Transcription
Philippines Final ReportOctober 1997–June 2007USAID’s Implementing AIDS Prevention and Care (IMPACT) Project
Final Reportfor theImplementing AIDS Preventionand Care (IMPACT) Project inthe PhilippinesOctober 1997 to June 2007
The Philippines Final ReportSubmitted to USAIDBy Family Health InternationalJune 2007Family Health International2101 Wilson Boulevard, Suite 700Arlington, VA 22201TEL 703-516-9779FAX 703-516-9781In partnership withInstitute for Tropical MedicineManagement Sciences for HealthPopulation Services InternationalProgram for Appropriate Technology in HealthUniversity of North Carolina at Chapel HillCopyright 2007 Family Health InternationalAll rights reserved. This book may be freely quoted, reproduced or translated, in full or in part, provided the sourceis acknowledged. This publication was funded by USAID’s Implementing AIDS Prevention and Care (IMPACT)Project, which is managed by FHI under Cooperative Agreement HRN-A-00-97-00017-00.
CONTENTSGLOSSARY OF ACRONYMS.ACKNOWLEDGMENTS .EXECUTIVE SUMMARY. 1PROGRAM STRATEGIES, IMPLEMENTATION, AND RESULTS. 3Country Context. 3Geographic and Social Landscape . 3HIV/AIDS in the Philippines . 3National and Local Policy Response to STI/HIV/AIDS. 4Program Strategies and Activities. 4STRENGTHENING STI SYNDROMIC MANAGEMENT . 5Validation and Revision of STI Case Management Guidelines . 5STI Services for MARPs . 6Pilot Syphilis Screening and Treatment Among MARPs in Angeles City. 6Enhanced STI Control in Angeles City and Cebu City . 7Development of Manual of Procedures for SHCs . 9IMPROVING THE SECOND-GENERATION SURVEILLANCE SYSTEM . 10Establishing the National STI Surveillance System . 10Population-based Survey of Male Sexual Behavior . 12National Preassessment of IDU Situation and Response. 12Sexually Transmitted Blood-borne Infection Prevalence among MSM: Qualitative,Behavioral, and Biological Studies. 14Improving National Biological and Behavioral Surveillance and Technical Assistance toIHBSS 2005 . 15Implementation and Management. 17Country Activity Timeline. 20Program Results . 20LESSONS LEARNED AND RECOMMENDATIONS . 24IMPLEMENTING PARTNER ACTIVITY HIGHLIGHTS. 27Implementing and Collaborating Partner List. 27Subproject Highlights . 28ATTACHMENTS . 30Attachment 1:Attachment 2:Attachment 3:Attachment 4:Administrative Order No.5-As 2003, Revised National Sexually Transmitted Infections(STI) Case Management GuidelinesSTI Surveillance System in the PhilippinesSTI Reporting and Feedback FlowSTI Reporting and Feedback Mechanism Summary
GLOSSARY OF TWAVESAcquired immune deficiency syndromeAIDS Surveillance and Education ProjectBrothel-based sex workersCenter for Multidisciplinary Studies on Health and DevelopmentCenter for Health DevelopmentCity health officeDepartment of HealthFemale sex workerFreelance female sex workerField Epidemiology Training Program Alumni Foundation, Inc.Family Health InternationalFHI’s Asia and Pacific DepartmentHuman immunodeficiency virusInjecting drug userImplementing AIDS Prevention and CareJose Fabella Memorial HospitalLocal Enhancement and Development for Health ProjectLocal government unitMost-at-risk populationMale clients of sex workerMale clients of STI clinicManual of proceduresManagement Sciences for HealthMen who have sex with menNational AIDS/STI Prevention and Control ProgramNational Epidemiology CenterNongovernmental organizationNational HIV Sentinel Surveillance SystemProgram for Appropriate Technology in HealthPolymerase chain reactionPhilippine Drug Enforcement AgencyPhilippine National AIDS CouncilPresumptive treatmentRapid assessment studiesRegional Epidemiology and Surveillance UnitRegistered female sex workerReachOut Foundation InternationalRapid plasma reaginRural health unitSTD/AIDS Central Cooperative LaboratorySentinel STI Etiologic Surveillance SystemSocial hygiene clinicJoint United Nations Program on AIDSUniversity of the Philippines-College of Public HealthUniversity of the Philippines-Manila Development FoundationUS Agency for International DevelopmentUniversity of Southern Philippines FoundationVoluntary counseling and testingWo/Men’s Access to Vital Education and Services International, Inc.i
ACKNOWLEDGMENTSFamily Health International would like to thank the US Agency for International Development (USAID),a strong supporter of the Philippine Government’s HIV/AIDS efforts, especially in surveillance andprevention education. USAID’s provision of financial support and guidance to local government andnongovernmental partners during the Implementing AIDS Prevention and Care (IMPACT) projectcontributed to a successful prevention program for the country’s most at risk groups.We would also like to express our gratitude to the agencies involved in the AIDS Surveillance andEducation Project and the Local Enhancement and Development for Health Project, bilateral USAIDprojects implemented concurrently during the life of the IMPACT project: Program for AppropriateTechnology in Health; Management Sciences for Health; Philippine Department of Health agencies(National Epidemiology Center, National AIDS/STI Prevention and Control Program, Jose FabellaMemorial Hospital, and the STD/AIDS Central Cooperative Laboratory); Philippine National AIDSCouncil; De La Salle University; University of the Philippines–College of Public Health; DavaoMemorial Medical Center; city health offices and their social hygiene clinics; and variousnongovernmental organizations. We appreciate working with all of you, and we value our close andeffective collaboration over the course of these projects. By working in close partnership, we were able tocollectively contribute to HIV/STI programming in the Philippines.ii
EXECUTIVE SUMMARYFor almost a decade, the USAID-funded IMPACT Project implemented activities in the Philippinessynergistically with the AIDS Surveillance and Education Project (ASEP) and eventually with the LocalEnhancement and Development for Health Project (LEAD), both funded by USAID.IMPACT/Philippines’ goals were to improve the management of STIs and HIV/AIDS by increasing theavailability, quality, and demand for STI services and to strengthen surveillance to generate quality datato reliably monitor HIV/STI prevalence and trends, program outcome, and impact. With a budget of aboutUS 2.1 million, the following activities to strengthen STI management and improve second-generationHIV surveillance were completed by IMPACT/Philippines: a study to validate and update the National STI Case Management Guidelines pilot syphilis screening and treatment among most-at-risk populations (MARPs) in Angeles City enhanced STI control in Angeles City and Cebu City establishment of a national STI surveillance system, includingo strengthening of existing STI reporting mechanism from social health clinics (SHCs)o establishment of syndromic sentinel site reportingo development of a system of periodic surveys to complement STI universal reporting and syndromicsite reporting population-based survey of male sexual behavior national preassessment of the injecting drug user (IDU) situation and response; sexually transmitted and blood-borne infection prevalence assessment among men who have sex withmen (MSM) qualitative and bio-behavioral surveys improvement of the national HIV biological and behavioral surveillance, including identification ofspecific groups of men at high risk for HIV as one of the sentinel surveillance groups, and technicalassistance for the implementation and analysis of the 2005 Integrated HIV Behavioral and SerologicSurveillance System (IHBSS).Among the various donor-assisted projects, IMPACT/Philippines was by far the staunchest partner of theNational AIDS/STI Prevention and Control Program–Department of Health (NASPCP-DOH) in the areaof STI programming. The evaluations, operations research, training, and other related activities that theproject implemented resulted to revisions in national STI guidelines; generation of reliable data fordecision-making; crafting of evidence-based interventions; reduction in the prevalence of the morecommon STIs among MARPs and, eventually, the general population; and improvement in the healthdelivery system.IMPACT/Philippines’ collaboration with the Department of Health’s National Epidemiology Center inHIV second-generation surveillance resulted in the current paradigm for STI surveillance, consisting ofuniversal STI reporting, the Sentinel STI Etiologic Surveillance System (SSESS), and periodicpopulation-based surveys. Triangulation of results from these data sources provided stakeholders with aclearer description of the burden of STI in the country.The assessment by IMPACT/Philippines of the decade-old HIV biologic and behavioral surveillancesystem provided the impetus for major innovations to the system—foremost of which was the change insampling methodology. While previous HIV surveillance results are nongeneralizable to the MARPsunder study because of the inherent limitation of convenience sampling, current probability samplingtechniques—in use and recommended by the assessment—allowed such generalizations. Moreimportantly, the new system allowed the DOH and local government units (LGUs) to track HIV1
prevalence and HIV risk behaviors over time. Likewise, the strengthened system enabled programplanners to measure the impact of interventions.IMPACT/Philippines supported the identification of occupational cohorts of men who were frequentclients of sex workers through rapid assessment studies and advocated that they be included in the activesurveillance. This undertaking enabled the DOH to identify potential niches for HIV. Likewise, theproject provided inputs for crafting behavior change interventions directed to the men.Other endeavors supported by IMPACT/Philippines included its attempt to characterize the IDU situationin the Philippines and describe prevailing male sexual behavior and how this may influence the HIVdynamics. The project also supported a hallmark MSM study that debunked the previously held notionthat Filipino MSM found in cruising sites were not really into the practice of anal sex. The latter studyrevealed high prevalence of rectal STI among MSM in cruising sites.Despite the achievements posted by IMPACT/Philippines, there many gaps remain in STI/HIVprogramming that should be addressed so that HIV prevalence does not breach the 1 percent mark amongthe MARPs. The experience from IMPACT showed that sustained STI/HIV/AIDS evidence-basedinterventions, an enabling environment in which behavior change interventions and effective STI servicescan be implemented, and a congenial partnership between donors, government, and nongovernmentalorganizations are paramount to stopping HIV and other STIs dead in their tracks.2
PROGRAM STRATEGIES, IMPLEMENTATION, AND RESULTSIn 1993, the USAID funded the AIDS Surveillance and Education Project (ASEP),which aimed tomonitor HIV prevalence and HIV risk behaviors through active biologic and behavioral surveillance aswell as prevent HIV/AIDS increase through prevention education. From April 1997 to September 2003,the Implementing AIDS Prevention and Care (IMPACT) Project supported ASEP in reducing theprevalence of common STIs, improving surveillance efforts, and refining prevention responses toaugment past efforts.Table 1: Country Program FinancialSummary by Year, Philippines.FiscalYearIMPACT Obligation(US 2,125,000IMPACT conducted its activities in close collaborationwith ASEP implementers and complemented the ASEPprogram strategy with a budget of more than US 2million (Table 1). ASEP ended in September 2003.Although the project was able to meet its salientobjectives, gaps were identified in HIV surveillance,education, policy, and advocacy.With the USAID-funded Local Enhancement andDevelopment for Health Project (LEAD) that began in2004, IMPACT was again tasked with filling gaps forHIV/AIDS programming in support of USAID’s Strategic Objective 4 for the Philippines: to increase theuse of improved effective and sustainable responses to reduce HIV transmission and mitigate the impactof the HIV/AIDS pandemic through enhanced quality, availability, and demand for STI management andprevention services, and improved availability of, and capacity to generate and apply, data to monitor andevaluate HIV/AIDS/STI prevalence, trends, and program.Country ContextGeographic and Social LandscapeThe Philippines is composed of more than 7,000 islands with a population of 87 million people (July2005). The United Nations Population Fund situational analysis identified the country’s annual growthrate as one of the highest in the region at 2.4 percent. Reproductive health services are weak, as evidencedby its high maternal mortality rate of 172 deaths per 100,000 live births and that one out of sixpregnancies is unintended and terminated.HIV/AIDS in the PhilippinesThe first known HIV/AIDS fatality in the Philippines was a foreign national who died of AIDS-relatedpneumonia in 1984. Between 1984 and 2006, passive surveillance by DOH’s National EpidemiologyCenter (NEC) recorded 2,719 HIV cases, with sexual transmission as the major route of infection. Theestimated number of HIV cases in the Philippines in 2005 was 11,200.The Joint United Nations Program on AIDS (UNAIDS) categorizes the Philippines as a low HIVprevalence country. HIV rates in all groups under surveillance—registered female sex workers (RFSWs),freelance female sex workers (FLSWs), men who have sex with men (MSM), male sex workers, injectingdrug users (IDUs), and male clients of STI clinics (MSTIs)—have not breached the 1 percent prevalence.The low level of HIV may be due in part to the low number of clients per sex worker, the relatively lownumber of full-time sex workers, the low proportion of injectors among drug users, the presence of socialhygiene clinics (SHCs) for sex workers, and the potential protective contribution of male circumcision.3
However, the low HIV prevalence is not a permanent scenario if the Philippines lets its guard down andbecomes complacent. Current surveillance information revealed 1 percent HIV prevalence and 81 percenthepatitis C prevalence among IDUs in Cebu City. Coupled with high levels of needle sharing andunprotected sexual partnerships, this is a potential route for further HIV transmission.HIV transmission knowledge, which is less than 55 percent in all monitored risk groups, falls well belowset DOH targets. Consistent condom use remains low in almost all populations and cities surveyed (lessthan 57 percent in many cities), and risk perception for HIV transmission revolves around drug injectionand multiple sex partners, not unprotected sex. The high prevalence of STIs, a known cofactor for HIVtransmission, amplifies the risk for the spread of HIV. Direct outreach information and services aresporadic for many cities and populations. Although some outreach interventions are available, no cityoffers a full package of HIV prevention outreach services. Access to voluntary counseling and testing(VCT) services remains low.National and Local Policy Response to STI/HIV/AIDSThe Philippine Government responded aggressively to the HIV/AIDS threat and adopted a dual strategyof surveillance and prevention education. The DOH classified HIV/AIDS as a notifiable disease in 1986and established the National HIV/AIDS Sentinel Surveillance System (NHSSS) in 1993.The Philippine National AIDS Council (PNAC) created in 1992, is a coordinating body composed of 26public and private organizations. One of its most significant accomplishments was the enactment of ThePhilippine AIDS Prevention and Control Act of 1998 (Republic Act 8504). The law integrated HIV/AIDSeducation and services into a variety of government departments—Education, Culture and Sports, Health,Interior and Local Government, Labor and Employment, Tourism, Social Welfare and Development,Foreign Affairs, National Economic Development, and Justice.Program Strategies and ActivitiesIn keeping with the USAID HIV/AIDS strategic plan of keeping HIV infections low, preventinginfections among the most-at-risk populations (MARPs), and integrating sustainable HIV/AIDSinterventions into local government units (LGUs) and nongovernmental organization (NGOs) programs,IMPACT/Philippines set the following goals: Improve the management of STIs and HIV/AIDS by increasing the availability, quality, and demandfor STI services. Strengthen surveillance to generate quality data to reliably monitor HIV/STI prevalence and trends,program outcome, and impact.To strengthen STI syndromic management in the Philippines, IMPACT conducted a study to validate andupdate the National STI Case Management Guidelines. It also supported STI services for MARPs,including pilot syphilis screening and treatment in Angeles City and enhanced STI control in AngelesCity and Cebu City.The following were among major activities undertaken to improve the second-generation HIVsurveillance system: the establishment of a national STI surveillance system that includedo the strengthening of existing STI reporting mechanism from SHCso establishment of syndromic sentinel site reportingo development of a system of periodic surveys to complement STI universal reporting and syndromicsite reporting4
a population-based survey of male sexual behaviora national preassessment of the IDU situation and responsean assessment of sexually transmitted and blood-borne infection prevalence among MSMqualitative and biobehavioral surveysimprovement of the national HIV biological and behavioral surveillance, including identification ofspecific groups of men at high risk for HIV as one of the sentinel surveillance groups, and technicalassistance for the implementation and analysis of the 2005 Integrated HIV Behavioral and SerologicSurveillance (IHBSS).IMPACT produced publications and materials that were circulated to partners and became usefulreference sources (Table 2).Table 2: IMPACT Publications, Philippines.TitleMale Sexual Risk Behavior and HIV/AIDS: A Survey in Three Philippine CitiesEnhanced STI Control in Angeles City, PhilippinesManual of Procedures for Social Hygiene ClinicsSSESS Manual of OperationsSexually Transmitted and Blood-Borne Infection Prevalence Assessment in a High RiskPopulation: MSM the PhilippinesQuantity500200200150150Strengthening STI Syndromic ManagementValidation and Revision of STI Case Management GuidelinesPoor accessibility, acceptability, and availability of services, as well as the rampant use of ineffectivedrugs, defined STI management in the Philippines. To address this, the DOH included STI services in thehealth delivery system and promoted STI syndromic case management. To ensure integration of STIservices and adoption of correct guidelines for STI management, IMPACT/Philippines, with technicalassistance from the Program for Appropriate Technology in Health (PATH)-Philippines, assisted theDOH in evaluating the existing STI syndromic case management guidelines and the risk assessment tools.IMPACT/Philippines conducted a study in 1998 to determine the validity of the flowchart for vaginal discharge determine the etiologic agents causing vaginal discharge in women and urethral discharge in men assess the validity of the current STI diagnosis and management practices in the study clinics inrelation to gold-standard etiologic diagnosis improve diagnostic validity of vaginal and urethral discharges and revise national STI casemanagement based on the study resultsIMPACT/Philippines collaborated with the DOH, the University of the Philippines-Manila DevelopmentFoundation (UPMDF), the University of the Philippines-College of Public Health (UP-CPH), JoseFabella Memorial Hospital, Davao Memorial Medical Center, PATH, STD/AIDS Central CooperativeLaboratory (SACCL), and the LGUs in the study sites. The two-phase cross-sectional study comparedsyndromic diagnosis with gold-standard etiologic diagnosis and was completed in 2002. A total of 2,000women with vaginal discharge and 200 men with urethral discharge participated in the study. In the firstphase, the researchers identified various behavioral, clinical, and laboratory factors associated with5
chlamydia and gonococcal infections. These factors were used to modify the flowchart for cervical andvaginal infections diagnosis.The second phase validated the diagnostic performance of the modified flowchart for the diagnosis ofcervical and vaginal infections. The flowchart that was developed had moderate sensitivity (79 percent)and low specificity (30 percent). Investigators thus constructed alternative flowcharts and tested them bycomputer simulation to analyze sensitivity, specificity, and positive predictive values. The cost analysesof the various flowcharts were also determined.The diagnostic validity and cost analysis of these flowcharts were presented to a technical advisory group.A flowchart with a reasonable sensitivity, specificity, positive predictive value, cost effectiveness balance,and feasibility to implement in the Filipino setting was selected as the recommended national STI casemanagement guideline for vaginal and cervical discharge. A dissemination forum was held during whichIMPACT/Philippines presented the findings of the study.FHI assisted the NASPCP in drafting an administrative order to revise the current national STI casemanagement guidelines. In January 2003, the DOH secretary of health signed administrative order No.5As 2003 entitled, Revised National Sexually Transmitted Infections (STI) Case Management Guidelines.Attachment 1 is the full text of the administrative order, without the flowcharts. IMPACT likewiseassisted PNAC to develop the national guidelines on STI diagnosis and management for female sexworkers (FSWs), MSM, and transgendered individuals. The guidelines have been used for STImanagement all over the country. IMPACT organized workshops for health workers to disseminate thenew guidelines.STI Services for MARPsHIV surveillance revealed low HIV but high syphilis rates among certain MARPs in some sites likeAngeles City. This was mainly due to the inability to treat cases because of poor FSW coverage in SHCs,the absence or irregular supply of STI drugs, lack of emphasis on partner notification and treatment, andlow condom use. Likewise, the MARPs refused to avail of STI services because of stigmatization,perceived poor quality of SHC services, and fear of being identified. To improve the access to and qualityof STI services, IMPACT/Philippines implemented the pilot syphilis screening and treatment amongMARPs in Angeles City and the enhanced STI control in Angeles City and Cebu City.Pilot Syphilis Screening and Treatment Among MARPs in Angeles CityGiven the high syphilis prevalence among certain MARPs, its tendency to be asymptomatic and theavailability of a cost-effective screening test, IMPACT/Philippines worked with ReachOut FoundationInternational (ROFI) and the Angeles City Government to develop a clinic-based and outreach model for effective screening, diagnosis, and treatment of syphilis improve the screening, treatment, and counseling skills of healthcare providers increase the number of MARPs screened and treated for syphilis increase the number of clients and partners properly counseled in preventing reinfection increase the number of partners notified and treated through intensive counseling develop a mechanism for government and NGO collaboration examine the effectiveness and impact of the intervention and the feasibility of replication promote the allocation of resources to sustain the activity after the initial intensive phase of syphilisscreening and treatmentAn enhanced syphilis screening and treatment study was conducted in Angeles City to address the issueof high syphilis rates among MARPs. This included on-site and clinic-based syphilis screening andtreatment.6
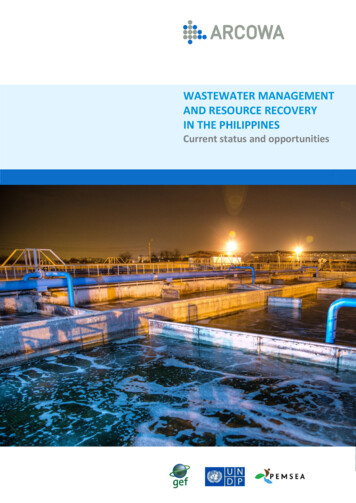
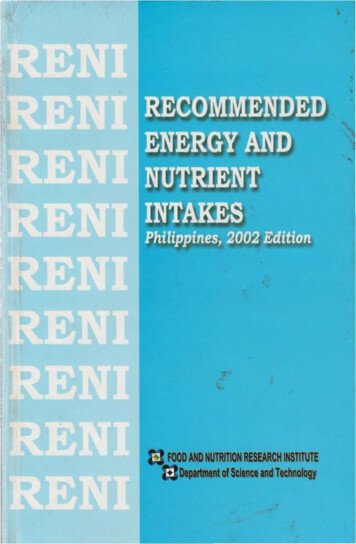
A total of 2,445 MARPs were screened; 5 percent were reactive and treated for syphilis (Figure 1).Pockets of active syphilis were found among FLSWs who did not have access to STI services or HIV/STIprevention activities.Figure 1: Percent Reactive and Treated for Syphilis Among MARPs, Angeles City, 1999.20% Reactive% Treated15105PartnersMSTDMCSWMSMFLSWRFSW0Not all reactive cases were treated with at least one dose of 2.5M unit of benzathine penicillin. Only 60percent of male clients of sex workers (MCSWs) were treated for syphilis. This was done either on-site orduring a follow up visit in the clinic. Of those treated, 8 percent received treatment on the same day and53 percent during follow-up visits. The 40 percent of cases who were not treated were mostly cases whoseblood samples were taken in the field and tested in the clinic. The majority of these cases failed to showup for their test results. Other failure to treat was due to clients being unable to wait for the test results.The syphilis screening and treatment, in conjunction with outreach education activities and incollaboration with NGOs and the government, was an effective way to reach people most vulnerable toHIV with asymptomatic syphilis.Enhanced STI Control in Angeles City and Cebu CityAfter both the pilot syphilis screening and treatment and the prevalence study among MARPs in AngelesCity, IMPACT/Philippines proposed an operations research for expanded and enhanced STI treatment toattain a rapid decrease of gonorrhea and chlamydia infection in the cities of Angeles and Cebu using the“STI Control Nexus” model as framework. The general objective of this operations research was to builda model for enhanced STI control through combined government- and NGO-delivered STI interventionsto provide an effective STI management package for FSWs. Specifically, the activity aimed to: reduce levels of common curable STIs by providing a round of presumptive treatment (PT) to womenat high risk maintain low prevalence of common curable STIs by strengthening preventive and curative services determine the prevalence of gonorrhea and chlamydia among FSWs and MCSWs prior to PT, onemonth, and six-to-twelve months later monitor STI rates in local health facilities during this period through records reviewThe government SHCs took charge of diagnosis and treatment, while health education, counseling,behavior change communication, and condom promotion and distribution were carried out by partnerNGOs. The operations research also included the provision of a single round of PT for FSWs to reducegonorrhea and chlamydia infection rates. In greater detail, the activities included the following:7
Reinforcement of routine screening of RFSWs using standardized clinical guidelines for STI screeningand management. Training on the use of clinical guidelines was provided to healthcare providers at theSHC. The SACCL provided training to strengthen the laboratory capacity of the clinic. Collaboration with PATH’s existing outreach and peer education efforts to improve access of FLSWsto preventive and curative services. Promotion of 100 percent condom use in commercial sex encounters. Improvement of access to effective STI treatment for symptomatic men through strengthening servicesof private-sector doctors and pharmacies. Private practitioners and pharmacists received trainingconducted by PATH and FHI on STI case management. Provision of a single round of PT to FSWs and their clients to rapidly reduce gonorrhea and ch
SACCL STD/AIDS Central Cooperative Laboratory : . System : SHC Social hygiene clinic : UNAIDS Joint United Nations Program on AIDS : UP-CPH University of the Philippines-College of Public Health : UPMDF University of the Philippines-Manila Development Foundation . rate as one of the highest in the region at 2.4 percent. Reproductive health .