Transcription
ORIGINAL ARTICLEWho Should Get Extended ThromboprophylaxisAfter Bariatric Surgery?A Risk Assessment Tool to Guide Indications for Post-dischargePharmacoprophylaxisAli Aminian, MD, Amin Andalib, MD, Zhamak Khorgami, MD, Derrick Cetin, DO, Bartolome Burguera, MD, John Bartholomew, MD,y Stacy A. Brethauer, MD, and Philip R. Schauer, MD Objective: To determine the risk factors for 30-day postdischarge venousthromboembolism (VTE) after bariatric surgery and to identify potentialindications for extended pharmacoprophylaxis.Background: VTE is among most common causes of death after bariatricsurgery. Most VTEs occur after hospital stay; still a few patients receiveextended pharmacoprophylaxis postdischarge.Methods: From American College of Surgeons-National Surgical QualityImprovement Program, we identified 91,963 patients, who underwent electiveprimary and revisional bariatric surgery between 2007 and 2012. Regressionbased techniques were used to create a risk assessment tool to predict risk ofpostdischarge VTE. The model was validated using the 2013 AmericanCollege of Surgeons-National Surgical Quality Improvement Program dataset(N ¼ 20,575). Significant risk factors were used to create a user-friendlyonline risk calculator.Results: The overall 30-day incidence of postdischarge VTE was 0.29% (N ¼269). In those experiencing a postdischarge VTE, mortality increased about28-fold (2.60% vs 0.09%; P 0.001). Among 45 examined variables, the finalrisk-assessment model contained 10 categorical variables including congestive heart failure, paraplegia, reoperation, dyspnea at rest, nongastric bandsurgery, age 60 years, male sex, BMI 50 kg/m2, postoperative hospital stay 3 days, and operative time 3 hours. The model demonstrated goodcalibration (Hosmer-Lemeshow goodness-of-fit test, P ¼ 0.71) and discrimination (c-statistic ¼ 0.74). Nearly 2.5% of patients had a predicted postdischarge VTE risk 1%.Conclusions: More than 80% of post-bariatric surgery VTE events occurredpost-discharge. Congestive heart failure, paraplegia, dyspnea at rest, andreoperation are associated with the highest risk of post-discharge VTE.Routine post-discharge pharmacoprophylaxis can be considered for high-riskpatients (ie, VTE risk 0.4%).Keywords: bariatric surgery, complication, deep vein thrombosis, gastricbypass, morbidity, mortality, pharmacoprophylaxis, pulmonary embolism,sleeve gastrectomy, thromboprophylaxis, venous thromboembolismFrom the Bariatric and Metabolic Institute, Cleveland Clinic, Cleveland, OH; andyHeart and Vascular Institute, Cleveland Clinic, Cleveland, OH.Funding: None.Presentation: This study was presented at the 32nd Annual Meeting of the ASMBSat ObesityWeek, Los Angeles, CA; November 2–7, 2015.ACS-NSQIP Disclaimer: The American College of Surgeons-National SurgicalQuality Improvement Program (ACS-NSQIP) and the hospitals participatingin the ACS-NSQIP are the source of the data used herein; they have not verifiedand are not responsible for the statistical validity of the data analysis or theconclusions derived by the authors.The authors declare no conflict of interest.Reprints: Ali Aminian, MD, Bariatric and Metabolic Institute, Cleveland Clinic,9500 Euclid Avenue, M61, Cleveland, OH 44195. E-mail: aminiaa@ccf.org.Copyright ß 2016 Wolters Kluwer Health, Inc. All rights reserved.ISSN: 0003-4932/16/26501-0143DOI: 10.1097/SLA.0000000000001686Annals of Surgery Volume 265, Number 1, January 2017(Ann Surg 2017;265:143–150)The obesity epidemic worldwide and the exponential rise inmorbid obesity have led to a significant increase in bariatricsurgery over the past two decades driven by the advancements insurgical techniques and use of laparoscopy.1–3 Despite a substantialdecrease in the postoperative adverse events because of key improvements in multidisciplinary perioperative surgical care of morbidlyobese patients, bariatric surgery is associated with certain postoperative complications.4Venous thromboembolism (VTE) remains a major cause ofmorbidity and mortality after bariatric surgery.5,6 Reported rates ofdeep vein thrombosis (DVT) are 1–3% and 0.3–2% for pulmonaryembolism (PE).7 –10 Given the significant VTE risk in these patients,both the American College of Chest Physicians and the AmericanSociety for Metabolic and Bariatric Surgery have recommended thatin addition to mechanical prophylaxis some form of pharmacoprophylaxis be administered to all bariatric surgery patients in theabsence of contraindications.11,12Greater majority of VTE events after bariatric surgery occurafter the discharge from the hospital but within the 30-day postoperative period.13 Furthermore, certain VTE risk factors such asbody mass index (BMI), age, sex, personal history of VTE, obesityhypoventilation syndrome, immobility, pulmonary hypertension,operative time, and procedure type have been identified.13– 15 However, such risk profiles are not well established and there is littleevidence to guide a risk-adjusted approach to VTE preventionpostbariatric surgery.Despite the customary inhospital use of mechanical andpharmacoprophylaxis, it is unclear who should receive a moreaggressive chemoprevention perhaps with a higher dose or a moreextended prophylaxis period after their hospital discharge. Hence, weaimed to determine the risk factors for 30-day postdischarge VTEafter bariatric surgery and to identify potential indications forextended pharmacoprophylaxis.METHODSThe study is based on analysis of data from the AmericanCollege of Surgeons-National Surgical Quality Improvement Program (ACS-NSQIP) database. The ACS-NSQIP prospectively collects detailed data on over 300 variables, including standardized andaudited demographic variables, preoperative comorbidities, laboratory values, and 30-day postoperative mortality and morbidity outcomes for patients undergoing major surgical procedures inacademic and community hospitals in North America (435 participating sites in 2013 and 374 sites in 2012). The program has utilizedseveral mechanisms to ensure that the data collected are of thehighest consistency and reliability.16www.annalsofsurgery.com 143Copyright 2016 Wolters Kluwer Health, Inc. All rights reserved.
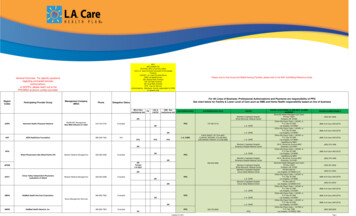
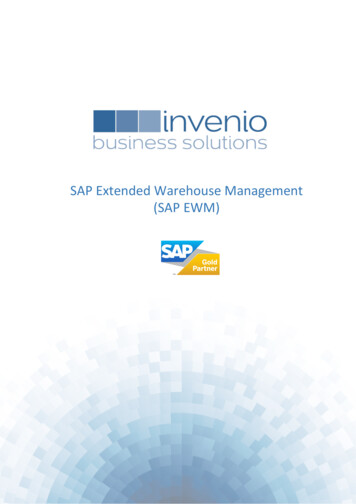
Annals of Surgery Volume 265, Number 1, January 2017Aminian et alWe identified adult obese patients (BMI 30 kg/m2), whounderwent bariatric surgical procedures including adjustable gastricbanding (AGB), sleeve gastrectomy (SG), Roux-en-Y gastric bypass(RYGB), biliopancreatic diversion-duodenal switch (BPD-DS), andrevisional surgery using their respective Current Procedural Terminology codes (AGB: 43770; SG: 43843, 43775; RYGB: 43644,43645; BPD-DS: 43845; and revision 43848, 43860, 43865).Patients who underwent emergency surgery or unrelated concurrentprocedures, such as hysterectomy, had a surgery in the 30 daysbefore the index bariatric surgery, preoperative sepsis, disseminatedcancer, and American Society of Anesthesiology (ASA) class 5(Moribund) were excluded. Based on the inclusion/exclusioncriteria, 91,963 patients from 2007 to 2012 were included. Aswe aimed to evaluate postdischarge VTE occurrence, patientswho developed VTE in the index hospital stay were further excluded(N ¼ 54) making the study cohort for statistical analysis at91,909 patients. In addition, 20,575 patients with the same criteriawere identified in the ACS-NSQIP 2013 database to examinethe validity of risk model.The primary outcome was the occurrence of postdischargeVTE (including DVT or PE) within 30-days of the index bariatricsurgery. The ACS-NSQIP defines DVT as a new thrombus within thevenous system confirmed with imaging studies and requiringtherapy. The PE should be documented with ventilation-perfusionlung scan (V-Q scan), CT scan, pulmonary arteriogram, or any otherdefinitive modality (including direct pathology examination such asautopsy). A postdischarge VTE variable implies events, whichoccurred after hospital discharge after index bariatric surgery.Independent demographic variables were sex, age, race/ethnicity, weight, and BMI. Lifestyle factors included smoking statusand alcohol use. Examined comorbidities included diabetes (andinsulin usage), hypertension, history of pulmonary diseases [pneumonia, dyspnea, and chronic obstructive pulmonary diseases(COPD)], congestive heart failure (CHF), history of coronary arterydisease (CAD) (binary variable representing angina, myocardialinfarction, cardiac interventions, and cardiac surgeries), history ofatherosclerotic peripheral vascular diseases (PVD), history of kidneydiseases (renal failure and being on dialysis), history of cerebrovascular diseases (transient ischemic attack and stroke), paraplegia,and steroid/immunosuppressant use for chronic conditions. Thefunctional status (dependent/independent) and the ASA score werealso collected. Preoperative laboratory variables included serumcreatinine, albumin, hematocrit, and platelet count. The effect oftype of surgery, operative time, return to the operating room, andlength of stay (LOS) were also assessed. All variables were clearlydefined in the ACS-NSQIP database user guide.16Statistical analyses were carried out using the STATA software(Stata Corp, TX) version 12. The estimates on the study variables areexpressed as mean standard deviation (SD) and frequencies (%).Patients were categorized into postdischarge VTE and no VTEsubgroups. Univariate analyses using student’s t test or Wilcoxonrank-sum test for continuous variables, and Pearson x2 test or Fisherexact test for categorical variables were used to assess potential riskfactors for postdischarge VTE.Multiple logistic regression with stepwise variable selectionwas used to construct a model for prediction of the primary outcome.Independent risk factors with a significant association with postdischarge VTE (P 0.1) in univariate analyses were entered into amodel. With backward elimination procedure, only significant riskfactors (P 0.05) were kept in the model. Afterward, a forwardstepwise selection was also utilized which achieved the same model.Once a stable model was developed, all eliminated variables wererechecked and none had a significant effect on the model. Odds ratio(OR) and 95% confidence intervals (CI) were used as measures ofmagnitude of association.The receiver-operating characteristic (ROC) curve showed thesensitivity and specificity of various cut-points for calculated risk topredict postdischarge VTE and the best cut-points were specifiedwith Youden’s J index (sensitivityþspecificity–1). The calibration ofthe model was tested using the Hosmer-Lemeshow goodness-of-fittest. The discriminatory capability of the model was assessed usingthe c-statistic.17–19 The risk model based on the 2007–2012 ACSNSQIP dataset was then validated using the 2013 dataset.The regression equation used to generate the risk assessmentmodel was utilized to construct a free online version of the calculatorusing the Cleveland Clinic Risk Calculator Constructor (http://www.r-calc.com).RESULTSWe identified 91,963 patients who underwent bariatricsurgeries between 2007 and 2012. Thirty-day total and postdischargefrequencies of DVT were 0.22% (N ¼ 207) and 0.19% (N ¼ 178),respectively. Furthermore, 30-day total and postdischarge frequencies of PE were 0.17% (N ¼ 154) and 0.13% (N ¼ 124), respectively.Overall, 83% (269/323) of postbariatric surgery VTE events occurredafter hospital discharge (Figure 1).Baseline characteristics of patients who underwent primaryand revisional bariatric surgery between 2007 and 2012 have beensummarized in Table 1. Patients had a mean age of 45.01 11.62years and BMI of 45.91 7.90 kg/m2. Seventy nine percent of cohortwere female, and 74% were white. After excluding the 54 patients,FIGURE 1. Postoperative occurrence ofdeep vein thrombosis and pulmonaryembolism in 30 days after bariatricsurgery.144 www.annalsofsurgery.comß2016 Wolters Kluwer Health, Inc. All rights reserved.Copyright 2016 Wolters Kluwer Health, Inc. All rights reserved.
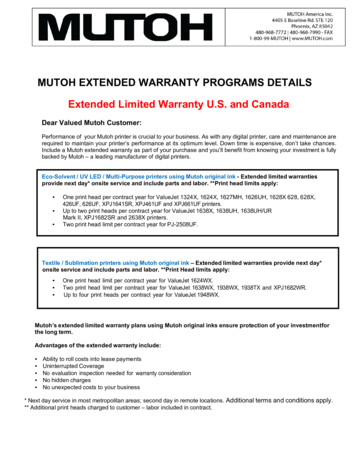
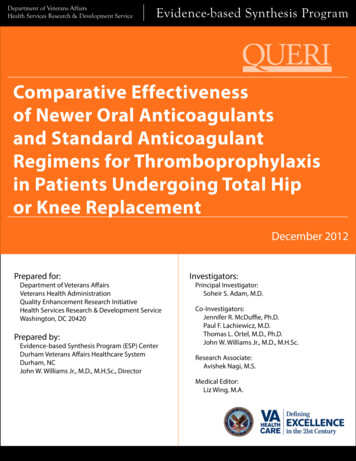
Annals of Surgery Volume 265, Number 1, January 2017Post-discharge Venous Thromboembolism After Bariatric Surgerywho developed VTE during their original hospital stay, we identified269 (0.29%) patients who suffered from postdischarge VTE. Compared with those with no VTE, the mean age of the postdischargeVTE patients was higher (48.03 vs 44.99 years old; P 0.001). Thepercentage of males among postdischarge VTE patients (34.20%)was higher compared with non-VTE patients (20.87%; P 0.001).Mean BMI was 49.16 kg/m2 in postdischarge VTE patients and45.90 kg/m2 in non-VTE patients (P 0.001).Selected perioperative characteristics of the study cohortare presented in Table 2. Overall postoperative mortality was0.10% (N ¼ 95). Among those with postdischarge VTE, themortality rate was 2.60% (N ¼ 7) compared with 0.09% (N ¼86) among those with no 30-day postoperative VTE (P 0.001).Patients with postdischarge VTE had a significantly higher proportion of ASA classes III and IV (75.47%, N ¼ 203) compared withthose patients with no VTE (65.52%, N ¼ 60,016; P ¼ 0.006). Thefrequencies of RYGB were similar between patients with postdischarge VTE (59.11%) and those with no VTE (57.16%; P ¼ 0.520).The frequency of SG was higher in the VTE group (23.05%)compared with non-VTE patients (13.48%; P 0.001) and thefrequency of AGB placement was higher in the non-VTE (26.87%)compared with postdischarge VTE patients (9.29%; P 0.001).Higher frequencies of BPD-DS and revisional surgeries werefound in postdischarge VTE patients (5.20% and 3.35%) comparedwith non-VTE patients (1.42% and 1.07%; P 0.001), respectively.Compared with RYGB, AGB was associated with lower riskof postdischarge VTE (OR ¼ 0.33; 95% CI 0.22–0.51), but SG(OR ¼ 1.65; 95% CI 1.23 –2.22), BPD-DS (OR ¼ 3.54; 95% CI2.04 –6.13), and revisional surgery (OR ¼ 3.03 95% CI 1.54–5.94)were associated with a higher risk of postdischarge VTE. Finally,mean LOS was also higher among patients with postdischargeVTE (2.69 days) compared with those with no VTE (1.88 days;P 0.001).Of the 45 examined variables, the final risk assessment modelfor prediction of postdischarge VTE contained 10 categorical variables including history of CHF (OR ¼ 6.58; 95% CI 1.95–22.20),paraplegia (OR ¼ 5.71; 95% CI 1.36–24.02), return to operatingroom (OR ¼ 5.11; 95% CI 3.25–8.04), dyspnea at rest (OR ¼ 3.95;95% CI 1.57–9.95), nongastric band surgery (OR ¼ 2.44; 95% CI1.55–3.85), age 60 years (OR ¼ 1.96; 95% CI 1.39–2.75), malesex (OR ¼ 1.92; 95% CI 1.44–2.57), BMI 50 kg/m2 (OR ¼ 1.67;95% CI 1.26–2.23), LOS 3 days (OR ¼ 1.58; 95% CI 1.16–2.14),and operative time 3 hours (OR ¼ 1.57; 95% CI 1.13–2.18)(Table 3). The calculated multiple logistic regression equationwas the following:L ¼ 7.337þ(congestive heart failure 1.883)þ(paraplegia 1.743)þ(return to operating room 1.631)þ(dyspnea at rest 1.375)þ(non-gastric band surgery 0.893)þ(age 60 years 0.67)þ(male sex 0.655)þ(BMI 50 kg/m2 0.516)þ(postoperative hospitalstay 3 days 0.455)þ(operative time 3 hrs 0.451).TABLE 1. Selected Baseline Characteristics of the Study CohortPatient CharacteristicAge (yrs) – mean SDSex (male) – N (%)Weight (kg) – mean SDBMI (kg/m2) – mean SDRace – N (%)WhiteBlackFunctional status – N (%)Partially or totally dependentSmoker – N (%)DM – N (%)HTN – N (%)Dyspnea – N (%)On exertionAt restCHF – N (%)CAD – N (%)yTIA/CVA – N (%)zPVD – N (%)§ParaplegiaCOPD – N (%)Steroid/Immunosuppressant use – N (%)Preoperative blood testHematocrit (%) – mean SDAlbumin (g/dL) – mean SDCreatinine (mg/dL) – mean SDPlatelets (109/L) – mean SDStudy Cohort N ¼ 91,963Postdischarge VTE N ¼ 269No VTE N ¼ 91,640P45.01 11.6219,169 (20.91)127.28 26.2545.91 7.9048.03 11.3692 (34.20)140.94 32.3449.16 9.6144.99 11.6219,059 (20.87)127.23 26.2245.90 7.90 0.001 0.001 0.001 0.0010.00168,099 (74.05)13,456 (14.63)180 (66.91)61 (22.68)67,876 (74.07)13,389 .14)(0.19)(0.09)(1.59)(0.96) 0.0010.1130.6910.007 0.0010.0050.10540.18 3.484.10 0.410.92 0.42278.38 69.790.217 0.0010.2070.0120.59540.18 3.484.09 0.410.92 0.42278.35 69.7840.46 3.503.96 0.440.95 0.26267.15 68.090.9220.2300.0040.001BMI indicates body mass index; CAD, coronary artery disease; CHF, congestive heart failure; COPD, chronic obstructive pulmonary disease; CVA, cerebrovascular accident; DM,diabetes mellitus; HTN, hypertension; PVD, peripheral vascular disease; SD, standard deviation; TIA, transient ischemic attack; VTE, venous theomboembolism. As the focus is only on postdischarge VTE, we have excluded the 54 patients who developed VTE during the original hospital stay from the subgroup analysis.yThis is a binary variable representing the occurrence of any history of angina within 1 month before index surgery, history of myocardial infarction within 6 months before surgery,any previous percutaneous cardiac intervention, or any previous cardiac surgery.zThis is a binary variable representing any history of transient ischemic attacks, or any cerebrovascular accidents irrespective of the presence of any neurological deficit.§This is a binary variable representing any history of revascularization or amputation for peripheral vascular disease, or the presence of rest pain or gangrene.ß2016 Wolters Kluwer Health, Inc. All rights reserved.www.annalsofsurgery.com 145Copyright 2016 Wolters Kluwer Health, Inc. All rights reserved.
Annals of Surgery Volume 265, Number 1, January 2017Aminian et alTABLE 2. Perioperative characteristics of the study cohort stratified on the occurrence of post-discharge VTEStudy Cohort N ¼ 91,963VariableASA Class y – N (%)(1)– No Disturbance(2) – Mild Disturbance(3) – Severe Disturbance(4) – Life-threateningOperation type – N (%)AGBSGRYGBBPD-DSRevisionalOperation time (minute) – mean SDAGBSGRYGBBPD-DSRevisionalLOS (day) – mean SDReturn to operating room – N (%)Mortality – N (%)Post-discharge VTE N ¼ 269No VTE N ¼ ,3831303979(26.87)(13.48)(57.16)(1.42)(1.07) 0.001 0.0010.520 0.001 0.00169.10 32.19100.43 48.10135.03 55.66176.36 94.33199.63 101.451.88 1.211593 (1.74)86 (0.09)0.0070.0050.0070.6310.769 0.001 0.001 0.00169.11 32.21100.55 48.16135.08 55.68176.24 94.18200.13 101.741.88 1.221625 (1.77)95 (0.10)86.56 47.00117.66 55.54147.00 62.90164.21 83.48189.67 76.872.69 1.6428 (10.41)7 (2.60)AGB indicates adjustable gastric banding; ASA, American Society of Anaesthesiology; BPD-DS, biliopancreatic diversion-duodenal switch; LOS, length of stay; RYGB, Roux-enY gastric bypass; SD, standard deviation; SG, sleeve gastrectomy; VTE, venous theomboembolism. As the focus is only on postdischarge VTE, we have excluded the 54 patients who developed VTE during the original hospital stay from the subgroup analysis.yPatients categorized as ASA class 5 (Moribund) at the time of the index surgery have been excluded from the study cohort.The estimated probability of 30-day postdischarge VTE for agiven patient is calculated using the following formula:Estimated probability of composite adverse event (100%)¼EXP [L] / (1þ EXP [L]).The notation EXP is equivalent to ex, where ‘‘e’’ is the base ofnatural logarithm (2.718). The model demonstrated a good calibration (Hosmer-Lemeshow goodness-of-fit test, x2 ¼ 4.58; P ¼0.711) and discrimination (c-statistic ¼ 0.741).The generated risk model based on 2007–2012 ACS-NSQIPwas subsequently validated on the validation dataset (2013, N ¼20,575), which showed a relatively similar performance (c-statistic ¼0.66; 95% CI 0.59–0.73). Of note, data of ‘‘paraplegia’’ was notavailable in the validation dataset, which could negatively affect themodel performance.On the basis of the regression equation and the parameterestimates listed in Table 3, a risk calculator for postdischarge VTEwas developed. A user-friendly version of the risk calculator isaccessible at http://www.r-calc.com under the bariatric surgeryformula tab. When the required values are entered into the calculator,the percent estimate of postdischarge VTE after bariatric surgery iscalculated. A few examples on the estimated probability of postdischarge VTE:Estimated risk in a healthy young woman with BMI of 40 kg/m2 undergoing uncomplicated RYGB would be 0.16%.Estimated risk in 63 years old man with BMI of 60 kg/m2undergoing SG with a postoperative LOS of 5 days would be 1.56%.Estimated risk in 48 years old woman with BMI of 38 kg/m2 andpreoperative dyspnea undergoing RYGB which needed reoperationand a prolonged LOS for a surgical complication would be 4.82%.Performance of the risk assessment tool at different cut-points hasbeen shown in Table 4. For example, cut-point 0.2% includes 50% ofpatients with a sensitivity of 82% and specificity of 50% for prediction ofpostdischarge VTE. With increasing cut-point to 0.5%, the percentageof included patients decreases to 12% along with a reduction insensitivity to 43% and an increase in specificity to 88%. Nearly 2.5%of patients had a predicted postdischarge VTE risk 1%.BMI 50 kg/m2 alone was a poor predictor of postdischargeVTE (c-statistic ¼ 0.60) with a sensitivity of 40% and a specificity ofTABLE 3. Predictive Factors of Postdischarge VTE Based on Multivariate AnalysisRisk FactorCrude ORCHFParaplegiaReturn to operating roomDyspnea at restNongastric band surgeryAge 60 (yrs)MaleBMI 50 (kg/m2)LOS 3 (day)Operation Time 3 sted OR 0.170.150.150.160.17BMI indicates body mass index; CHF, congestive heart failure; CI, confidence interval; LOS, length of stay; OR, odds ratio; SEE, standard error of estimate; VTE, venousthromboembolism.146 www.annalsofsurgery.comß2016 Wolters Kluwer Health, Inc. All rights reserved.Copyright 2016 Wolters Kluwer Health, Inc. All rights reserved.
Annals of Surgery Volume 265, Number 1, January 2017Post-discharge Venous Thromboembolism After Bariatric SurgeryTABLE 4. Performance of Risk Calculator in Various Cut-points to Detect Postdischarge VTECut-point 0.2% 0.3% 0.4% 0.5% 0.75% 1% 3%For Comparison:BMI 50 kg/m2Patients Included (%)Sensitivity (%)Specificity (%)Youden’s J 36333126172.524407515BMI, Body Mass Index; VTE, Venous Thromboembolism. Youden’s J index is a statistic that captures the accuracy performance of a diagnostic test in conjunction with Receiver Operating Characteristic (ROC) analysis which is used toidentify the best cut-point and is obtained using the following formula: sensitivityþspecificity 1.75%. Predictive ability of the proposed model was significantlybetter than BMI alone (P 0.001). Likelihood ratio test also showedthat the full model was superior to BMI alone (P 0.001).DISCUSSIONPulmonary embolism is a major cause of postdischargemortality after bariatric surgery.5,6 Hence, occurrence of VTE inthe postoperative period especially after the patient is dischargedfrom the hospital is a highly feared complication particularly afterelective procedures such as bariatric surgery. We found that theprevalence of post-discharge VTE was 0.29% among patients whounderwent bariatric surgery between 2007 and 2012 and even thoughthe mortality rate of the entire cohort of patients was an acceptablevalue of 0.1%,20,21 those who suffered from a postdischarge VTE hada significantly higher mortality rate of 2.60%.We also found that patients who developed postdischarge VTEas compared with those with no VTE were older black males with ahigher BMI, who had a higher prevalence of dyspnea at rest, CHF,PVD, paraplegia, and COPD at baseline. In addition, they hadsignificantly higher ASA scores, underwent lengthier operationsand had more BPD-DS and revisional procedures, stayed in thehospital longer, and needed more reoperations. Moreover, afterthe multivariate analysis, we found 10 major risk factors forpostdischarge VTE all of which increased the risk of VTE by atleast 1.5-fold and subsequently were used to generate a risk calculator. CHF was found to be the strongest independent predictorincreasing the likelihood of postdischarge VTE by near seven-fold,followed by the presence of paraplegia (near 6-fold), 30-day return tothe operating room (more than five-fold), and dyspnea at rest thatindependently accounted for a near four-fold increase in the likelihood of postdischarge VTE. Age greater than 60 years, male sex,super-obesity (BMI 50 kg/m2), procedures other than AGB placement, longer operation ( 3 hrs), and lengthier index hospital stay( 3 days) were also found to be independent risk factors forpostdischarge VTE.Historically, there have been a few VTE risk assessmentmodels, such as Kucher,22 Rogers,23 Caprini,24 Pannucci,25 andScarborough models,26 that are either considered accurate assessment tools for higher-risk patients only, complex to use with toomany predictors, or created using only vascular surgery patientswhich would limit their use for other surgical procedures such asbariatric surgery.Merkow et al27 identified predictors of post-discharge VTE inpatients undergoing cancer surgery using ACS-NSQIP data and afterdemonstrating that over 33% of all VTE events occurred postdischarge, advocated for extended prophylaxis in higher-riskß2016 Wolters Kluwer Health, Inc. All rights reserved.patients. Winegar et al13 also evaluated the 90-day VTE events afterbariatric surgery using the Bariatric Outcomes Longitudinal Database and found that greater than 70% of VTE events ensued after thepatient was discharged; furthermore, the majority of the occurrencesfell within the 30-day period. In our current study, 80% of postbariatric surgery VTE events occurred postdischarge. Thus, it isimportant to identify risk factors for VTE after discharge so patientswith a higher risk profile could theoretically benefit from a moreaggressive prophylaxis.To our knowledge, our study is the first to evaluate thesepredictors and generate a risk calculator for postdischarge VTEevents in patients undergoing primary and revisional bariatricsurgery using a large multicenter database. Our results are consistentand have expanded on the findings from the study by Finks et al15which using the Michigan Bariatric Surgery Collaborative databasecreated a risk calculator for all postoperative VTE events postbariatric surgery. Like our study they identified higher age andBMI, male sex, longer surgery ( 3 hours), and non-AGB placementprocedures along with a prior history of VTE as independent riskfactors for postoperative VTE. However, our study identifiedadditional strong cardiopulmonary risk factors in CHF, dyspnea atrest, and paraplegia as a marker of immobility all of which have beenrecognized in other postsurgical VTE risk assessment models.26– 28In addition, unlike the study by Finks et al the accuracy andperformance of our risk calculator was internally validated usingthe 2013 ACS-NSQIP database. Using the ACS-NSQIP data, whichis a robust clinical, validated, and audited database, enabled us toconsider multiple perioperative variables from a large sample size ofpatients from both the academic and community centers. The userfriendly online version of this calculator can assist in risk assessmentand decision making.Choosing a particular cut-point on estimated risk of postdischarge VTE to guide extended pharmacoprophylaxis can be arbitrary. By choosing a lower cut-point, which is associated with ahigher sensitivity but lower specificity (Table 4), a higher percentageof patients will receive extended prophylaxis that may in turntranslate into higher costs and adverse events such as bleeding.In our opinion, a risk 0.4% can be a reasonable indication forextended pharmacoprophylaxis: 20% of patients would need postdischarge prophylaxis with sensitivity, specificity, and Youden’s Jindex of 53%, 80%, and 33. Compared with BMI 50 kg/m2 alone,which some bariatric centers use as a criterion for extended pharmacoprophylaxis, the former provides higher sensitivity (53% vs40%) and specificity (80% vs 75%), whereas impacting fewerpatients (20% vs 24%). Overall, cut-point of risk 0.3 has thebest performance (Youden’s J index ¼ 36), but include almostone third of bariatric patients and 40% of nongastric band patients.www.annalsofsurgery.com 147Copyright 2016 Wolters Kluwer Health, Inc. All rights reserved.
Annals of Surgery Volume 265, Number 1, January 2017Aminian et alA predicted risk 1% can represent 2.5% of patient population whoare very high risk to develop postdischarge VTE (specificity ¼ 97%).Therefore, the threshold depends on how aggressive versus howconservative the physicians want to offer prophylactic anticoagulation. In considering extended pharmacoprophylaxis, predicted risk ofVTE, potential benefits, and possible complications (including therisk of bleeding) of available medications, and cost should be takeninto account.Once the higher-risk patients for postdischarge VTE areidentified, the question remains as to how to adequately carry outVTE prophylaxis beyond their hospital stay. No clear consensusexists on the choice, dosing, and duration of thromboprophylaxisafter bariatric surgery.29,30 A large literature review by Huo et al31showed that low-molecul
deep vein thrombosis (DVT) are 1-3% and 0.3-2% for pulmonary embolism (PE).7-10Given the significant VTE risk in these patients, both the American College of Chest Physicians and the American Society for Metabolic and Bariatric Surgery have recommended that in addition to mechanical prophylaxis some form of pharmacopro-