Transcription
Bariatric SurgeryClaims Data Snapshot
Introduction This publication contains an analysis of the aggregated data from MedPro Group’s casesclosing between 2011-2020 in which an bariatric surgeon is identified as the primaryresponsible service. A malpractice case can have more than one responsible service, but the “primary responsibleservice” is the specialty that is deemed to be most responsible for the resulting patient outcome. Note: case volume is low ( 100) and any conclusions should take this fact into consideration. Our data system, and analysis, rolls all claims/suits related to an individual patient eventinto one case for coding purposes. Therefore, a case may be made up of one or moreindividual claims/suits and multiple defendant types such as hospital, physician, or ancillaryproviders. Cases that involve attorney representations at depositions, State Board actions, andgeneral liability cases are not included. This analysis is designed to provide insured doctors, healthcare professionals, hospitals,health systems, and associated risk management staff with detailed case data to assistthem in purposefully focusing their risk management and patient safety efforts.
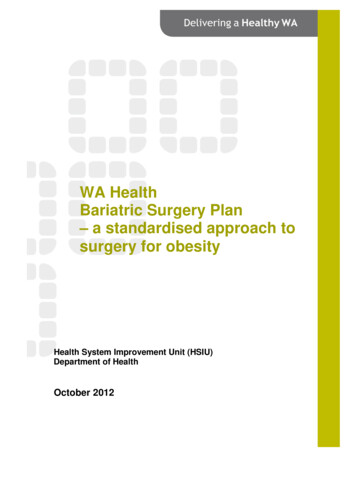
Major allegations & financial severity50%% of case volume and total dollars paid45%44%40%35%35%30%35%30%27%Case volume25%Total dollars paid*20%15%12%9%10%8%5%0%Improper performanceof surgeryImproper managementof surgical patientDiagnosis-relatedOther**Multiple allegation types can be assigned to each case; however, only one “major” allegation is assigned that best characterizes theessence of the case. Performance of surgery and management of surgical patient allegations account for almost 80% of bariatric surgerycase volume. Although overall diagnosis-related case volume is low, these cases closed with indemnity paid more often, thus accountingfor the disproportion of dollars paid. Management-related cases tend to be more complex to defend than procedural cases, and on averageare more expensive to resolve.MedPro Group closed cases, bariatric surgery as responsible service, 2011-2020 (N 100); *Total dollars paid expense indemnity; **Other includes allegations for which no significant case volume exists
Surgical & diagnosis-related allegations Surgical performance casesinvolve a variety of procedures, mostcommonly gastric sleeves. Recognizing and managing knowncomplications, including bowelperforations, lacerations andslippage of gastric bands arerecurring themes throughout thesecases. Poor technique and clinical decisionmaking regarding the mostappropriate procedure for the patientare additional issues identified. Cases involving the managementof surgical patients, including pre-,intra-, and post-operatively, are oftenrelated to the surgeon’s response todeveloping complications such asbowel perforations. While complications of proceduresmay have been the result ofprocedural error, the failure to timelyrecognize and/or monitor/managethe issue prevents the opportunity forearly mitigation of the risk of seriousadverse outcome. These management cases tend toresult in the most serious outcomes,and include patients who developedsurgical complications such aspulmonary emboli and infections.MedPro Group closed cases, bariatric surgery as responsible service, 2011-2020 Diagnostic cases primarily involvedelays in diagnosing post-operativecomplications such aspunctures/lacerations and infections. These cases reflect narrowdiagnostic focus, inadequate patientassessments, especially assymptoms are escalating, and failedcommunication among providers,particularly when reporting and/orfollowing through on diagnostic testresults.
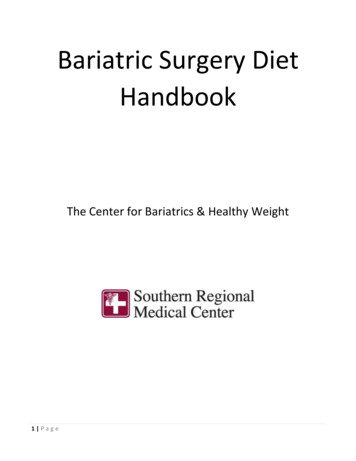
Clinical severity*Clinical severity categoriesSub-categories% of casevolumeEmotional Injury OnlyLOWMEDIUM1%DefinitionsMental distress or suffering that is generally temporary; includes HIPAA violations,discrimination, involuntary stayTemporary Insignificant InjuryLacerations, contusions, minor scars or rash, where no delay in recovery occursTemporary MinorInfection, fracture set improperly or a fall, where recovery is complete but delayedTemporary Major46%Burns, drug side effect; recovery delayedPermanent MinorLoss of fingers or loss or damage to organs; includes non-disabling injuriesSignificant Permanent InjuryDeafness, loss of limb, loss of eye or loss of one kidney or lungMajor Permanent InjuryHIGHParaplegia, blindness, loss of two limbs or brain damage53%Grave Permanent InjuryQuadriplegia, severe brain damage, lifelong care or fatal prognosisDeathDeath20%% of case volume resulting in patient deathTypically, the higher the clinical severity, the higher the indemnity payments are and the more frequently payment occurs.MedPro Group closed cases, bariatric surgery as responsible service, 2011-2020; *National Association of Insurance Commissioners rating scale5
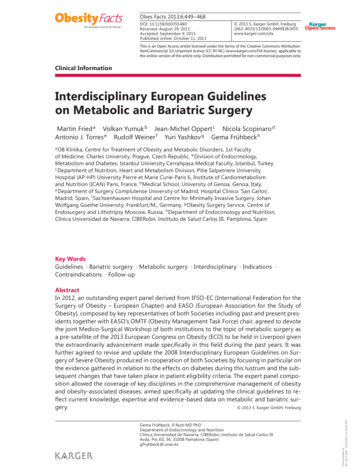
Claimant type & locationInpatient: 67%Ambulatory: 30%Location% of case volumeInpatient OR51%Patient room/ICU24%Office/clinic13%Ambulatory surgery8%Emergency department3%Other*1%Emergency: 3%MedPro Group closed cases, bariatric surgery as responsible service, 2011-2020; *Other includes locations for which no significant case volume exists6
Contributing factorsContributing factors are multi-layered issues or failures in the process of care that appear tohave contributed to the patient outcome, and/or to the initiation of the case, or had a significantimpact on case resolution.Multiple factors are identified in each case because generally, there is not just one issue thatleads to these cases, but rather a combination of issues.Contributing factors reflect both provider and patient issues, but are not programmaticallyassigned to specific individuals. They denote breakdowns in technical skill, clinical judgment,communication, behavior, systems, environment, equipment/tools, and teamwork. The majorityare relevant across clinical specialties, settings and disciplines; thus, they identify opportunitiesfor broad remediation.CRICO Strategies. (2020). The Power to Predict: Leveraging Medical Malpractice Data to Reduce Patient Harm and Financial Loss. Retrieved from lBenchmark-Reports/The-Power-to-Predict
Top* contributing factor categories by allegation100%94%100%Improper performanceof surgery90%% of case volume with these factors81%Improper managementof surgical ore than one factor per case is usually present, therefore totals will not equal 100%.MedPro Group closed cases, bariatric surgery as responsible service, 2011-2020; *Those present in / 10% of case volume in at least one allegationClinicalsystems
Contributing factors: most common factor details in bariatricsurgery casesAdministrativeInadequate staff training/education, physician coverage, credentialing issues, failure to followpolicies/proceduresBehavior-relatedPrimarily involves patient non-adherence to follow-up and with treatment regimen, and patientdissatisfactionClinical judgmentInadequate assessments; these include failures to appreciate/reconcile patient signs/symptoms/testresults (sometimes leading to premature discharge from care), inadequate history/physical,failures/delays in seeking consults, narrow diagnostic focus, delays in ordering diagnostic testingCommunicationSuboptimal communication among providers regarding patient condition, inadequate informed consentdiscussions and failures to manage patient expectationsClinical systemsReflective of delays in scheduling/performing/reporting diagnostic testing, and general failures in thesystem for patient care (including patient ack of documentation leading to difficult defense of casesTechnical skillRecognition/management of known complications, poor technique, procedural inexperienceMedPro Group closed cases, bariatric surgery as responsible service, 2011-2020
Factors predictive of cases closing with indemnity paidCRICO Strategies analyzed 37,000 cases* to determine which breakdowns in health careprocesses indicate the highest odds of a case closing with an indemnity payment.AdministrativeClinical JudgmentDocumentationFailure to have or followa policy or protocolPatientassessment failuresAbsent or insufficientdocumentation2.451.851.76ODDS RATIOODDS RATIOODDS RATIO*All specialties, closed between 2014-2018; CRICO Strategies. (2020). The Power to Predict: Leveraging Medical Malpractice Data to Reduce Patient Harm and Financial Loss. Retrieved nnual-Benchmark-Reports/The-Power-to-Predict; MedPro Group is a member of CRICO Strategies’ Community Benchmarking System (now known as CandelloCompare) which represents 30% of all US MPL cases.
Bariatric surgery: where to focus your efforts Ongoing evaluation of procedural skills and competency with equipment is critically important. Conduct a thorough assessment of the patient pre- and post-operatively. Ensure that all testing and specialty evaluations are available for review prior to induction; in an ambulatory setting, these details might not always beas readily available as in the inpatient setting. Maintain a consistent post-procedure assessment process. Communicate with each other. Actively collaborate with other members of the patient’s surgical care team – including all operating and recovery room staff. Coordinate the steps ofthe patient’s care, including post-operatively. Ensure nursing staff have open lines of communication for notifying surgeons of situations such as non-response to post-op pain control, repeatedpatient complaints about discomfort, and changing vital signs. Talk also to the patient/family, elicit a comprehensive patient history and conduct a thorough informed consent with the patient. Understand that clinical systems issues encompass breakdowns in the process for safe patient care. This factor includes scenarios when there are multiple providers involved in post-operative decision-making; failure to designate the provider in charge– be it the surgeon or the medical specialty physician – can lead to compromised treatment. Engage patients as active participants in their care. Consider the patient’s health literacy and other comprehension barriers. Recognize that patient satisfaction with treatment outcomes can be influenced by a thorough informed consent and education process. Document. The operative record is critically important for detailing the pre-operative patient assessment, intra-operative steps, and post-operative sequence ofevents. Discrepancies or gaps in the details/timing make it much more difficult to build a supportive framework for defense against potentialmalpractice cases.
MedPro Group dataMedPro is partnered with Candello, a national medical malpractice data collaborative and division of CRICO, the medical malpracticeinsurer for the Harvard-affiliated medical institutions.Derived from the essence of the word candela, a unit of luminous intensity that emits a clear direction, Candello’s best-in-classtaxonomy, data, and tools provide unique insights into the clinical and financial risks that lead to harm and loss.Using Candello’s sophisticated coding taxonomy to code claims data, MedPro is better able to highlight the critical intersectionbetween quality and patient safety and provide insights into minimizing losses and improving outcomes.Leveraging our extensive claims data, we help our insureds stay aware of risk trends by specialty and across a variety of practicesettings. Data analyses examine allegations and contributing factors, including human factors and healthcare system flaws that result inpatient harm. Insight gained from claims data analyses also allows us to develop targeted programs and tools to help our insureds minimizerisk.DisclaimerThis document should not be construed as medical or legal advice. Because the facts applicable to your situation may vary, or the laws applicable inyour jurisdiction may differ, please contact your attorney or other professional advisors if you have any questions related to your legal or medicalobligations or rights, state or federal laws, contract interpretation, or other legal questions.MedPro Group is the marketing name used to refer to the insurance operations of The Medical Protective Company, Princeton Insurance Company,PLICO, Inc. and MedPro RRG Risk Retention Group. All insurance products are underwritten and administered by these and other BerkshireHathaway affiliates, including National Fire & Marine Insurance Company. Product availability is based upon business and/or regulatory approvaland may differ between companies. 2022 MedPro Group Inc. All rights reserved.12
MedPro advantage: online resourcesFind us online atwww.medpro.com/dynamic-risk-toolsTools & resourcesEducational opportunitiesFollow MedPro on LinkedIn and Twitter(@MedProProtector)Education Materials and resources to educate followersabout prevalent and emerging healthcare risksAwarenessConsulting informationVideoseRisk Hub Cybersecurity Resource Information about current trends related topatient safety and risk managementPromotion Promotion of new resources and educationalopportunities
MedPro Group closed cases, bariatric surgery as responsible service, 2011-2020; *National Association of Insurance Commissioners rating scale 5 Clinical severity categories Sub-categories % of case volume Definitions LOW Emotional Injury Only 1% Mental distress or suffering that is generally temporary; includes HIPAA violations,