Transcription
COMMUNITY PROFILE REPORTPuget Sound AffiliateSusan G. Komen for the Cure 112 Fifth Avenue NorthSeattle, Washington 98109www.komenpugetsound.org
AcknowledgementsThe Komen Puget Sound Affiliate Community Profile (CP) Update could not have been written withoutthe dedicated research and assistance of many individuals and organizations. We deeply appreciate allof the time and effort by the following contributors:Community Profile TeamKathleen E. Malone, PhD, Fred Hutchinson Cancer Research Center (Lead CP Team Member)Michael A. Hunter, MD, Evergreen HospitalSheila Edwards Lange, PhD, University of WashingtonLori K. Nomura, Attorney at Law, Foster PepperChisula Chambers, MPH, PS Komen InternElisa Del Rosario, Grants Program Manager, Puget Sound AffiliateData Expert PartnersMahesh Keitheri Cheteri, PhD, Washington State Cancer Registry, Dept. of HealthDavid Doody, MS, Fred Hutchinson Cancer Research CenterLinda Gunnels, MSPH, Community Wellness and Prevention, Dept. of HealthChristopher I. Li, MD PhD, Fred Hutchinson Cancer Research CenterSources of Exploratory DataPS Komen also wishes to thank these individuals and organizations for their assistance in conveningand/or facilitating focus groups with Asian Indian, Pacific Islander and Vietnamese women:Grace Grymes Chapman, ARNP, West Seattle Health Clinic, PS Komen InternAsia Pacific Cultural Center: Faaluaina “Lua” PritchardAsian Counseling & Referral Service: Kim Co, Chau Dang, Hanh Lai, Jeannie NguyenGurudwara Singh Sabha of Washington, Renton: Jasmit Singh, Molina Kochar, Sutinder Kaur Chawla,Anita UppalInternational Community Health Services: Fa’amaile Frost and Minh Nguyen WymanSamoan National Nurses Association: Jackie LeSageSikh Centre of Seattle (Bothell): Balwant and Gurjeet Aulck; Arvind Mann; Sippy Hira; Daljit GrewalAppreciation is also extended to the following organizations and individuals who served as keyinformants for target communities or key issues:African American: Worship in Pink Ambassadors -- Brittany Blue, Marilyn Calbert, Doris Harris, LovieIvey, Mona Lake Jones, Donna Manier, Lorraine Rose-Drayton, Velma Ragsdale, Joycelyn Thomas,Janet White, Jeri White, Valerie WilsonHispanic/Latina: Antoinette Angulo, Rosa Borja, Kendall Dodd, Agueda Fernandez-Webster, KarlyGarciaAmerican Indian/Alaska Native: Christina Hicks, Roberta Kimberly, Teresa Garrett Hill, Rose James,Elizabeth Siegel and participants of the 2010 Inter-tribal Breast Cancer Awareness WalkCounties of Interest: Clallam County -Nancy Adams, Jack Slowriver; Skagit & Whatcom Counties- BeckyJones, Cary Kaufman, MD, Linda McCarthy; Thurston County/SW WA – Melodie Petersen, KathleenPyper, Cobie WhittenPublic Policy/WBCCHP: Susie Tracy, Northwest Advocates and Pama Joyner, Dept. of Health2
Table of ContentsAcknowledgements . 2Table of Contents . 3Table of Tables . 4Executive Summary . 5Introduction . 5Statistics and Demographic Review . 5Health Systems Analysis. 6Qualitative Data Overview . 7Conclusions . 7Action Plan. 8Introduction . 10Purpose of Report . 10Affiliate History . 10Organizational Structure . 10Description of Service Area . 11Breast Cancer Impact in Affiliate Service Area. 14Methodology . 14Overview of the Affiliate Service Area . 14Communities of Interest . 27Conclusions . 28Health Systems Analysis of Target Communities . 29Overview of Continuum of Care. 29Methodology . 29Overview of Community Assets . 30Legislative Issues in Target Communities . 35Key Informant Findings . 36Conclusions . 36Breast Cancer Perspectives in the Target Communities . 38Methodology . 38Review of Qualitative Findings . 39Conclusions . 43Conclusions: What We Learned, What We Will Do . 45Review of the Findings . 45Action Plan. 45References. . . . . .473
Table of TablesTable 1. Estimated Race/Ethnicity Population.16Table 2. Estimated 2009 Family Income by County/Region . . .18Table 3. Estimated 2009 Insurance by County/Region . 18Table 4. Incidence of newly diagnosed invasive breast cancer in womenby race/ethnicity for 2003-2007 -- in the Service Area . . 19Table 5. Distribution of stage at breast cancer diagnosis by race/ethnicityamong cases diagnosed in 2003-2007 -- in the Service Area .20Table 6. Distribution of stage at diagnosis by Asian/Pacific Islander ethnicityamong cases diagnosed in 2003-2007 -- in the 13 counties of the ServiceArea covered by the SEER cancer registry . .20Table 7. Five-year cause-specific survival from invasive breast cancer byrace/ethnicity among cases diagnosed in 1997-2001 and 2002-2006 –in the 13 counties of the Service Area covered by the SEER registry. .22Table 8. Screening rates for women age 40-75 by Race/Ethnicity-- in Service Area . 23Table 9. Incidence rates of newly diagnosed breast cancer (in situ and invasive)in women by county and region for 2003-2007 -- in the Service Area .23Table 10. Proportional distribution of stage of breast cancer at diagnosis in2003-2007 by county and region -- in the Service Area . 25Table 11. Five-year cause-specific survival from invasive breast cancer forcases diagnosed 2002-2006 by county -- in the 13-county area covered by CSS .274
Executive SummaryIntroductionThe Susan G. Komen Foundation began as a promise between two sisters to end breast cancerforever. Susan Goodman Komen was diagnosed with breast cancer at the age of 33 and diedthree years later. Ms. Komen’s younger sister, Nancy Goodman Brinker, founded the foundationin 1982. The Komen Puget Sound Affiliate was founded in 1993 to forward the mission of ournational organization – to save lives and end breast cancer forever by empowering people,ensuring quality of care for all and energizing science to find the cures. Since its inception, theKomen Puget Sound Affiliate has invested nearly 23 million in local nonprofit, tribal andgovernment agencies that provide breast health and breast cancer services to medicallyunderserved residents of our 16-county service area (Service Area).The purpose of the community profile is to take a timely assessment of the state of breast cancerin the Affiliate’s Service Area. This report examines statistics, services and communityperspectives to identify disparities, gaps in service and barriers to care that prevent women wholive in our community from accessing, early detecting and surviving breast cancer. This reportwill be used to set the Affiliate’s priorities, goals and objectives in its strategic planning, grantmaking and educational efforts to ensure that we are meeting our promise to save lives.Statistics and Demographic ReviewThe majority of data used in the demographic section of the community profile was obtainedthrough Thomson Reuters 2009, a National Komen commissioned custom module ofestimated demographic data for the Affiliate’s Service Area. Statistical data on breast cancerincidence and mortality was obtained from the Washington State Cancer Registry and the CancerSurveillance System, the Surveillance Epidemiology and End Results (SEER) Program cancerregistry serving 13 of the 16 counties in our service area that is funded by the National CancerInstitute.The Service Area as a whole, with 69 percent (or 4,607,327) of the total state population, is thedensest and most racially/ethnically diverse area in the state. Within the Service Area, theGreater Metropolitan areas of King, Snohomish, Pierce and Kitsap counties had the greatestnumber of residents (78.6 percent or 3,623,557) and the greatest diversity (25 percentminorities). While King, Snohomish and Pierce counties have the greatest numbers of uninsuredresidents and families living below the poverty level, the counties in the southwest region of thestate have the highest percentages of families below the poverty line and individuals who areuninsured.Breast cancer is the most frequently diagnosed cancer among Washington State women and thesecond leading cause of cancer death. Washington ranks 12th highest in incidence and 35thhighest in mortality in the country.Higher proportions of cases diagnosed at advanced stage and/or lower proportions diagnosed atthe in situ stage are likely indicators of insufficient rates of mammogram screening. AfricanAmerican, Hispanic, American Indian/Alaskan Native (AI/AN), and Vietnamese, Pacific5
Islander and Asian Indian/Pakistani women had the highest proportions of breast cancers thatwere advanced stage at diagnosis. African American, AI/AN, Asian Indian/Pakistani andPacific Islander women have the lowest five year rates of survival among all the ethnic and racialgroups in the Service Area, with the majority of these women living in King, Pierce andSnohomish counties.Lewis and Pacific counties had the highest proportion (both at 32 percent) of breast cancer casesdiagnosed with advanced stage in the Service Area. Compared to the statewide average (20percent), several counties had considerably lower proportions of cases with an in situ diagnosis –Pacific (12.4 percent), Clallam (13.7 percent), Grays Harbor (15.6 percent) and Thurston (17.2percent).Seven counties (of the 13 with breast cancer survival data) had lower than average five yearsurvival rates: Mason, Grays Harbor, Jefferson, Clallam, Skagit, Whatcom and Pierce.It is important to note that the three most densely populated counties (King, Pierce andSnohomish), although not the worst performers in terms of proportions of cases with advancedstage at diagnosis and survival, carry some of the heaviest burdens in our service area because ofthe sheer large numbers of women diagnosed with advanced stage or dying from breast cancer.With respect to utilization of breast cancer screening, 76 percent of Washington women over age40 who were surveyed reported having a mammogram in the past two years, which mirrors thenational average. Of the 16 counties in the Service Area, the five counties with the lowestscreening rates were Wahkiakum (48.4 percent screened), Lewis (64.7 percent), Grays Harbor(70.1 percent), San Juan (71.9 percent) and Clallam (72.3 percent). American Indian/AlaskanNative women had the lowest screening rate at 54 percent reporting having a mammogramwithin the past two years.Health Systems AnalysisIdentification and updating of breast cancer resources were focused more on the “new” countiesand populations not previously identified as areas of interest in the 2009 Community Profile.These are Clallam, Whatcom, Skagit and Thurston counties and Pacific Islander and AsianIndian/Pakistani women. For these “new” counties identified for further exploration, snapshotsfrom the 2007 report were sent to key informants in those counties to confirm accuracy and forany additions or changes. These snapshots include information on breast health resources andgaps in services in their community.For the previously identified counties of interest in the 2009 report – Greater Metropolitancounties of King, Pierce and Snohomish and Southwestern counties (Grays Harbor, Lewis,Pacific and Mason) – key informants from those communities were asked to verify/updatestatements from the last report.Western Washington is home to many state-of-the-art medical facilities, mammography centers,and cancer treatment centers; however, the majority of services are clustered in the GreaterMetropolitan (Seattle/Tacoma) area. The challenge in this region is not so much the lack offacilities and resources, but rather disparities in utilization or access. The focus must be on6
ensuring that women are knowledgeable about and can access existing resources, and thatproviders and programs have the capacity to meet the demands for breast cancer screening andtreatment of low-income residents who require no-cost care.Many women living in the Southwest Washington region struggle with lack of information aboutbreast health resources, transportation and poverty. Women’s health care is very fragmented andtypically involves sending a woman to several providers when she is diagnosed with breastcancer. Communication can be difficult and women may get lost in the system.Qualitative Data ReviewThe Affiliate gathered input from key stakeholders whose connection to residents of targetedgeographic areas and to racial and ethnic communities and their issues would be helpful to thecommunity profile process. Key informant interviews and/or focus groups were conducted to getperspectives from those living and working in the target areas and populations. Participantsincluded community leaders, employees of county health departments, representatives from localhospitals, WBCCHP Prime Contractors and subcontractors, breast cancer survivors and healthcare providers.Financial barriers and lack of health care insurance are the most commonly reported reasons whywomen of color don’t get screened. This is followed by the lack of awareness or prioritization ofbreast health or preventive health care practices in general. Myths about breast cancer andmammograms, as well as cultural taboos, fears and modesty issues were all commonly cited asbarriers to screening among women of color.There are many concerns among racial and ethnic minorities about trust, and the intentions of thehealthcare system. Based on their past history, this is especially true for African American andNative American women who may fear experimentation or doubt the intention of healthcareproviders to care for people of color. Undocumented Hispanic women often fear theconsequences of entering a government-supported program, doubt the actual anonymity of careand may find questions from providers to be intrusive and alarming.ConclusionsBased on detailed analyses of the breast cancer statistics, demographic information, healthsystem resources and qualitative data, we identified areas of need:African American, Hispanic, American Indian/Alaska Native, Vietnamese, PacificIslander and Asian Indian women need early detection services and support duringtreatment.Lewis, Pacific, Grays Harbor and Mason counties in Southwest Washington continue toneed increased access to quality and convenient breast cancer treatment as well as earlydetection services.King, Pierce and Snohomish counties have the greatest burden of women in need ofservice, particularly women of color; women living in these counties need moreinformation about available resources, as well as increased capacity for screening, patientnavigation and treatment support.7
A common theme heard among all counties and populations was the need to increaseawareness about breast health and about available resources and the need to address gapsin transportation, particularly in rural areas, and interpretation services to addresslanguage barriers of racial and ethnic minority women.However, the current economic climate has resulted in tremendous increase in demand for freeor low cost breast health services. The Affiliate does not have adequate resources to meet thisdemand, but is committed to working with our partners to preserve and protect current servicesand will continue our commitment to increase funding to invest in proven effective life-savingstrategies.Action PlanGoal: Increase breast cancer screening, patient navigation and treatment support servicesoffered in Grays Harbor, Lewis, Pacific and Mason counties, particularly for low-income,Hispanic and American Indian/Alaska Native women.Objective 1 – By March 2014, increase investments in effective screening, patient navigationand treatment support services and cultivate new applicants to the Affiliate’s grant programsthat meet our target communities and priority service areas.Objective 2 – Each grant period, increase by 5% the number of women enrolled and screenedthrough WBCCHP and other partners providing low/no-cost screening, especially amongHispanic and American Indian/Alaska Native women.Objective 3 – By March 2014, work with local partners to develop new and expand currentawareness campaigns (using traditional and social media, Worship in Pink, HispanicInitiative, etc.) that target low-income, Hispanic and American Indian/Alaska Native womenin these counties.Goal: Increase breast cancer awareness, screening and patient navigation in King,Snohomish and Pierce counties for low-income, African American, Hispanic, AmericanIndian/Alaska Native, Vietnamese, Pacific Islander and Asian Indian women.Objective 1 – By March 2014, increase investments in effective education, screening andpatient navigation services and cultivate new applicants to the Affiliate’s grant programs thatmeet our target (current and new) communities and priority services.Objective 2 – By March 2014, expand Worship in Pink campaign to include faith-basedorganizations beyond the African American community.Objective 3 – By March 2014, increase the number of African American, Hispanic,American Indian/Alaska Native, Vietnamese, Pacific Islander and Asian Indian women whoare enrolled in WBCCHP by 5% each grant period.8
Objective 4 – By March 2014, work with local partners to develop new and expand currentawareness campaigns (using traditional and social media, Worship in Pink, HispanicInitiative, etc.) that target low-income, African American, Hispanic, American Indian/AlaskaNative, Vietnamese, Pacific Islander and Asian Indian women in these counties.Goal: Improve access to breast health and treatment services throughout our Service areathrough strategic alliances and change in public policy.Objective 1 – By March 2014, work with National Komen, regional and local partners toadvocate for increased federal and state funding for WBCCHP.Objective 2 – By March 2014, work with Affiliate lobbyist to advocate for and prevent cutsto existing transportation programs and collaborate with American Cancer Society to expandits volunteer transportation program.Objective 3 – By March 2014, work with Affiliate lobbyist and other partners to preserveand/or increase funding for medical interpretation services.Objective 4 – By March 2014, develop strong alliances with existing and new partners thatcan help to move the Komen mission forward through Health Reform implementation.9
IntroductionPurpose of Community Profile ReportThe purpose of this updated report is to assess the extent and prevalence of breast cancer in theService Area. The writers of this report examined statistics, services and community perspectivesto identify disparities, gaps in service and barriers to care that prevent women from detectingbreast cancer early. This report will be used to set Affiliate priorities, goals and objectives in itsstrategic planning, grant making and educational efforts to ensure that we are meeting ourpromise to save and improve lives.Affiliate HistoryNancy G. Brinker promised her dying sister, Susan G. Komen, she would do everything in herpower to end breast cancer forever. In 1982, that promise became Susan G. Komen for the Cure,which is the world’s largest breast cancer organization and the largest source of nonprofit fundsdedicated to the fight against breast cancer with more than 1.3 billion invested to date.The Komen Puget Sound Affiliate in Washington (the Affiliate) was founded in 1993 to forwardthe mission of the National organization – to save lives and end breast cancer forever byempowering people, ensuring quality of care for all and energizing science to find the cures.Since inception, the Affiliate has invested nearly 23 million in local nonprofit, tribal andgovernment agencies that provide breast health/breast cancer services to medically underservedresidents of our sixteen county service area.Affiliate Organizational StructureThe Affiliate is led by a 15-member board of directors and 13 employees. The Affiliate alsorelies on hundreds of volunteers to fulfill its scope of work.10
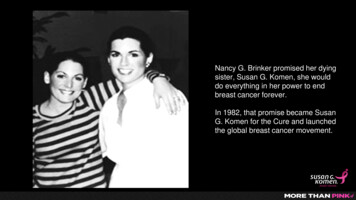
Description of Service AreaThe Affiliate serves 16 counties in Western Washington that includes Whatcom, Skagit, SanJuan, Island, Snohomish, King, Kitsap, Clallam, Jefferson, Mason, Pierce, Thurston, Lewis,Grays Harbor, Pacific and Wahkiakum Counties (the Service Area). The Service Area containsmajor metropolitan cities, rural towns, remote coastal communities and islands that can only beaccessed by boat or plane. See map below.For the purposes of this report, the Service Area is divided into four regions:Greater Metropolitan AreaKing County is the most populated county in Washington. Its largest city is Seattle, with apopulation of more than 600,000. Other primary population centers located on the I-5 or I405 corridor include Bellevue, Redmond, Kirkland, Renton, Kent and Federal Way. Theeastern most part of the county is more rural and less densely populated.Kitsap County is located on the Kitsap Peninsula in the center of the Puget Sound Basin.The population is concentrated within seven major communities – Bremerton, Port Orchard,Poulsbo, Hansville, Silverdale, Kingston and Bainbridge Island. Bremerton is the largest citywith a population of 37,700 but due to the presence of the military, the population tends to betransient. In fact, nearly 70 percent of the county is unincorporated. The northern part of thecounty includes two tribal areas – Suqaumish and S’Klallam.11
Pierce County is located in the southern Puget Sound area and contains a large metropolitanarea (Tacoma), rural farmland, national park and forest area (Mt. Rainier) and two militarybases. The majority of people are concentrated in Tacoma and along the I-5 corridor. Thelargest employer in Pierce County is the Joint Base Lewis McChord. There are a number oftribal areas in Pierce County, including the Puyallup and Nisqually reservations.Snohomish County is located in the north Puget Sound area. The largest city is Everett,which has 24 percent of the entire county’s population. Other major cities in the westernregion include Lynnwood, Bothell, Marysville and Edmonds. The eastern part of the countyis primarily rural and has limited public transportation.Olympic PeninsulaClallam County is west of Seattle and bordered by the Pacific Ocean, the Strait of Juan deFuca and Jefferson County. Major population centers with health services, east to west alongState Route 101, are Sequim, Port Angeles and Forks. Most of the southern part of ClallamCounty is part of national or state forestland and therefore is not inhabited.Jefferson County is located on the Olympic Peninsula, west of Seattle. The largest town isPort Townsend, which is located in the extreme northeast corner. Other towns includeBrinnon and Quilcene in the southeast part of the county. The entire middle of the county iscomposed of Olympic National Park. A small, remote strip of Jefferson County lies along thePacific Ocean and includes Kalalock, Queets and Clearwater.Northwestern CountiesIsland County is comprised of Whidbey Island and Camano Island. While Whidbey Islandis a true island, Camano is physically connected to Snohomish County. This physicalconnection has resulted in a stronger linkage between Camano and Snohomish and Skagitcounties for purposes of seeking services. The majority of Whidbey Island is rural. There arethree population centers - Oak Harbor in the north, Coupeville on central Whidbey Island andClinton in the south. Oak Harbor is home to the Whidbey Island Naval Air Station.San Juan County is located in the northwest corner of the state and comprised of multiplesmall islands. Population and services are principally located on one of three larger islands,San Juan, Lopez and Orcas.Skagit County is located in northwestern Washington and bordered by Whatcom County tothe north, Snohomish County to the south, the Puget Sound to the west and Chelan andOkanogan Counties to the east. Mount Vernon and Anacortes are the largest cities.Whatcom County is located on the northern boundary of Washington State with BritishColumbia, Canada to the north. The county is surrounded by Puget Sound to the west, SkagitCounty to the south and Okanogan County to the east. Most of the population in WhatcomCounty is concentrated along the I-5 corridor. The major population center is Bellingham,which accounts for 59 percent of the county population. Bellingham is also the location of12
Western Washington University. The eastern and northern portions of Whatcom County arerural.Southwestern CountiesGrays Harbor County is situated on the coast, bordering Mason and Thurston counties. Thecounty is largely rural. The largest incorporated cities are Aberdeen and Hoquiam. Othersmaller towns lie along the main road to Olympia and along the coast.Lewis County is situated at the southern end of the Puget Sound region, just below ThurstonCounty. It has the sixth largest land area of all counties in the state, and is predominantlyrural. Centralia is the largest city in the county.Mason County lies on the southern end of the Olympic Peninsula, south of the Hood Canal.A large portion of Mason County is part of Olympic National Forest and uninhabited.Shelton is the largest town in the county and accounts for almost 65 percent of the county’spopulation. The county is home to the Skokomish and Squaxin Island Indian Reservations.Pacific County is on the west coast of Washington. It is primarily rural and composed ofsmall towns, most of which hug the coastline. Most of the population lives in unincorporatedareas. The largest town is Raymond.Thurston County is the fifth most populous county in the Affiliate’s Service Area and lies atthe southern tip of Puget Sound. The population of residents is concentrated in Olympia andLacey, which account for nearly 82 percent of the county’s population.Wahkiakum County is located in the southwest corner of Washington, along the ColumbiaRiver. It is the least populated county in the Affiliate’s Service Area with less than 4,000people. Due to its rural nature, services are limited and the nearest access requires extensivetravel.13
Breast Cancer Impact in Affiliate Service AreaMethodologyThe majority of data used in the demographic section of the Community Profile was obtainedthrough the Thomson Reuters 2009 package: a Komen National commissioned custom moduleof estimated demographic data for the Service Area.The Affiliate relied on local and national sources for our region’s breast cancer sta
Ms. Komen's younger sister, Nancy Goodman Brinker, founded the foundation in 1982. The Komen Puget Sound Affiliate was founded in 1993 to forward the mission of our . Financial barriers and lack of health care insurance are the most commonly reported reasons why