corrective Action Mitigation5 Step ProcessIDENTIFY Identify the Opportunity for Improvement and enter into *PI tracking system Associate system related Event to a patient; link the Corrective Actions to future patientsANALYZE Document and analyze the current state of the ‘Event’ using registry data, benchmarks Identify contributing factors: System, Provider, PatientACTION Appoint a PI Team ( 5) and SME to brainstorm corrective actions & mitigation strategies Document PI Team Charge (goals) and present recommendation on specific trouble areasIMPLEMENT Design a roadmap to support implementation with timeline for improvement Mange the implementation across the continuumEVALUATE Evaluate loop closure with metric driven criteria Monitor for set time (really depends on how often the Event occurs: 1x/day, month, yearDOCUMENT Enter ALL follow up actions in the Corrective Action area, with date of completion Attach all Emails, letters, draft or completed CPGs, copies of Evidence Base Practice
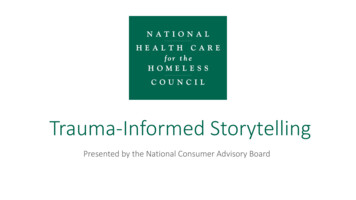
Nursing Documentation on Trauma FlowsheetGoal Statement: Improved Trauma Flowsheet DocumentationCompliance will be at 95% within 6 months Analyze each areas of weakness Vital Signs Physical Assessment Response to InterventionsTrauma FlowsheetFocus GroupJUL 2017MAR 2018unk97%42% Redesign FS with Key Area shadingPhysical Assessment CheckboxesResponse to Intervention CheckboxesEducation/Train the Trainer/Training75%Implement Real TimeAudit (end of each shift)Audit tied to Staff Evaluations 95% compliance with key metrics
Roadmap for Corrective ActionNov 2017CorrectiveAction PlanDevelopedJan 20158Policy,EducationPreventionFeb 2018ImplementPolicy afterTrainingApril 2018Analyze Metricdata and reportto CommitteeMarch 2018Tracking Metricto MeasureComplianceDeficiency: Trauma PI Process does not identify opportunities for improvement or integrate with the hospital quality departmentReceive Report ofDeficiencyForward to TraumaMedical Director9.Individually presentObjectives to allstaffAnalyze andValidateDeficiency2.Appoint TraumaWorkgroupHospitalQualityDepartmentTrauma System CommitteeTraumaWorkgroupTraumaProgramManagerTrauma MedicalDirector‘C’ Suite03/02/20153.Draft Goals andObjectives4.Present Goals andObjectives toDepa rtmentManagers6.Refine Goa ls andObjectives bas ed onfeedback8.Present Vision andGoals to all staff7.Approve Goals andObjectivesPrioritize ObjectivesGoals a nd Objectives(final)5.Provide feedback
Corrective Action: Physician Attendance 50% Physician attendance at Peer Review Committee or Systems Meeting was noted asdeficiency/weakness at verification reviewIDENTIFY Review the attendance logs; validate it is not a sign in issue; assess if alternate attended Query liaisons for rationale; If attendance is a Medical Staff Bylaw; official appointment letters Assess the suitability of the Liaison and commitment to trauma program; Committeeappointment letter from COS, Chair, CEOANALYZEACTION Change the meeting time; combine Peer and System back to back; Serve lunch/breakfast/pizza Set up reminders in Outlook for all attendees; call/text cell on the day of the meeting; offer CME!! Increase Participation: Establish roles for each participant, reporting calendar for eachdepartment, and hold accountable Provide education to all Committee participants and liaisons as to the changes and strategiesIMPLEMENT Sign in sheets monitored on entrance and exit; ‘Read Receipt’ when minutes are E-distributed Evaluate compliance with attendance; 50% minimum goal; 100% expectation Disseminate minutes with signature of review when there is absence Monitor for set time; loop closure with metric driven criteria; show integration into Hospital PIEVALUATE process/Bylaws Process
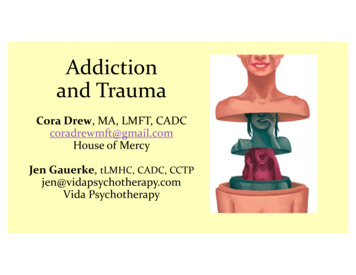
Over and Under Triage ReportMarch 2017Arrival Year-Month:2013-03HighestSecond LevelConsultNo AlertTotalOver TriagedUnder TriagedISS 1 to 9 ISS 10 to 14 ISS 15 to 24 ISS 25 Total with ISS Not Valued ISS30017202100000223Number of Patients: 5Percentage: 83.33%Number of Patients: 5Percentage: 22.73%0600033002228009
Over and Under Triage ReportJuly 2017Arrival Year-Month: ISS 1 to ISS 10 to9142013-07ISS 15 to24ISS Total with ISS Not Valued ISS25Highest300250Second Level100010Consult300030No Alert14000145Total2100223Over TriagedNumber of Patients: 3Percentage: 60.00%Under TriagedNumber of Patients: 0Percentage: 0.00%
60
Let’s Talk .What are the biggest Events1.in your trauma Transfers/TransportDelaysComplications2.3.4.5.What data do you need to analyze the Event?
Summary Don’t try to run before you can walkWhat is the significance of the event?Take Events through Levels of ReviewTriage Events based upon Degree of HarmDelay to OR with a poor outcome: SeverePoor compliance with ED Nursing documentation: Minimal Document each step of the process in your Trauma PIPS Plan!62
Thank you!Questions?Kathleen.martin2@uchealth.org63
Registry. The Trauma PI Program will review complications for injury or treatment that significantly affect patient outcome. The Trauma PI Committee makes appropriate referrals and recommendations and will be monitored for trend analysis Audit Filters/Systems Events: All identified Events that are not provider related are reviewed in the Trauma