Transcription
CCTP Experience atScripps Health Care SystemSusan Erickson RN, MPHSenior Director Patient NavigationDecember 13, 20131
Transition from Traditional CaseManagement to Care Management ModelCCTP is part of a broader initiative at Scripps Navigators: EDInpatientOutpatient Ambulatory Interdisciplinary Team: MD MTM Pharmacist Navigator Bedside Rounds– Goal boards in room – patient friendly language– Milliman Guidelines utilized for goal LOS, D/C barriers Follow patient for 30 days post acute care discharge (CTI ON) Evaluation of outcomes: LOS, Readmissions, Patient SatisfactionConfidential2
Community Care TransitionsProgramGOAL: Decrease 30 Day Readmissions forMedicare FFS PatientsFOCUS at Scripps:– Increase Footprint Documentation– Understand Causes of Readmissions(Readmission RCA)– Enhance Screening Capability
Increasing FootprintMONTH ENCOUNTERS256249292393740664Staffing Changes670628
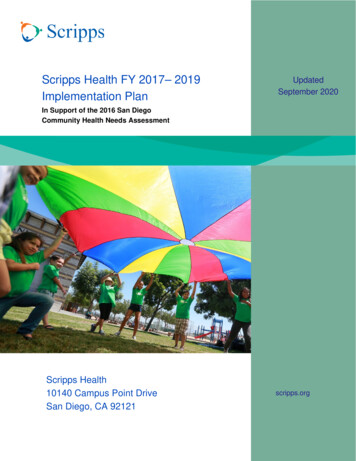
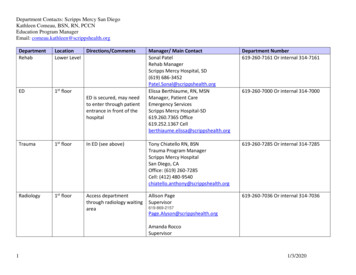
CCTP Footprint TrackingNov. 1 - 11Nov. 12 - 15Nov. 16-22Nov. 23-30Dec. 1%82.1%82.4%84.1%La Jolla50.4%44.2%45.8%56.2%55.0%Chula Vista75.3%64.9%84.5%83.3%91.7%Mercy 0.0%20.0%0.0%EncinitasNov. 1 - 11Chula VistaNov. 12 - 15GreenNov. 16-22Mercy SDLa JollaNov. 23-30System AverageDec. 1-6SystemAverage62.5%61.0%64.9%74.2%76.6%
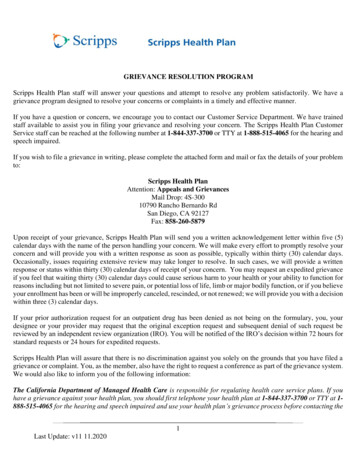
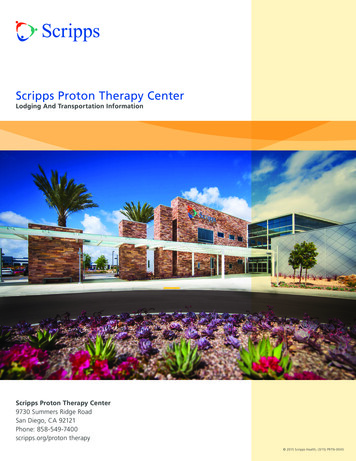
Readmission Root CauseAnalysis (RCA) ProcessReadmissionsList GeneratedCM / Navigator Interviews Patientin Real Time, Reviews Chartand discusses with MD/PharmacistDecreasedReadmissions!Meeting at System Level2-3x/yr to Review Trends andIdentify Opportunities/StrategiesFindings Entered intoCommon Midas DatabaseQuarterly Hospital SpecificData Review & Presentationto Site UR/UM Committee
30-day ReadmissionRoot Cause Analysis (RCA)InitiativeStatsInitial Study Period:Total # of readmissions:% of surveys completed:1/14/13-8/14/134,03560.5% (2,441)Dr. Adam Ellis
Timing of ReadmissionsKey Findings: Days 0-5 post-discharge most vulnerable: 33%of readmissions system-wide 55% of readmissions within 10 days ofdischarge (steady decline thereafter)– 80-89 year olds at greatest risk during 10 day window– Medicare A/B beneficiaries disproportionally affectedduring days 6-10 Goal is for every high-risk patient to be discharged with1 appointment in hand for follow up within 7 days ofdischarge– Pilot post-discharge ‘transition clinic’ at Scripps Encinitas
Ambulatory Care Follow-UpPrior to ReadmissionKey Findings: 20 % of patients had not seen an outpatientphysician prior to being readmitted 42.6% readmitted on days 6-30 post-dischargehad not seen an outpatient physician– Medicare A/B patients disproportionally affected New survey to examine effectiveness ofpatients leaving the hospital with at least 1follow up appointment in hand
Readmission Frequent Flyer ClubKey Findings: 21.5% of patients readmitted had 2 or morereadmissions during the first four months ofstudy Future analysis of ‘poly-readmitters’ (e.g.3 readmissions) by diagnosis, age andpayer-type Higher level of care management for highutilizers
Root Cause of Readmission1/14/13-4/14/13N 971 surveysWorsening illness:New Illness:Other:Medication related:Misc. (combined):Non-compliance:35%24%19.1%8.3%7.3%6.3%
30-day ReadmissionRoot Cause Analysis (RCA)InitiativeSuccesses Clear picture of:– who’s coming back age primary coded diagnosis primary payerChallenges Initial survey:– root cause question not specificenough (e.g. ‘worseningillness’)– allowed use of ‘other’ asresponse– when they’re coming back– how often they’re coming back Subjectivity of preventabilitydesignation– follow up with an outpatient MDbefore readmission Time constraints of Inpatient– readmission rates of top 5 NavigatorsSNFs for each hospital– some questions left blank– degree of readmission Not digging deep enoughpreventability
Enhancing Case Finding:360Fresh13
Scripps Health Care System Susan Erickson RN, MPH Senior Director Patient Navigation December 13, 2013 . Follow patient for 30 days post acute care discharge . Encinitas Green La Jolla Chula Vista Mercy SD System Average Nov. 1 - 11 89.7% 80.6% 50.4% 75.3% 16.5% 62.5% .