Transcription
How WellMed Reduced Health Care Costsin the Rio Grande Valley of TexasPresented by:Carlos O. Hernandez, MDPresident, WellMed Medical Group, P.A.
OverviewRio Grande Valley health care costsWho is WellMed?WellMed’s business modelWhat drove health care cost in the RioGrande Valley?WellMed’s strategies for successDid our strategies work?Next steps2WellMed Medical Management Internal use only. Donot copy or distribute without written permission
Rio Grande Valley Health CareCosts - Then and Now“ I’ve come to think that a major reason for thechange may be a collection of primary-care doctorswho don’t even seem to recognize the impact ofwhat they’ve been doing.”-Atul Gawunde3
WellMed Mission and VisionOur goal is to provide betterpreventive healthcare to seniorsthrough a proven measurable andresults-driven healthcare deliverysystem.Mission: To help the sick become well and to helppatients understand and control their health in alifelong effort at wellness.Vision: To change the face of healthcare deliveryfor seniors by providing quality, proactive patientcare with a focus on prevention.¾y4WellMed Medical Management Internal use only. Donot copy or distribute without written permission
The WellMed DifferenceDr. George M. Rapier III founded WellMed in 1990as a single clinic in the San Antonio Medical CenterGuiding principle was to focus on the PCP-patientrelationship – PCPs working to comprehensivelycare for our patients’ health care needs andbreaking down barriers to our patients’ healthissuesOver the years, WellMed grew into a diversifiedhealthcare company with clinics, medicalmanagement, utilization management,transportation services, and an award winningDisease Management program5WellMed Medical Management Internal use only. Donot copy or distribute without written permission
WellMed at a Glance6WellMed Medical Management Internal use only. Donot copy or distribute without written permission
What We AreWellMed is a healthcare delivery system serving seniors ina primary care-centered environment through acomprehensive network of contracted and employedphysicians and multiple Medicare Advantage Health Plans.7WellMed Medical Management Inc.MSOWellMed Medical Group PAOrganizationPhysicianWellMed Network Inc.501aRisk-bearingWellMed Medical Management Internal use only. Donot copy or distribute without written permission
The WellMed Business ModelWe believe the highest qualitymedical care yields lowest costs byremoving healthcare expenses fromthe system over time.Mutually BeneficialRelationships withPCPsHigh Quality MedicalCare Focusing onaccess, carecoordination and caredelivery resulting inlower health costsShifts away fromtraditional acute andepisodic care to achronic care deliverymodel8WellMed Medical Management Internal use only. Donot copy or distribute without written permission
The Rio Grande Valley (RGV) ofTexas - Six Years AgoDr. Atul Gawande – “The Cost Conundrum”, TheNew Yorker, June 2009Cost of Care in McAllen, Texas compared to ElPaso, TexasMedicare spent 15K per enrollee in 2006 -2Xnational averageEl Paso County (800 miles from McAllen) - Generallysame demographics half the per-capita Medicarecosts and the same or better resultsUtilizationMedicare Patients in McAllen received 2-3Xpacemakers, CABG’s, stentsHome health was 5X El Paso costs9WellMed Medical Management Internal use only. Donot copy or distribute without written permission
The Rio Grande Valley (RGV) ofTexas - Six Years AgoUtilization compared to El PasoAlmost 50% more specialist visits for critically illMedicare patients2/3 more likely to see 10 specialists in a 6 month periodMedicare Patients in McAllen received20% more abdominal ultrasounds200% nerve-conduction studies to diagnose carpaltunnel syndrome2-3X pacemakers, CABG’s, stentsHome health was 5X El Paso costs10WellMed Medical Management Internal use only. Donot copy or distribute without written permission
Misaligned Incentives Drove CostsDoctors were rewarded in a Fee forService model so the focus was onQUANTITY of care deliveredSome doctors owned a stake in hospitals,home health agencies, imaging centers,and other designated health servicesDoctors incented to over-utilize and overtreat patients with minimal perceivedthreat of penalties for this behavior11WellMed Medical Management Internal use only. Donot copy or distribute without written permission
WellMed entered the RGV in 2009WellMed entered the market in a valuebased payment model (an alternative to feefor-service)WellMed partnered with select health plansto accept full-risk capitation payments forsenior and dual-eligible patientsWellMed Networks, Inc. contracted withvarious specialists, home health andhospitals in the regionAcquired the first clinic in the RGV in 200912WellMed Medical Management Internal use only. Donot copy or distribute without written permission
Medicare Population RGVThree Select CountiesState Name County 3.91%148,72152,75735.47%WillacyJan 2015TotalWellMed Medical Management Internal use only. Donot copy or distribute without written permission
Key Strategies to WellMed’sSuccess Care Management/Care Coordination Quality Risk Adjustment Growth Provider and Patient Engagement Systems approach to care14WellMed Medical Management Internal use only. Donot copy or distribute without written permission
What is Care Management?15WellMed Medical Management Internal use only. Donot copy or distribute without written permission
Disease Management ProgramsDelegated Patients who have one of the followingchronic conditions are eligible to enroll inthe Disease Management Programs16WellMed Medical Management Internal use only. Donot copy or distribute without written permission
Care Coordination Team17
Advanced Care Management Program
Advanced Care ManagementProgram Care Management for High Risk/ComplexPatients- top 3-5% of high risk population(Home Based Care/Palliative Care) Telephonic & Face to Face Assessment &Monitoring Transitions Program Clinic Based Patient Care Conferences(PCC)19WellMed Medical Management Internal use only. Donot copy or distribute without written permission
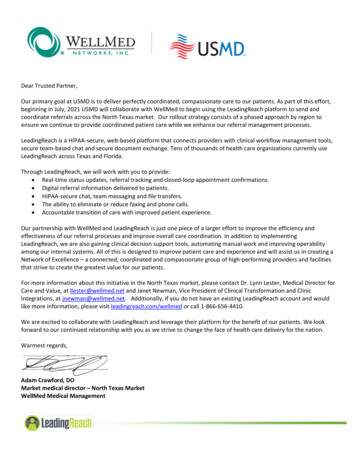
Illness Pyramid – The Rosetta StonePercent ofPopulation78% ofadmissionswere formembers inbands 1 and 2Advanced/ CriticalIllnessBAND 120Source:CareFirst HealthCare Analytics – 2012 DataPercent ofCostPMPMCostIllnessBurdenRange
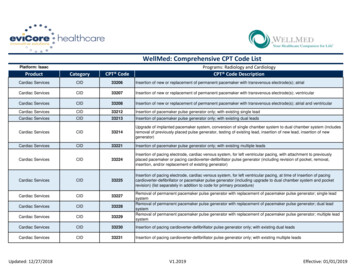
Population Stratification BandsClinic Based Care TeamBAND 1 Health & Wellness Preventive Screening Annual Care VisitsBANDBAND 22ClinicBasedClinic Based TeamTeam andand CareCareManagementManagementDisease ManagementPrograms SNP members Controlled/Stable CHF Controlled/StableCOPD/Asthma Controlled/Stable Diabetes Controlled/Stable IHD/HTNUtilization Management Observation Admissions Elective Admissions ER VisitAtAt RiskRiskBANDBAND 33AdvanceAdvance IllnessIllnessBANDBAND 55 Transplants (evaluation stage through transplant) Co-occurring Medical and Mental Conditionssuch as Bipolar disorder, schizophrenia andmajor depression (mental health dx plus any oneof the 4 chronic disease states (DM, IHD, CHF,COPD, PVD) ESRD -fistula High Cost Injectables HIV 85 & lives alone Cancer- active chemo treatment (Round 3 ) Other conditions or situations deemed by PCP 1 unplanned admission in 6 months Frequent falls greater than 2 in a 3 month period Homebound Hospice appropriate –not willing toenroll Life limiting illness with possible lifeexpectancy 12-24 months Requires Symptom Management Metastatic Malignancy CHF stages IV-V End stage COPD, CirrhosisHighHigh RiskRiskBANDBAND 44 2 admissions in last 6 months S/P MI within 60 days AIDS CHF stage III ESRD- temporary catheter Hospice graduates Cancer- active chemo treatment (Rounds 1 &2) Change in Functional Status (Amputation , CVA) Poly-Pharmacy and poor compliance ( 8 prescription meds) Home Health greater than 2 months Multiple ER visits within 3-6 months Moderate to severe dementia Requires short term case management assistance Oxygen Dependent S/P transplant to 1yr after transplant Hip fracture age 75
Care Management Across AllSettings22WellMed Medical Management Internal use only. Donot copy or distribute without written permission
Transitions Program
Transitions Program Goals DecreaseReadmissions/ER Visits Facilitate Safe Transitionto Home Coordination of Services(medicationreconciliation, teamcommunication, andclose follow up) Meet SNP Requirements(Special Needs Plan) andHEDIS quality goals24WellMed Medical Management Internal use only. Donot copy or distribute without written permission
Clinic-based Population ManagementPatient Care Coordination Meetings Weekly Meeting withHealth Care Team Review InpatientTransitions and ER visits Review Complex CareCases/risk stratificationof population Develop/Revise Plan ofCare Opportunity for processimprovement25WellMed Medical Management Internal use only. Donot copy or distribute without written permission
Provider Engagement Intrinsic rewards– Autonomy, mastery,purpose, tradition Extrinsic rewards– Incentives– Comparative reporting– Personal development26WellMed Medical Management Internal use only. Donot copy or distribute without written permission
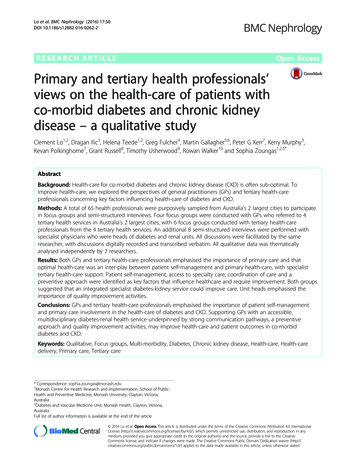
Did it work?Rio Grande Valley – Historic Utilization MetricsDates of Service: Jan 2009 - March 201527WellMed Medical Management Internal use only. Donot copy or distribute without written permission
Did it work?Rio Grande Valley – Historic Utilization Metrics RAF AdjustedDates of Service: Jan 2009 - March 2015-Risk adjusted28WellMed Medical Management Internal use only. Donot copy or distribute without written permission
29WellMed Medical Management Internal use only. Donot copy or distribute without written permission
30WellMed Medical Management Internal use only. Donot copy or distribute without written permission
31WellMed Medical Management Internal use only. Donot copy or distribute without written permission
32WellMed Medical Management Internal use only. Donot copy or distribute without written permission
Next Steps The work of improving is never done!Specialty compactsVolume steeragePatient engagementPatient portalTechnology33WellMed Medical Management Internal use only. Donot copy or distribute without written permission
Engaging the Physiciansand Healthcare TeamIncentives based on:Health care costsQualityOutcomesRisk adjustment coding accuracyPatient satisfactionMembership/MA panel sizeProvider behavior/core values34WellMed Medical Management Internal use only. Donot copy or distribute without written permission
Physician IncentivesQ4 HCCPMPM %HCC PMPMQtrly Pool Base RELATIVETO PAYOUT Q4 HCC PMPMLine QualityFOCUS ONCARE %RELATIVETO PAYOUTFOCUS ONCAREHCC %RELATIVETO PAYOUTHCC%MEMBERSHIP SCORE2/201512/2014EVALUATIO Proposed BonusN SCORES With 47.5549,077.73 54,077.7354,236.11 43,787.91 11,294.93 36,678.52 3692.09%345.3699.85%1,123.301.001.004,043.32 11,229.17 9,197.02 65,465.28 58,274.7635QUALITY %Q4 Final HCC RELATIVEPayoutTO PAYOUT9,747.02 8,780.68 2,766.45 8,594.54 30,283.23 63,824.76 52,568.59 14,061.38 45,273.05 184,548.22WellMed Medical Management Internal use only. Donot copy or distribute without written permission
36WellMed Medical Management Internal use only. Donot copy or distribute without written permission
Success - Three KeysPatient StratificationTransitions ProgramAccess to Care37WellMed Medical Management Internal use only. Donot copy or distribute without written permission
SummaryRio Grande Valley health care costs then & nowWellMed’s business modelHealth care cost in the Rio Grande Valley drivenby misaligned incentivesWellMed’s strategies for successOur systems approach to care drove costs downWellMed is not done yet .still striving toimprove care to our patients while driving costdown where appropriate38WellMed Medical Management Internal use only. Donot copy or distribute without written permission
Questions?39WellMed Medical Management Internal use only. Donot copy or distribute without written permission
ReferencesGawande, A. (2009, June 1). The Cost Conundrum - The New 1/the-costconundrumGawande, A. (2009, June 23). The Cost Conundrum Redux - TheNew Yorker. e-the-cost-conundrum-reduxGawande, A. (2015, May 11). America's Epidemic of UnnecessaryCare. illatul-gawande40WellMed Medical Management Internal use only. Donot copy or distribute without written permission
WellMed entered the RGV in 2009 WellMed entered the market in a value- based payment model (an alternative to fee- for-service) WellMed partnered with select health plans to accept full-risk capitation payments for senior and dual-eligible patients WellMed Networks, Inc. contracted with various specialists, home health and hospitals in the region