Transcription
The association of indoor tanning and melanoma inadults: Systematic review and meta-analysisSophia Colantonio, MPH,a Michael B. Bracken, PhD, MPH,c and Jennifer Beecker, MDbOttawa, Ontario, Canada, and New Haven, ConnecticutBackground: Tanning beds are associated with increased risk of melanoma.Objective: We sought to update the evidence of the association of melanoma and indoor tanning focusingon frequency of use and exposure to newer tanning beds.Methods: We searched Scopus, MEDLINE, and Cumulative Index to Nursing and Allied Health Literatureon August 14, 2013. We included all observational studies that included patients with melanoma who hadindoor tanned. Odds ratios (OR) with 95% confidence intervals (CI) were extracted and combined usinggeneric inverse variance methods assuming a random effects model.Results: In all, 31 studies were included with data available on 14,956 melanoma cases and 233,106controls. Compared with never using, the OR for melanoma associated with ever using indoor tanning bedswas 1.16 (95% CI 1.05-1.28). Similar findings were identified in recent studies with enrollment occurring inthe year 2000 onward (OR 1.22, 95% CI 1.03-1.45) and in subjects attending more than 10 tanning sessions(OR 1.34, 95% CI 1.05-1.71).Limitations: The quality of evidence contributing to review results ranges from poor to mediocre.Conclusion: Using tanning beds is associated with a subsequent melanoma diagnosis. Exposure frommore than 10 tanning sessions is most strongly associated and there was no statistically significantdifference in this association before and after 2000, suggesting that newer tanning technology is not saferthan older models. ( J Am Acad Dermatol 2014;70:847-57.)Key words: indoor tanning; melanoma; meta-analysis; risk factor; skin cancer; solaria; systematic review;tanning beds.Melanoma is a major public health concernworldwide. During the past 5 decades,incidence rates have increased in fairskinned populations in North America,1 Europe,2and Oceania.3-5 Recent evidence suggests that theincidence of melanoma may have stabilized in NorthAmerica, Australia, New Zealand, and Norway; however, incidence rates are increasing in southern andeastern Europe.6Radiation from sunbeds is a ‘‘known humancarcinogen’’7 increasing an individual’s likelihoodFrom the Faculty of Medicinea and Division of Dermatology,Department of Medicine,b University of Ottawa; and Center forPerinatal, Pediatric, and Environmental Epidemiology, YaleSchool of Public Health, New Haven.cFunding sources: None.Conflicts of interest: None declared.Supplemental tables and figures are available at http://www.jaad.org.Accepted for publication November 26, 2013.Abbreviations used:CI:IARC:OR:UV:confidence intervalInternational Agency for Research onCancerodds ratioultravioletof developing melanoma.8,9 A recent meta-analysisexamined the burden of melanoma associated withuse of indoor tanning globally.9 To our knowledge,Reprint requests: Michael B. Bracken, PhD, MPH, Center forPerinatal, Pediatric, and Environmental Epidemiology, YaleSchool of Public Health, One Church St, Sixth Floor, NewHaven, CT 06510. E-mail: michael.bracken@yale.edu.Published online March 14, 2014.0190-9622/ 36.00Ó 2014 by the American Academy of Dermatology, 7
848 Colantonio, Bracken, and BeeckerJ AM ACAD DERMATOLMAY 2014no meta-analysis to date has separately examined theStudies in Epidemiology (MOOSE) checklists wereassociation in geographic subgroups (Northfollowed to report the meta-analysis findings.15,16America, Europe, Oceania) and in persons youngerthan 25 years. In addition, a dose-dependent relaLiterature searchtionship between sunbed use and the association ofA search for all relevant observational studies inmelanoma is vaguely defined in the literature asScopus (from 1996), MEDLINE (from 1946), and‘‘high use’’ versus never.9 It is important to quantifyCumulative Index to Nursing and Allied Healththis association in metricsLiterature (from 1937) wasthat are more easily underperformed up to August 14,CAPSULE SUMMARYstood and personally rele2013. One author performedvant to patients.the search with assistanceIndoor tanning increases melanoma risk.Recent estimates reportfrom a medical librarianThis meta-analysis observes increasedthat 30 million Northwith expertise in searchingrisk particularly after 10 tanning sessions,Americans expose themresearch bibliographies. Noand this risk persists despite lower-riskselves to indoor tanning andlimits to date or languagetechnical changes to ultraviolet bulbs.of those 2.3 million are adowere applied. Translationslescents.10 The highest use iswere obtained for articlesRisk estimates based on number ofamong Caucasian Americanthat were published in lansessions facilitates patient riskwomen aged 18 to 21 yearsguages other than English orassessment and patient education.and 22 to 25 years with aFrench. A manual search wasprevalence of 31.8% andconducted on references29.6% use in the past year, respectively.11 Thecited in selected articles and meta-analyses/prevalence of ever using sunbeds in Germany issystematic reviews on this topic.9,17-20 Efforts were1239.2% and within the past year was 14.6%. Tanningmade to contact the authors of 6 studies.21-26 Authorsbed use within the past year in Denmark wasfrom 3 studies23-25 responded and none were able toestimated to be 29% and with females aged 15 tolocate their original data sets as they were 20 to 4019 years comprising the highest users, 59%.13 Sunbedyears old. Subsequently, these 6 studies wereuse in Australia is lower than in North America andincluded in the systematic review but were excludedEurope with 10.6% of adults and 2.5% of teensfrom the meta-analysis because they did not includereporting ever using tanning beds and the mostan estimate of odds of melanoma.frequent users being women age 18 to 24 yearsThe electronic search strategy to identify relevant(17.1%) and 25 to 44 years (20.7%).14articles included searching for articles containing theThe purpose of this systematic review and metakey word ‘‘melanoma’’ in combination with any ofanalysis is to determine the association of melanomathe following key words to identify indoor tanningfrom the use of indoor tanning beds worldwide inexposure: ‘‘sunbed,’’ ‘‘sun bed,’’ ‘‘sunbathing,’’ ‘‘interms of frequency of use, and use of newer tanningdoor tanning,’’ ‘‘tanning bed,’’ ‘‘tanning parlor,’’beds.‘‘tanning salon,’’ ‘‘tanning booth,’’ ‘‘solaria,’’ ‘‘solarium,’’ ‘‘sun lamp,’’ ‘‘artificial UV,’’ ‘‘artificial ultraviolet,’’ and ‘‘artificial light’’ (see Supplemental Table IIMETHODSfor full search strategy). Key words were truncatedStudy selectionappropriately to catch all variations and wordIncluded studies were all cohort, case-control, andendings to assure that studies pertaining to melacross-sectional studies that examined patients givennoma and indoor tanning were identified.the diagnosis of melanoma who were exposed or notto indoor tanning. For retrospective studies, the mainData extraction and statistical analysesmeasurement outcome was development of melaTwo authors checked titles and abstracts found innoma (yes/no). For prospective studies, the mainthis search and determined the eligibility of themeasurement outcome was time to melanoma diagarticle using the defined inclusion criterianosis. Excluded studies were reviews, ecological(Supplemental Table I). Information was extractedstudies, case reports, editorials, commentaries, letters,from the articles meeting the inclusion criteria by 2news, perspectives, conference proceedings, in vitro/authors and 1 entered it into Review Managerin vivo studies, and studies with irrelevant content.software (RevMan5)27 for analysis. Data were exTheses and unpublished studies were excluded(Supplemental Table I). The Preferred Reportingtracted following RevMan527 criteria developed byItems for Systematic Reviews and Meta-AnalysesCochrane Review. Two authors assessed the risk of(PRISMA) and Meta-analysis of Observationalselection bias, recall bias, and interview bias. Studiesddd
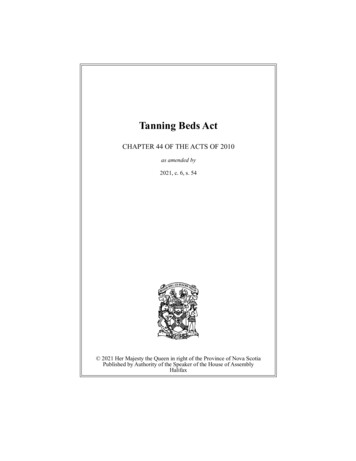
J AM ACAD DERMATOLVOLUME 70, NUMBER 5Colantonio, Bracken, and Beecker 849Fig 1. Flow chart of studies of exposure to indoor tanning use with risk of melanoma.
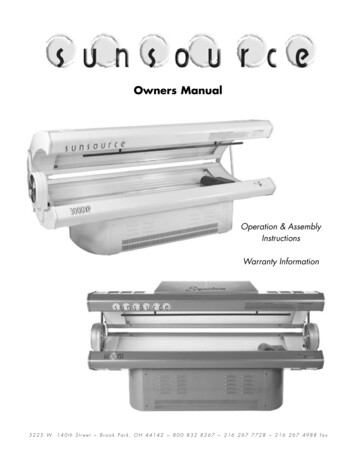
850 Colantonio, Bracken, and BeeckerJ AM ACAD DERMATOLMAY 2014Fig 2. Melanoma risk based on ever versus never used indoor tanning by region. Estimate forMacKie et al38 in 1989 was determined from a meta-analysis of men and women subgroups;Nielsen et al57 in 2012 was from a meta-analysis of sunbed use 1-10 and [10 times/y. Variationsin the estimate from the original article may vary by 100th of a decimal place because ofrounding in RevMan.27 CI, Confidence interval; df, degrees of freedom; IV, inverse variance.were excluded if they included populations withhigh inherent risk of melanoma, such as patients withprofound immunosuppression and genetic predispositions to skin cancer.If duplicate data were present in multiple sources, the source with the longest follow-up wasincluded. RevMan527 was used for statisticalanalyses. Studies that met the inclusion criteriawere critically evaluated and data were extracted.This information was compiled into summarytables. Odds ratios (OR) with 95% confidenceintervals (CI) were used for the prospective andcase-control studies, respectively, to examine therisk difference between those who had used tanning beds versus those who had never used tanningbeds. Adjusted ORs were used when available,otherwise crude ORs were used. A generic inversevariance method assuming a random effects modelwas used for the meta-analysis. Heterogeneity wastested by the x 2 test and using the I2 statistic with avalue of: less than 25% none; 25% to 49% low;50% to 74% moderate; and 75% or more high.28
J AM ACAD DERMATOLVOLUME 70, NUMBER 5Colantonio, Bracken, and Beecker 851Fig 3. Melanoma risk based on ever versus never used indoor tanning in studies withenrollment year \2000 versus 2000. Estimate for MacKie et al38 in 1989 was determined froma meta-analysis of men and women subgroups; Nielsen et al57 in 2012 was from a meta-analysisof sunbed use 1-10 and [10 times/y. Variations in the estimate from the original article mayvary by 100th of a decimal place because of rounding in RevMan.27 CI, Confidence interval;df, degrees of freedom; IV, inverse variance.Prespecified subgroup analyses were carried outaccording to:1. Continent (North America, Europe, Oceania).2. Recent studies (study enrollment completed\2000 vs 2000).3. Dosage (number of lifetime indoor tanningsessions: 1-10 vs [10).4. Age of first use of sunbeds (\25 vs 25 years).5. Duration of use ( # 1 vs [1 year).RESULTSThe electronic database search yielded 361records and the manual search yielded 18additional records on the use of indoor tanningbeds and melanoma (Fig 1). After duplicate recordswere removed, 281 records were screened. Afterscreening, 85 full-text articles were assessed foreligibility. A total of 37 studies met the inclusioncriteria for the systematic review (n 251,808participants) and 31 articles provided specific riskestimates and were included in the meta-analyses(n 248,062 participants). Characteristics ofincluded studies in the systematic review andmeta-analysis are described in SupplementalTables IIIa and IIIb. The North American subgroupstudy characteristics are presented in SupplementalTable IIIc.In all, 48 studies were excluded (SupplementalTable IV). Common reasons for exclusion include:
852 Colantonio, Bracken, and BeeckerJ AM ACAD DERMATOLMAY 2014Fig 4. Melanoma risk based on duration of use # 1 and [1 year versus never use. For use # 1year: Swerdlow et al60 in 1988 estimate was determined from a meta-analysis of duration of usesubgroups: \3 months and 3 months to 1 year. For use [1 year: Lazovich et al46 in 2010estimate was determined from a meta-analysis of subgroups 2-5, 6-9, and [10 years. Variationsin the estimate from the original article may vary by 100th of a decimal place because ofrounding in RevMan.27 CI, Confidence interval; df, degrees of freedom; IV, inverse variance.Fig 5. Melanoma risk based on frequency of use 1-10 times versus never use. For Chen et al42in 1998 and Clough-Gorr et al43 in 2008 the estimate was for \10 times. For Fears et al44 in 2011the estimate was for 1-9 times. For Naldi et al56 in 2000 the estimate was for # 15 times. ForWesterdahl et al62 in 1994 the estimate was determined from a meta-analysis of subgroups of1-3 and 4-10 uses per year. For Westerdahl et al63 in 2000 the estimate was determined from ameta-analysis for 1-5 and 6-10 uses per year. Variations in the estimate from the original articlemay vary by 100th of a decimal place because of rounding in RevMan.27 CI, Confidenceinterval; df, degrees of freedom; IV, inverse variance.multiple reports of the same study; outcome was notcutaneous melanoma (eg, ocular/uveal melanoma,benign papillomatous melanocytic nevi, or basal cellcarcinoma); participants were not followed up untilthe diagnosis of melanoma; and only prevalencedata were reported without an estimate of theassociation of indoor tanning use and melanoma(Supplemental Table I).Compared with the avoidance of tanning beds(never used), the overall (North America, Europe,and Oceania) OR for melanoma associated withever using indoor tanning beds was 1.16 (95% CI1.05-1.28, number of studies [n] 31) (Fig 2). InNorth America, the OR was 1.23 (95% CI 1.03-1.47,n 8) with high heterogeneity (Fig 2). Similarfindings were identified in recent studies withenrollment occurring in the year 2000 onward(OR 1.22, 95% CI 1.03-1.45, n 10) (Fig 3).Duration of exposure to tanning beds suggesteda dose-dependent relationship: exposure less thanor equal to 1 year was associated with a 37%increased risk (OR 1.37, 95% CI 1.06-1.77, n 3)and rose to 61% with exposure for more than 1year (OR 1.61, 95% CI 0.98-2.67, n 3) (Fig 4). Thedata also suggest a threshold effect exists withincreasing frequency of exposure to indoor tanning. A significant result was found with lifetimeexposure to greater than 10 tanning sessions (OR1.34, 95% CI 1.05-1.71, n 10), and a nonsignificant result was found with lifetime exposure of
J AM ACAD DERMATOLVOLUME 70, NUMBER 5Colantonio, Bracken, and Beecker 853Fig 6. Melanoma risk based on frequency of use [10 times versus never use. For Chen et al42in 1998 and Clough-Gorr et al43 in 2008 the estimate was for 10 times. For Fears et al44 in 2011the estimate calculated by adding 10-50 times and 50 times then calculating the crude oddsratio. For Lazovich et al46 in 2010 the estimate was determined from a meta-analysis for 11-24,25-100, and [100 sessions. For Naldi et al56 in 2000 the estimate was for [15 times. ForWesterdahl et al62 in 1994 the estimate was for [10 times per year. For Westerdahl et al63 in 2000the estimate was determined from a meta-analysis for 11-15 and 20 uses per year. Variationsin the estimate from the original article may vary by 100th of decimal place because of roundingin RevMan.27 CI, Confidence interval; df, degrees of freedom; IV, inverse variance.Fig 7. Melanoma risk based on age of first use \25 versus 25 years by ever versus never use.Age at first use\25 years: for Clough-Gorr et al43 in 2008 an estimate of age\20 years was used;for Fears et al44 in 2011 an estimate of use before age 20 years was used; and for Lazovich et al46in 2010 an estimate was derived from a meta-analysis for age \18 and 18-24 years. Age at firstuse 25 years: for Chen et al42 in 1998 an estimate was derived from a meta-analysis for age25-45 and [45 years; for Clough-Gorr et al43 in 2008 an estimate of age 20 years was used; forCust et al67 in 2011 an estimate was derived from a meta-analysis for age 25 years (1-10 vs 10 sessions); for Fears et al44 in 2011 an estimate of age 20 years was used; and for Lazovichet al46 in 2010 an estimate was derived from a meta-analysis for age 25-34 and 35 years.Variations in the estimate from the original article may vary by 100th of decimal place because ofrounding in RevMan.27 CI, Confidence interval; df, degrees of freedom; IV, inverse variance.1 to 10 tanning sessions (OR 1.07, 95% CI0.90-1.26, n 10) (Figs 5 and 6). Indoor tanningfirst use younger than 25 years (OR 1.35, 95% CI0.99-1.84, n 6) carried a higher risk than first useat age 25 years or older (OR 1.11, 95% CI 0.86-1.42,n 6) (Fig 7). There was no meaningful differencebetween the primary analysis and the sensitivityanalysis for all sub-group comparisons: region,enrollment year, duration of use, frequency of use,and age of first use (Supplemental Table V).
854 Colantonio, Bracken, and BeeckerRisk of bias in included studiesIncluded studies were assessed for several types ofbias including: selection bias, recall bias, interviewbias, and questionnaire bias (Supplemental Table VI).Selection bias occurred in the form of controlselection and self-selection. Control selection biasmay have occurred in the studies that used hospitalbased controls. Observational studies are prone toself-selection bias. Nonparticipant cases and controlsmay have differed significantly from participantswith respect to sunbed use. Highly exposedindividuals may refuse to participate to avoid thepotential scrutiny by medical professionals, thusunderestimating the association. Most studies didnot collect information on nonparticipants.Observational studies carry an inherent risk ofrecall bias; controls may underreport their use and,less likely, cases may overreport sunbed exposuresto explain their melanoma. The direction of this biasis likely to vary with each study’s specific population.Many of the observational studies collected information through interviews where interview bias couldhave been introduced. Most studies reduced interviewbias using one or a combination of: structuredquestionnaires, trained interviewers, and distractingquestions. Blinding case and control status was notalways possible because some cases had visible scarsafter melanoma excision or because respondents’answers to interview questions revealed their case orcontrol status. This would likely inflate the associationas cases would be encouraged more than controls toreport exposure to tanning beds; however, this biasmay only contribute minimally to the overall findings.Publication bias was assessed using a funnel plot of theSE(log)OR against the odds estimate for each study.DISCUSSIONThe results of this meta-analysis support thegrowing body of evidence that use of indoor tanningincreases the odds of melanoma. Overall in this studythe increased risk was 16%. North Americans who hadever exposed themselves to indoor tanning had a 23%increased risk of developing melanoma. This association was nonsignificant in Europe and Oceania,possibly because tanning beds in Europe and inAustralia and New Zealand are limited in intensity toultraviolet (UV) index of 12 and 36, respectively.29 TheOceania limits were tightened in 2008 to the new UVindex limit of 36, which was previously a maximum UVindex of 60 under 2002 regulations.29 In the UnitedStates, the intensity of tanning beds is unrestricted butoften has short ‘‘maximum recommended exposuretimes.’’30 The limitations of intensity in Europe andOceania versus no limits in the United States mayaccount for the observed differences. In addition, weJ AM ACAD DERMATOLMAY 2014observed a threshold effect for more than 10 tanningsessions conferring higher odds of melanoma. Also, theevidence showed that using indoor tanning before theage of 25 years further increased an individual’s odds ofmelanoma from 11% to 35% as compared with thosewho started indoor tanning after the age of 25 years. Alimitation of this finding was 4 of the 8 studies used age20 years as a cutoff instead of age 25 years. Thesestudies were included to increase the sample size;however, it is likely to have attenuated the effectobserved. Lastly, it was demonstrated that there wasno statistically significant difference in the associationof melanoma and indoor tanning before and after 2000,suggesting that newer technology tanning bulbsappear to be no safer than older models. This questioncould ideally be examined in future studies by identifying subjects who started use of tanning beds in thesetime periods, as the exposure to the beds may haveoccurred well before study enrollment. Our findingsare consistent with a recent meta-analysis examiningglobal trends that found early exposure and morefrequent use of indoor tanning significantly increasedrisks of melanoma.9 Earlier meta-analyses includestudies from all populations: North America, Europe,and Oceania and provide an aggregate measure of theassociation9,17; however, we provide specific estimatesby region that have not been reported. We defined firstsunbed exposure to be younger than 25 years tocapture the particular experiences of teenagers andyoung adults who may be more susceptible to peerpressure, advertising, and less aware of lifetime cumulative risks.31,32 The risk profile for adults age 25 to 35years is different as they are generally considered lesslikely to indulge in risky behaviors.33-36 Our studyquantified ‘‘high use’’ as greater than 10 indoor tanningsessions. Assessing and communicating health risk topatients in an easily understood metric based onnumber of tanning bed sessions could be helpful toclinical practice. Our analysis is novel in the delineationof use of newer tanning beds, captured in the subgroupof studies from the year 2000 onward. More than adecade ago, the tanning industry switched to higherpressure lamps emitting larger doses of long-wave UVA([335-400 nm) and this association has not been fullyevaluated.37This systematic review contains 37 studies and251,808 participants (16,667 cases and 235,141controls). Only moderate heterogeneity among 31studies in the meta-analysis was observed (I2 52%).However, the quality of the body of evidencecontributing to results of the review ranges frompoor to mediocre and several of the subgroupanalyses contained high heterogeneity (I2 75).This low-medium quality is likely a result of the casecontrol study design that was used in almost half of
J AM ACAD DERMATOLVOLUME 70, NUMBER 5the studies especially those with enrollment occurring before the year 2000. A case-control design canestimate the magnitude of association of tanning beduse and melanoma because the disease has a longinduction period; however, it is vulnerable to biasparticularly selection, recall, and interview bias. Inparticular, observational studies can producemisleading results regarding the association oftanning bed use and melanoma as the exposure totanning beds could not be allocated randomly or useblinding. Bias was potentially present in all includedstudies and several studies possibly had largeamounts of bias. The case-control design is alsolimited in establishing a temporal relationshipbetween tanning bed exposure and developmentof melanoma. More recent studies with enrollmentoccurring since the year 2000 have begun to useprospective cohorts and nested case-control designsthat reduce the likelihood of bias and shouldimprove the overall quality of evidence. No evidenceof publication bias was observed from a funnel plotanalysis in the overall estimate of association or bygeographic region (Supplemental Fig 8).There have been 5 prior systematic reviews of apossible association between indoor tanning andmalignant melanoma.9,17-20 Comparison of dataextracted by them demonstrates an alarming tendencyfor data extracted for one review to be copiedby subsequent reviewers without reference to theoriginal article, precluding checking for errors. Forexample, the International Agency for Research onCancer (IARC) Working Group20 published aninfluential review in 2007 that appeared to havetypographical errors in the number of controlsreported for MacKie et al38 in 1989 (180 instead of280) and Adam et al39 in 1981 (207 instead of 507).These errors were replicated in 2 subsequentreviews.9,18 Other perhaps more debatable differencesin data extraction refer to whether intent-to-treatprinciples should be applied to case-control studies.For example, in considering Adam et al39 in 1981, theIARC20 reviewers included cases and controls withincomplete or no questionnaire data (some subjectshad died) whereas the current review and Swerdlowand Weinstock19 in 1998 analyzed only subjects withcompleted questionnaires. Other data from IARC20 in2007 extracted from Garbe et al40 in 1993 (280 casesand 280 controls), and copied by Boniol et al9 in 2012could not be replicated by us (856 cases and 705controls), which agrees with the reviews by Swerdlowand Weinstock19 in 1998, Gallagher et al17 in 2005, andHirst et al18 in 2009. Further, data we have extractedfrom Ting et al41 in 2007 (79 cases and 1439 controls)disagree with Boniol et al9 in 2012 (29 cases and 307controls), which we could not derive.Colantonio, Bracken, and Beecker 855This meta-analysis has highlighted the poor tomediocre quality of evidence available on this topic,mainly because of the majority of studies using acase-control design that is prone to several biases.Randomized clinical trials are the gold standard ofevidence but they are unethical for studying thecarcinogenic potential of tanning beds. Thus, futureresearch should consider prospective study designsin large population cohorts. Clinicians shouldcontinue to educate patients on the harms of indoortanning and encourage its cessation.We are grateful to Livia Kidd for her technical assistancein the preparation of this manuscript and to Janis Glover forconsulting on the bibliography search methodology.REFERENCES1. Linos E, Swetter SM, Cockburn MG, Colditz GA, Clarke CA.Increasing burden of melanoma in the United States. J InvestDermatol 2009;129:1666-74.2. de Vries E, Coebergh JW. Cutaneous malignant melanoma inEurope. Eur J Cancer 2004;40:2355-66.3. Baade P, Meng X, Youlden D, Aitken J, Youl P. Time trendsand latitudinal differences in melanoma thickness distribution in Australia, 1990-2006. Int J Cancer 2012;130:170-8.4. Bulliard JL, Cox B. Cutaneous malignant melanoma in NewZealand: trends by anatomical site, 1969-1993. Int J Epidemiol 2000;29:416-23.5. Sneyd MJ, Cox B. Melanoma in Maori, Asian, and Pacificpeoples in New Zealand. Cancer Epidemiol Biomarkers Prev2009;18:1706-13.6. Erdmann F, Lortet-Tieulent J, Schuz J, Zeeb H, Greinert R,Breitbart EW, et al. International trends in the incidence ofmalignant melanoma 1953-2008eare recent generations athigher or lower risk? Int J Cancer 2013;132:385-400.7. US Department of Health and Human Services, PublicHealth Service National Toxicology Program. 12thReport on Carcinogens (RoC). Research Triangle Park (NC);2011. pp. 430-3. Available from: URL: http://ntp.niehs.nih.gov/?objectid 03C9AF75-E1BF-FF40-DBA9EC0928DF8B15. Accessed August 8, 2012.8. The Indoor Tanning Working Group. Report of the IndoorTanning Working Group (ITWG). Victoria, British Columbia(Canada): British Columbia Ministry of Health; 2011.9. Boniol M, Autier P, Boyle P, Gandini S. Cutaneous melanomaattributable to sunbed use: systematic review andmeta-analysis. BMJ 2012;345:e4757.10. Fisher DE, James WD. Indoor tanningescience, behavior, andpolicy. N Engl J Med 2010;363:901-3.11. Centers for Disease Control and Prevention (CDC). Use ofindoor tanning devices by adultseUnited States, 2010.MMWR Morb Mortal Wkly Rep 2012;61:323-6.12. Schneider S, Diehl K, Bock C, Schluter M, Breitbart EW,Volkmer B, et al. Sunbed use, user characteristics, andmotivations for tanning: results from the Germanpopulation-based SUN study 2012. JAMA Dermatol 2013;149:43-9.13. Koster B, Thorgaard C, Clemmensen IH, Philip A. Sunbed usein the Danish population in 2007: a cross-sectional study.Prev Med 2009;48:288-90.14. Francis K, Dobbinson S, Wakefield M, Girgis A. Solarium use inAustralia, recent trends and context. Aust N Z J Public Health2010;34:427-30.
856 Colantonio, Bracken, and Beecker15. Moher D, Liberati A, Tetzlaff J, Altman DG, PRISMA Group.Preferred reporting items for systematic reviews andmeta-analyses: the PRISMA statement. PLoS Med 2009;6:e1000097.16. Stroup DF, Berlin JA, Morton SC, Olkin I, Williamson GD, RennieD, et al. Meta-analysis of observational studies in epidemiology:a proposal for reporting; meta-analysis of observational studiesin epidemiology (MOOSE) group. JAMA 2000;283:2008-12.17. Gallagher RP, Spinelli JJ, Lee TK. Tanning beds, sunlamps, andrisk of cutaneous malignant melanoma. Cancer EpidemiolBiomarkers Prev 2005;14:562-6.18. Hirst N, Gordon L, Gies P, Green AC. Estimation of avoidableskin cancers and cost-savings to government associated withregulation of the solarium industry in Australia. Health Policy2009;89:303-11.19. Swerdlow AJ, Weinstock MA. Do tanning lamps causemelanoma? An epidemiologic assessment. J Am AcadDermatol 1998;38:89-98.20. International Agency for Research on Cancer Working Groupon Artificial Ultraviolet (UV) Light and Skin Cancer. Theassociation of use of sunbeds with cutaneous malignantmelanoma and other skin cancers: a systematic review.Int J Cancer 2007;120:1116-22.21. Beitner H, Norell SE, Ringborg U, Wennersten G, Mattson B.Malignant melanoma: etiological importance of individualpigmentation and sun exposure. Br J Dermatol 1990;122:43-51.22. Dubin N, Moseson M, Pasternack BS. Sun exposure andmalignant melanoma among susceptible individuals. EnvironHealth Perspect 1989;81:139-51.23. Gallagher RP, Elwood JM, Hill GB. Risk factors for cutaneousmalignant melanoma: the western Canada melanoma study.Recent Results Cancer Res 1986;102:38-55.24. Holly EA, Kelly JW, Shpall SN, Chiu SH. Number of melanocytic nevi as a major risk factor for malignant melanoma.J Am Acad Dermatol 1987;17:459-68.25. Klepp O, Magnus K. Some environmental and bodilycharacteristics of melanoma patients: a case-control study.Int J Cancer 1979;23:482-6.26. Rodenas JM, D
reporting ever using tanning beds and the most frequent users being women age 18 to 24 years (17.1%) and 25 to 44 years (20.7%).14 The purpose of this systematic review and meta-analysis is to determine the association of melanoma from the use of indoor tanning beds worldwide in terms of frequency of use, and use of newer tanning beds. METHODS