Transcription
Basics ofLocal Human Services
OverviewPublic HealthSocial ServicesConsolidatedHumanServicesMH/DD/SA
Plan General overview of each area Functions What does the agency do? Relationships What is the relationshipbetween the BCC and the director? Thegoverning board? Mock budget workshop Looking ahead
PUBLIC HEALTH
QuestionsFunction What does theagency do?Relationships Between BCCand the director? Between the BCCand thegoverning board?
1854: Cholera in London & theBroad Street water pump6
1980: Worldwide eradication ofsmallpox 1949: Last naturallyacquired case in the US 1977: Last naturallyacquired case in theworld (in Somalia) 1980: Disease declarederadicated
Common threads in the stories Focus on populations, not just individuals Focus on conditions that promote or threaten goodhealth Focus on prevention Evidence-based strategies
What does public health do?Population Assessment Policy Preparation & responseEnvironment Food, lodging, &institutional sanitation Water & wastewater Lead, pests, other risksIndividuals Disease detection,prevention and control Clinical care Service coordination10
Organization of local public health in NCLocal healthdepartmentLocal board ofhealth (BOH)Local healthdirectorCounty health departmentCounty board of health orBCC*Local health directorConsolidated humanservices agencyConsolidated humanservices board orBCC*Consolidated humanservices director**District health departmentDistrict board of healthLocal health directorPublic health authorityPublic health authorityboardPublic health authoritydirectorPublic hospital authority(Cabarrus only)Public hospital authorityboardPublic hospital authoritydirector* Board of county commissioners may assume powers & duties of board** CHS director must appoint person with local health director education/experience
Local Public Health Agencies & BoardsApril 2019County health department with county board of health (48)County health department governed by board of county commissioners (Graham, Jackson, Stokes, Sampson, Pamlico) (5)District health department with district board of health (6 districts delineated by different shades of purple) (Yancey, Mitchell,Avery; Rutherford, McDowell (includes Polk until 7/1/19); Watauga, Ashe, Alleghany; Granville, Vance; Hertford, Bertie, Gates, Chowan,Perquimans, Pasquotank, Camden, Currituck; Martin, Tyrrell, Washington) (21)Consolidated human services agency with consolidated human services board (Haywood, Buncombe, Polk (eff. 7/1/19), Gaston, Davie,Union, Forsyth, Stanly, Rockingham, Wake, Nash, Edgecombe, Carteret, Dare) (14)Consolidated human services agency governed by board of county commissioners (Clay, Swain, Yadkin, Mecklenburg, Guilford,Montgomery, Richmond, Bladen, Brunswick, Pender, Onslow) (11)Public hospital authority with hospital board authorized to act as board of health (Cabarrus) (1)
BOH Statutory Powers & DutiesRole: “protect and promote thepublic health”Powers and duties: Appoint the local health director Make policy for local public health agency Adopt local public health rules Adjudicate disputes regarding local rules or locally imposedpublic health administrative penalties (fines) Impose local public health fees Satisfy state accreditation requirements for BOHs13
Local Health Director Powers & DutiesG.S. 130A-41Elsewhere in GS 130A Administer PH programs Hire/dismiss employees Enforce PH laws & employ legalremedies Investigate & control communicablediseases & rabies Investigate other diseases Disseminate PH information andpromote health Advise local officials on healthmatters Enter contracts (subject toBCC/manager oversight) Rabies vaccination clinic Isolation & quarantine authority Access to records Etc.Elsewhere in GS Approve jail medical plan Relocation of graves Etc.Other Compliance, budget, etc.14
Summary of BCC actionsEstablish agencyEstablish boardApprove budget BCC decides public health agency type Appointed BOH or consolidated human services (CHS)board: BCC has role in appointing board members Each type of appointed board has at least one countycommissioner member Direct exercise of BOH role: BCC may assume BOH powers and duties in a countywith a county health department or a consolidatedhuman services agency that includes public health BCC approves agency budget, including any local feesimposed by BOH or CHS board BCC appropriates local funds15
SOCIAL SERVICES
QuestionsFunction What does theagency do?Relationships Between BCCand the director? Between the BCCand thegoverning board?
Fred Fred is 84. He livesalone, walks with acane and has milddementia. Fred’s daughter, Beth,lives out of state. She isworried that an inhome aide may befinancially exploitingFred.
Susan DSS receives a call fromSusan, who is a nurse in apediatrician’s office. The nurse explains that ayoung child is beingtreated in the office andhas many suspiciousbruises.
Karen Karen is a single momwith three children The father of heryoungest is refusing topay child support She needs the money topay for child care for theinfant so she can returnto work20
Claudia Claudia is a widow wholives in a smallapartment. She receives a smallpension but it is oftennot enough to cover herbasic expenses. She usually eats only onemeal a day.
Common Threads Protection Child protective services Adult protective services Support Economic services Transportation Oversight Licensure and inspectionImage: http://www.maconnc.org/dss-adult-abuse.html
What does DSS do?Catawba County Annual Report 2014
Intergovernmental: Who doeswhat?FederalStateLocal24
Example of Roles – APS FundingPolicyImplementFederalStateLimited – someblock grantVery limitedfundsSignificant –Limited – tiedlegislation,to grantregulations,fundingpolicy, oversightNoneLimited tosupervisionCountySignificantLimitedSignificant
Organization Single county DSS Regional DSS Consolidated humanservices agency Other options Share director Interlocal agreement forregional departments orshared services26
BCC Governing BoardSome Serve as governing board Appoint all members of the governingboard (CHSB)Some Appoint 2 members of a 5 membercitizen governing board (or 1 of 3)Some
BCC DirectorSome Hire & supervise directorSome Manager hires & supervises director, with advice& consent of appointed governing board (CHSB)Some Appointed governing board hires & supervisesdirector
CONSOLIDATED HUMANSERVICES
Is this alServices
What is Being Consolidated? Two or more county programs that provide humanservices “Human services” not defined Most include public health and social services but theyare not required to do so May include other human services such as aging,transportation, and veterans’ services May not include LME/MCO Level of integration/consolidation varies across thestate
G.S. 153A-77 Options12Board ofCountyCommissionersBoard of CountyCommissionersConsolidated HumanServices BoardDepartment ofSocial ServicesConsolidated HumanServices Agency3Board of CountyCommissioners as aConsolidated HumanServices BoardConsolidated HumanServices Agency32
PH and SS Organization and GovernanceJune 2012Not consolidatedConsolidated human services agency (CHSA)with a consolidated human services board (Wake)CHSA with BOCC as governing board (Mecklenburg)33
PH and SS Organization and GovernanceResolutions as of April 2019SS & PH agencies with appointed governing boardsOption 1 with both SS & PH agencies governed by BOCC (Graham, Jackson,Stokes, Sampson)Option 1 with SS agency governed by BOCC, PH agency with appointedgoverning board (Cherokee, Ashe, McDowell, Cleveland, Mitchell, Watauga, Wilkes, Surry, Columbus)Option 1 with PH agency governed by BOCC, SS agency with appointed governing board (Pamlico)Option 2 with consolidated HS agency including SS & PH, appointed CHS board (Haywood, Buncombe, Polk (eff. July 1), Gaston, Davie,Union, Forsyth, Stanly, Rockingham, Wake, Nash, Edgecombe, Carteret, Dare)Option 3 with consolidated HS agency including SS & PH, governed by BOCC, health advisory committee (Clay, Swain, Yadkin, Mecklenburg[no advisory comm.], Guilford, Montgomery, Richmond, Bladen, Brunswick, Pender, Onslow)Option 3 with consolidated HS agency including SS & other human services but not PH, governed by BOCC (Cabarrus)34
Key DifferencesBoardHire Agency DirectorDSSAppointed;3-5 mem.Board hiresSHRAPHAppointed;11 mem.Board hiresSHRAOneElected*BOCC hiresSHRATwoAppointed;Manager hires with advice & SHRAup to 25 mem. consent of CHS boardOptionalThree Elected*Manager hires with advice & SHRAconsent of BOCCoptional* If public health affected, must appoint health advisory committee35
CHSB Powers and Duties1. Assume powers and duties of board ofhealth and social services board2. Assigned additional duties by law3. County vision may be more expansive
Motivations for Change Improve service delivery forcitizens Create a new vision for humanservices programs Create a unified personnel systemfor all county personnel Change the relationship betweenboard of county commissionersand the departments Identify efficiencies and reducehuman services spending
Other Options Remain Single county PH and/or DSS Multi-county PH and/or DSS Interlocal agreements for shared services orcollaboration Counties may share a DSS director Functionally integrate in many ways withoutmaking changes to organization and governance
MENTAL HEALTH, DEVELOPMENTALDISABILITIES, AND SUBSTANCEABUSE SERVICES
Terminology and Acronyms Acronyms MH mental healthDD developmental disabilitiesIDD intellectual and developmental disabilitiesSA substance abuseSU substance useSUD substance use disorderCEO area director director of the MH/DD/SA authority North Carolina public mental health authority Area MH/DD/SA AuthorityArea AuthorityLocal Management Entity (LME)Managed Care Organization (MCO)LME/MCO The public entity responsible for managingMH/DD/SA services paid for with public funds
QuestionsFunction What does theagency do?Relationships Between BCCand the director? Between the BCCand thegoverning board?
What does an LME do?Local management entities are responsible for themanagement and oversight of the public system ofMH/DD/SA services at the community level.An LME shall plan, develop, implement, and monitorservices within a specified geographic area to ensureexpected outcomes for consumers within availableresources.G.S. 122C-115.4
LME-MCO RegionsMap courtesy of Sandhills Center
Who pays for services?State andFederal Block County OtherGrant2%1%17% 369 millionMedicaid80%Vaya Health (Smoky Mountain Center )FY 2015-16 Budgeted Revenues By Source
Where does the money go?Admin.11%Risk Reserve1% 360.5millionServices88%Vaya Health (Smoky Mountain Center)FY 2015-16 Budgeted Medicaid/State/Federal Revenues
Managing Care Managing the quality of care Managing the cost of careLMEDoctorPatient
LME-MCO Functions*AccessProvider Relations capacityenrollmentmonitoring*Service Management authorizationutilizationcare coordinationQuality Management*Community Collaboration
Access and Service AuthorizationLME Call deServicesPersonCentered PlanServiceAuthorization
Service ManagementApprove specific services toindividual consumers—“service authorization” Evaluate the medical necessity, clinicalappropriateness, and effectiveness of servicesaccording to state criteria—“utilizationmanagement” Monitor individual care decisions at criticaltreatment junctures to assure effective care isreceived when needed—“care coordination”
Service ManagementLME Eligible individual? Covered service? Based on clinical assessment? Medically necessary? Qualified provider? Evidence that treatment helps? Other needed services? Outcomes over time?LMEMCOProvider
Community CollaborationThe LME must establish and maintain effectivecollaborative working relationships with otherpublic agencies, health care providers, and humanservices agencies within its catchment areaRecommendation—Ask your LME how they arecollaborating with other agencies, includingsocial services, juvenile justice, communityhospitals, and the courts.
Collaborative ealthCareProvidersSchoolsOthers52
LME-MCO OrganizationDirector Planning Implementing Monitoring
Counties Establish the Agency Two or more BCCs jointly must establish an areaauthority with approval of DHHS Secretary A county may “disengage” from one LME and“realign” with another with Secretary approval Two area authorities may consolidate (merge) tocreate one larger area authority with SecretaryapprovalG.S. 122C-115.54
Counties Appoint the Governing BoardBCCs within the LME’s catchment area must appoint members according to a plan jointly adopted byparticipating counties that describes the boardcomposition, and appointment and selection processLME board statute requires At least 11 and no more than 21 voting members 11 prescribed categories of professional and constituentrepresentationG.S. 122C-118.1, 122C-115.255
Adopt an LME Business PlanEach county through its area authority mustdevelop, review, and approve a business planfor the management and delivery of servicesthat addresses Planning to identify service gaps and ways to fillthose gaps Collaboration with other local service systems toensure access to and coordination of servicesG.S. 122C-115.256
Other County Roles Appropriate funds Provide input—annual review of area director Developing and maintaining effective relationships withthe community served and with state and local officials Appoint a commissioner to the countycommissioner advisory board Assess LME’s capacity to meet service needs Quarterly service delivery reports Annual progress report57
LME-MCO Reporting to Counties Quarterly service delivery reports that assess thequality and availability of services Annual progress report assessing the LME’s abilityto meet the service needs of its catchment area Quarterly financial reports Approved budget and annual audit Submission is for informational purposes. An LME-MCOis a “public authority” under G.S. 159 and is responsiblefor its own budgeting and fiscal control.58
Mock Human ServicesBudget Work Session
Budget TimelineJanuaryMid-YearReviewMaySchool Budget &Work SessionsFebruaryDepartmentHeads/ManagerJunePublic portJulyBudget Adopted
County Expenditures by Function Statewide Average Coates CountyChart TitleOther16%PublicSafety17%GeneralGovernment16% 2018-19 AFIREducation19%DebtService16%HumanServices16%
MEETINGS! MEETINGS! MEETINGS!Jason King, Education DirectorNCACC So much to learn! So manymeetings! The Manager isyour FRIEND!Neil Emory, NCACCOutreach Associate
Coates County HealthDepartment OverviewLayton Long, Public Health Director
Coates County Health DepartmentPrograms & ServicesHealth Promotion and Policy AdministrationEnvironmental Health Permitting and InspectionsClinical ServicesAnimal Services
Public Health Reality MomentJill D. MooreAssociate Professor of PublicLaw and GovernmentLayton LongPublic Health DirectorChatham County Local Health Departments vary greatly in the servicesand programs they offer Some departments are moving away from theprovision of clinical services
NC Health Department ServicesHealth department must provide: Environmental health services (inspections& permitting) Communicable disease control Vital records servicesHealth department must provide,contract for, or assure: Adult healthHome healthDental public healthMaternal healthChild healthFamily planningPublic health laboratory
Coates County Health DepartmentFY2019 Estimated Revenues & Administration7%23%16%Animal Services25%Health Promotion& PolicyAnimal Services15%15%Clinical ServicesHealth Promotion& PolicyClinical th
Public Health Reality MomentJill D. MooreAssociate Professor of Public Lawand GovernmentLayton LongPublic Health DirectorChatham County “The patient is the community” Controlling disease outbreaks Promoting health Assuring safe water, food, etc. throughenvironmental health functions
Questions?
Coates County SocialServices DepartmentOverviewNancy Coston, Social Services Director
Coates County Social ServicesPrograms & Services Services for Children & Families Adoption Child Welfare (CPS & Foster Care) Independent Living for FosterChildren Work First Family Assistance Adolescent Parenting Program Services for Adults Adult Protective ServicesGuardianshipAdult DaycareIn-Home AidPlacement ServicesRepresentative PayeeServices for the BlindVeterans Services Economic Services Adult MedicaidEmergency AssistanceFamily & Children’s MedicaidFood & Nutrition ServicesLIEAP (Energy Assistance) Employment Services Work First Employment and Training On-the-Job Training Administration Staffing, financial support, &operations
Social Services Reality MomentAimee N. WallProfessor of Public Lawand GovernmentNancy Coston, DirectorOrange County Departmentof Social Services County-by-county variation Most programs are available statewide but thereare some local programs Counties have adopted different approaches toorganization and governance The role of the Board of Commissioners varies
Social Services ProjectedExpenditures FY2019
Social Services Reality MomentAimee N. WallProfessor of Public Lawand GovernmentNancy Coston, DirectorOrange County Departmentof Social Services Pressure points System reform and federal oversight Data/NCFAST/Dashboard Workforce Medicaid Transformation Demographic trends
Questions?
The Sandhills Center LocalManagement Entity/ManagedCare OrganizationVictoria Whitt, Executive Director
The Alphabet Soup of our System LME/MCO Local Management Entity/ManagedCare Organization North Carolina’s public authority responsible forcommunity-based MH/IDD/SA services MH Mental Health IDD Intellectual & Developmental Disabilities SA Substance Abuse PMPM Per member per month the way theState allocates Medicaid money to LME-MCOs
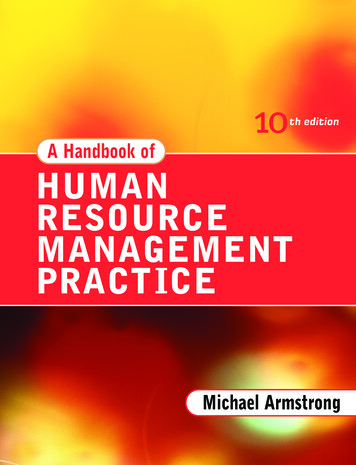
COATES COUNTY MEMBERS SERVED – In Calendar Year 2018Most Frequent Behavioral Health Services ReceivedLast Calendar YearService( 14,926,932 total)Innovations ServicesIntermediate Care FacilitiesOutpatient ServicesIntensive In-Home ServicesInpatient HospitalizationPsychiatric Residential Treatment FacilitiesBehavioral Health Long Term ResidentialAssertive Community Treatment TeamHighest Serving Behavioral Health ProvidersLast Calendar YearProvider(223 providers serving local members)Daymark Recovery ServicesAdvanced Behavioral Center, Inc.VC & Associates, Inc.Therapeutic Alternatives, Inc.Central Carolina HospitalCarolina Behavioral Care, P.A.UNC at Chapel Hill Faculty PhysiciansMembers Served80522419515214011197AmountPaid 4,622,730 3,703,241 1,666,711 1,083,081 1,015,214 886,883 790,648 258,630
LME-MCO Reality MomentMark BottsAssociate Professor of PublicLaw and Government County Maintenance of Effort
LME-MCO Reality Moment Counties shall appropriate funds for area authority programs. Counties shall not reduce county appropriations andexpenditures for current operations and ongoing programs orservices because of the availability of State allocated funds,fees, capitation amounts, or fund balance to the areaauthority. Counties may reduce appropriations previously appropriatedfor one-time, non-recurring needs.G.S. 122C-115. Recommendation—Ask your LME to talk about the programsor services that wouldn’t be available without county dollars.81
COATES COUNTY MEMBERS SERVED – In Calendar Year 2018Most Frequent Behavioral Health Services ReceivedLast Calendar YearService( 14,926,932 total)Innovations ServicesIntermediate Care FacilitiesOutpatient ServicesIntensive In-Home ServicesInpatient HospitalizationPsychiatric Residential Treatment FacilitiesBehavioral Health Long Term ResidentialAssertive Community Treatment TeamHighest Serving Behavioral Health ProvidersLast Calendar YearProvider(223 providers serving local members)Daymark Recovery ServicesAdvanced Behavioral Center, Inc.VC & Associates, Inc.Therapeutic Alternatives, Inc.Central Carolina HospitalCarolina Behavioral Care, P.A.UNC at Chapel Hill Faculty PhysiciansMembers Served80522419515214011197AmountPaid 4,622,730 3,703,241 1,666,711 1,083,081 1,015,214 886,883 790,648 258,630
LME-MCO Reality MomentEach county through its area authority must develop,review, and approve a business plan for themanagement and delivery of services that addresses Planning to identify service gaps and ways to fill thosegaps Collaboration with other local service systems to ensureaccess to and coordination of servicesG.S. 122C-115.285
Sandhills’ Reinvestment Strategiesin Coates County Specialty Courts—UNCG (contract) Assessment/Treatment Planning—Specialty Courts(contract) Psychiatric Services/Staff Detention – Correct CareSolutions Piedmont Health Services and Sickle Cell Agency –Co-location of Substance Abuse Counselor/LCSW,Van driver and consumer assistance – PHSSCA Access2Care Screening/Kiosks – High Point Libraryand Guilford Public Health Malachi House II – Consumer Supports Triad Medical Group (Integrated Care & Opiate contract)
Questions?
Looking Ahead
MENTAL HEALTH, DEVELOPMENTALDISABILITIES AND SUBSTANCE USEDISORDERS
Medicaid Transformation Currently—Medicaid dollars for MH/DD/SA servicesare allocated by the State to seven public managedcare organizations called LME-MCOs Prepaid, capitated contracts with the state for servicesin a defined geographic region November 2019—Medicaid dollars for physicalhealth services, prescription drugs, long-term care,and MH/DD/SA services will be allocated to privateMCOs Prepaid, capitated contracts with the state for servicesin a defined geographic region Most Medicaid beneficiaries will be enrolled in these“standard” plans
Medicaid Transformation Health Regions
Standard Medicaid Plan Will serve those with lower intensity behavioralhealth needs. LME/MCOs will continue to manage services for thosewith more serious BH/IDD needs. The Standard Plans will be administered by severalcomercial entities. AmeriHealth Caritas Blue Cross and Blue Shield United Healthcare Wellcare Carolina Complete Health (a provider led entity)
July 2021—LME-MCOs beginoperating “Tailored Plans” Specialized Medicaid plans for those with significantbehavioral health and intellectual/developmentaldisabilities needs (“serious” MI, “severe” SA) No more than 7 and no less than 5 Plans will beallowed LME-MCOs Will manage non-Medicaid funding (federal/state/county) Contract with the Standard Plans for coordination ofphysical healthcare for members After 4 years, State contracts for tailored plans willbe competitively bid to non-profits and LME-MCOs
Medicaid Transformation Current: MH, IDD, SA ServicesLME/MCO Future: MH, IDD, SA and physical healthservices for individuals with IDD andserious MH or SA (“Tailored Plans”)Fee forServiceMedicaidMild toModerate MHand SA moves toPrivate MCOMostmove toPrivateMCO Current: physical healthservices, prescription, longterm care Physical, prescription,long term care, MH, SAPrivate MCO (“Standard benefitplans”)
SOCIAL SERVICES
Tremendous Changes UnderwayState efforts System reform (S.L. 2017-41) Child welfare reform Guardianship reform (maybe)Federal oversight Program Improvement Plan (child welfare) Families First implementation (child welfare)Medicaid transformation
Overview – S.L. 2017-41 (H 630)
ContextReform PlanMOUs/CorrectiveActionConsultant proposal for state agency and systemreform; dashboardAgreement b/t counties and state; performancerequirements; failure to comply corrective actionRegionalDepartmentsOption beginning 3/1/19; counties may join togetherto offer some or all services through regional deptsChildren’sCouncilImprove coordination/collaboration/communicationamong publicly-funded child serving agencies
SSWG tyCollaborationRegionalAdministration Improve state supervision of countyadministered agencies through morecoordinated and comprehensive regionalsupervision Options for increasing involvement of localelected officials in county-administeredagencies Legislative and regulatory changes necessaryto improve collaboration between counties Benefits and challenges associated withmandatory regional administration
Local InvolvementChargeWork Identify “options forauthorizing the board ofcounty commissioners tointervene in urgentsituations to assumedirect control of [DSS]prior to the Stateassuming direct controlof administration.” Discussed the fulllifecycle of local socialservices agencyorganization andgovernance Identified options forincreasing involvementfrom local electedofficials as well as othersP. 22-26
Local Involvement - OptionsAgency formationComm’r on governing boardOngoing oversightComposition requirements for Governing boards moreproactivegoverning boardCommunicationGoverning board trainingBOCC trainingBOCC training about budgetPerformance updates fromstate
Local Involvement - OptionsInitial non-compliance/urgent circumstancesNotice from state tocounty officialsAgency updates tocounty officialsExtended non-compliance/urgent circumstancesCounty officials involvedin corrective action planState assumes administrationAfter state restores,BOCC and manager have BOCC re-evaluatesaccess to confidentialagency organizationinformationand governanceBOCC has emergencypowers
Next StepsDHHSCSFNCGA Report to NCGA related to Stage One/regionalsupervision transmitted February 27 Final report expected soon May consider legislative change this session based onrecommendations from DHHS, CSF and/or SSWG
CONSOLIDATED HUMANSERVICES
PossibilitiesOrganization and governance More counties making changes Some counties undoing changesLegislative changes? Technical changes?Try to facilitate information sharing in CHSAs?Regional consolidated human services agencies?Changing role of local officials (per SSWG recommendations)?Human resources changes?
Public HealthPUBLIC HEALTH
Public HealthMedicaid transformation New administrative procedures Effects on local revenues uncertainContinued changes to local agency/governance approaches Consolidation or de-consolidationCross-county voluntary collaborations Example: NC Public Health HIPAA Alliance
Public HealthClinical services: keep or divest? Expect this to vary based on local needs Local partnership development: community healthcenters, hospitalsEmerging issues in population health Social determinants of health Infrastructure and health Controlling communicable disease in an era of vaccinehesitancy
Contact UsMark Bottsbotts@sog.unc.edu919.962.8204Patrice Roeslerproesler@sog.unc.edu919.843.4167Jill Mooremoore@sog.unc.edu919.966.4442Aimee Wallwall@sog.unc.edu919.843.4957
Role: "protect and promote the public health" 13 Powers and duties: Appoint the local health director Make policy for local public health agency Adopt local public health rules Adjudicate disputes regarding local rules or locally imposed public health administrative penalties (fines) Impose local public health fees Satisfy state accreditation requirements for BOHs