Transcription
HAWAI IMEDICALJOURNALApril 2003Volume 62. No 4!SSN 0017-8594.I.a
ii/22Intr(-to prepare theaccording to yourto repair the stratum corrto avoid the sun s.Recommendwww c taphil.comGALD(The first and last wc‘‘‘p
HAWAIIMEDICALJOURNALContentsloditorial: All Physicians Have I)ouble LivesCoO/stein Ml)(USPS 237-640)72.\oi’iiti litPublished monthly hr theHasu an Medica.i Assoctationlicorporeted in S56 under the Ninirelis101 South Beretauj. Suite(1Hr dulu. [Lusait ms 1—1-Ph ne ‘101 CeO-iC: Eju ytb 5.7Prohiem Based learning and Medical IIalpractice: i)oes How YoueBeen Trained Niake A Difference?Do/i h-t/iii e JD. kioreti Lull. Rtehord Set cult, .11.8,11 111)/ It J’ / IISDJ I ILEditors—Resideiits Case Series: A 76 Year-Old 1an with Anemia.\rnian Goldstein MD.\sociatc Editor: William 5k. Goodhuc Jr. Ml)Sews Editor: Deer;- \:\1DContributing Editor: Russell 1. Stodd MI)Editorial BoardJiiltn Breinich Ni i S. Saturn isutsit PhD.5 G Massey NID. Mr roil L Shirasu MD.DouglaErank I Tahrth MD. Alfred I). Morris MDLymphadenopath and Pericarditis.F iiumt-I ncr/tool tot MD. iOtro,t I-Ei:it4 :111). toil‘cOre/dill)Si)Medical School Hotline: The Role of \ iolence Prevention Educationat the L niversit of hawaii John A. Burns School of Medicine iL [l-JABSO7sIii/im it P.S. (Lc m’l’cr, .1-Il)1-Journal StaffEditorial Aui;tant: Drake (hinenOfficersPresident: Cals-in Skong Ni BPre;ident-Elect: Sherrel Hammer Ml)Secretary-: fhittaau Kosasa MI)Treasurer: Paul DeMare MDPast President: Gerald McKenna Ml)(‘ancer Research Center Hotline: Childhood Cancer.Rapid Changes in the Last 40 \‘earsRol,ei’t U . U i/hit , it lii)84News and Notesllcitrv N. lokovsimo Ml)87Classified Notices89WeathervaneT ,Stotla Sell)90County PresidentsHawaii: Jo—Amt Saruhi MI)Honolulu: inant Cr Rahman Ml)Maui: Joseph Karnaka Mi)West Hawaii: Mi Bairos MDKauai: Gardner Quarton MDAdvertisrng RepresentatiseRoth Communications 2O4OAlewa .DriveHonolulu, Hawaii 96817Phone (80K) 595-4124Fax. (808) 595-5087I1tJ?usmc//I‘0iiiiNlitiS)IIS5I’(‘as cv art by Dietrich Varez, \olcano. Hass aureserved hr the artist.Al riehtsPele c Dream of LohiauPiule. taiddecs sit the volcano dreami al her loserwhile sieeptflg n a lava cave,71
cause of the suit sensitivity i it red tattoos and published ow studiesin the Artnals at Internal ,\ledrcrne, .1. Russell Elkrni,rtrrn, M.D. theEdiior, said. Adoldstein has sol ed the Case of the itching Tattoowith a deftness that woukl do honor to the Master Sleuth of BakerStreet (himselfa strtdent and connoisseur of tattoos) and that would(as usual) bring amazement to the admirine Dr. Watson and consternation to inspector Lestrade.”1-artunateim. most PtF’Stciali-s\ r:terv haS e not nad to go cup theirday ohs.” and Hec’nan discusses manm of them. Hcenan sass thataccardit’tg to same survey” di)’? I-Ohm’scIrtrrs sso aId do onret.hinelse if them’ could. rEd: und”ubtedim, moat because of I-RiO s.HII’PA, etc.). Physicians are not alone in some dissatislaction iflthe.ir chosen prot’k.ssion. According to attorney and author John.Graham (The Farm most it v ems vs on II r ither ha doing something else,”lii our t’OiCsN1Ofl. the cc’ninlotrai its heiss ccii rnedcttte and lueralure nov’. hecon’titte’ “institutionalized.” ‘-I of medical schoolsortered literature classes to I huh and 39i ree. uired thetisI s as vein pleased to receis e an announcement about tire ThirdAnnual National Medical Fiction Writers Competition for Physician.s sponsored by SEAK Inc., a medi.cal publish .ng, ertnpar.y.Please don’t give up yo’ur scalpel and steth.oscope. Y’ou cast havemore than one lile.EditorialNorman Goldstein MDEditor, Hawaii Medical JournalAll Physicians Have Double LivesPCcmnslasto wetr ulmi’ than OitC flat at the SItticIlfli.healers. twtcherc. and re archcr. ae areInto our nJchusbands/wives, parents and c.liildre.n, a.[l at once.But tt.ere are some p.hysic.i.ans who truly lead double. lives not asclandestine CIA or FBI agents, but as very speci.al people. Some arevet’y well-known it. th media and some are not so well-knownhj 1si r,,h proiLnarm D Sa nuj \\ r, Dtw ‘or o’ I,t,SsH i KPttHt,F—Iaaa.ii rrphthahioertAuthor N lichaei Crichton Fire Andromeda Strain a also aHarvard Medical School graduate. Other non-practicing phr Nicranwriters i.tic iDe Robin Cook (Coma,). Ethan Canin (Carry’ Me Acrossthe Water), Deepak. Chopra (The. Seven Spiritual Laws of Success’),a.nd Spencer J )hnson (\Vho Moved My Cheese?).In reading Double [ft cv by David Heenan, a trustee of the mutesCampbell Estate and former Vice President for Academic A (Firsand Dean at the Lois ervite nt I lao mu) Busroess School. I sascaptivated hr the bh retaphics of 1/ac) noting people sv ho has e ledmore than ‘rue I ti/a A tier 22 years 5? astronauts and 36 ‘maitned”missions, an American suoman was tn space on June 18. 1983. SallyRide, the nation’s first woman astronaut, then found life afterNASA, She helped in training scientific national security and inarms control affairs: accepted a position as Professor of Ph sics atL. (1 Suit Dieo. and des eloped “Kid Sat.” a kids’ satelltte prouram.and she helps girls and : ounu wotueti become interested in scienceand math. Sally Ride’s ads icc’, ‘‘Nces cr Stop Learning.’’‘FesN Gerriten. \l . [)., is also a s’arm succestul author, tirstromance novels, Her hooks include Harvey’, vs hich made tire NYTimes best seller list in 1996, [ilk Support (1997 , Bloodstream(1998), and The Surgeon (2001). Tess Gerritsen’s advice, “writeabout what you know”Other hiocraphiec 01 cream e souls with double live” tnclude\orio Oha, Chairman ot the Board of Sons’. opera singer.nony conductor, and jet Hot. Ohga cines it all hr proerauu’ningJsAloha Laboratories, Inc.When results countCAP accredited laboratoryspecializing in AnatomicPathologyQuality and Sen iceTwo of the biographies are I’amniliar names to the art ssorld,e.specially in Hawaii, Rrm. K’ent and Chuck Watson, Kent, a a Flknown s’tock.hroker, (Fund his artistic talent in turned wood bowlswhile Wars on, former Chairman of H’awaiian Dred i.ng and Construction C an panv. later to leave Di lii ugham Corporation. l/,’rcedholerN, ü earcanc rollers earl restored trartr’rs non culpruretearing ,tli over Han ,ut end the Pacrfic.I)Hao’0Iueeestion n “Crafting vol [lid. ui Work andoffers arcedi’assi.on for Untold Success.” H.is last chapter otTers 20 key’s to adouble life.Hrstortcally, perhaps the best known literar’ physicians wereAnton Chekhov and Sir ArthurConan Fovle, When I d.iscovercd theDavid M. Amberger. MDi.aborator DirectoryPhone: SOS 842-6600Fax: (84)8) 848-0663“,,-I’ftiIaii: results@aIohalabscomhttp :I/ww ‘.aiohaIabs.com72
Problem Based Learning and MedicalMalpractice: Does How You’ve BeenTrained Make a Difference?David Behiing JD, Kristen Low, Richard Sevehno MS, David W. Boldt MS, and John Hardman MDPresentlareported h the Civil Trial \etsvork, the rate of medicalmalpractice cases land other persomil injur’ turN tiled in this.countra has increased 2tY in the i I) years he tween I 9Sb— I a94.Furthermore, there is no indication that this ti-end is slacking off, Asresult vera inree economic cost 5 imposed utron the medicalmalpractice liability iitsurance industra and the pha sicians theyrepresent. Ultimately the patients hear the burden of a physician’sincreased cost of doing business by paying higher medical fees,Societal and public health costs associated with medial malpractice claims in the U,S, are also significant. It has been argued thatthe prolific nature of malpractice claims ss eaken the nature of thest 0thi iph Km m P iticnl P mon hit thmoudethat a patient must constattla he on the lookout for physicians who3are not qualified or do not has e the patients’ best interests in mind.Am’i equal if not ereater social cost of the high levels ot medicalmalpractice claims n this counIr arise lrotn a phvsiemans’ reluctance to t’epui-t possible treattuent errors or sources of errors tbr lOamof a patiemtt suing them. This results in public health specialists’inahilit to properly assess the true amount of physician erroractually present in otir society, As a result dangerous conditionswhich othemn ise could he discovered and corrected h public healthspecialists persist Presentla it is believed that phvs ictan error isresponsible fOr up to i St.i.ilD) deaths a rear.Abstractasaa0 more PBL oPec s, statis0cuP. significant[cr0 groups ‘‘rj be obtainm(iflO5bet- IntroductionCR1 liability for phYsicians’ proh.ssional conduct. commonlyknow n as “ledical Malpractice’’ is a judicial phenomenon withserious social. econontic and pubhc health ramifications, Medicalmalpractice merits, and is presentlr receivins in the current literalure. extensive res iew and investigation. This paper attempt’ tores iesv a small hut potentially important aspect ot medical malpraclice which has not set been addressed in the literature: \\ hetherphs sician trained under a problem based learning ( PBL curriculumhave signific amA different rates of medical malpractice filingsagainst them in comparison with graduates of a traditional lecturebased format. It is hypothesiicd that there is no statisticallysignificant difference between the rates of medical malpracticehetw een PBL and traditional graduates. Thi’ hr pothesic is based onthe tact that PBL cut’rtcuia emphastze strong phr sictan—patientrelationship deveh pment and phr sic’ian-patient c ,nimnutncation.2. Problem Based Learning at the University ofHawaii:Background1. Medical Malpractice:Problem based learning PBL,) is a method of medical educationwhich is largely self-directed by the medical students invols coin theprogram. During t.he first 2. ears of medical training in a PB]’.lOt-ma traditional learning techniques su.ch as lectures an.d formalreading assi enments are Iai’gei.y excluded. The core of the PBL.process alhw s the students to choose their own meadine assignTrvtee ss eekla sinaI I moup meeting’ of 5 orb students in the’presence ut a group tutor tacilitat.e and guide th.e ‘mtemation ofappropriate readinc’ assi nmcnts. At these ‘neetiny’s. mulled “tutuit’iedieairiPs”) the depth of tudent umderstandii’ia iissues assessed sin iii I iath ‘ii ,31’heaith ca’e case prohiem Fhcsccases consist of tictrtous pat:cnt.s and their healt.,h problems eerie rated by fhcuity physicians and sc.i.entific stnf,f, When students aree.x.posed to medical issues that they dO not e.t have a sufficientunderstancli ne of tie.y are ad vised to research these. areas in order todiagnose and treirt that “patient” i,n the upcoming meeting, I mporantla, one ot toe rtrimams toe: in the tutorial. s tine liewith aapproach them Patients. Iron the very limst uturalEconomic, Societal and Public Health Costs of Medical Malpractice:Medical malpractice is a significant legal and societal issue, The,average value ol a j nra serdict I ti a malpractice act i m brought in thek’S. over 5201 .otfi In comp:mrison. the eragc nra verdtcm hrnotIPSb I ,tJ{)t’t. Furthcrni’rc. medical malpractice antouncr tom a taeucrof all tort tu rs’ verdicts uscrune million dollars. Thjs isbnfar the lion’s share of million dollar crdicts heng’ nure than 51create.rthan the next largest tort catecory, products iiahi.iity at i1”f,mnents.n‘5.a,,.‘ssCc usoondence to:Dear; Bewqs.ses’ion.73
“patient centered perspective”. The goal is to instill in the studenta reflex to recognize patients’ potential emotional, social andspiritual problems and concerns. Students are trained to recognizethat patients of different social groups. religious backgrounds orgeographical regions may have very different primary concernseven if the have the same physical problems.Concurrently, PBL students are also required to meet weekly in aclinical setting with community physicians and their patients. During this clinical experience, called “preceptorship”. students aretrained in the taking of history and the performance of physicalexaminations.Additionally, PBL students are required to spend halfaday a weekat a community based medical support organizations such as careprograms for the homeless, hospice. critically ill children, studentbased health organizations. etc. It is the goal of these programs toincrease the clinical and community health exposure of PBL students to accelerate their acclamation and competence in workingwithin and utilizing these environments and resources.As stated above, the purpose of this research is to support thehypothesis that PBL curricula adequately trains physicians to develop equally strong physician-patient relationships when cornpared with traditionally trained physicians. Authors used the ratesof filings of medical malpractice claims against physicians as anobjective assessment of the physician-patient relationship. it is nothypothesized or even suggested that traditional or PBL graduateshave any greater or lesser medical proficiency or knowledge in theactual rendering of diagnoses and treatment to their patients. Itis theopinion of these authors that the instigation of a malpractice actionby a patient against their physician is in most cases not a reflectionon that physician’s ability to render biological treatment. A filing ofa medical malpractice claim is instead, largely an indication of’ afailing in the relationship and communication between that physician and their patient.3 John A Burns School of Medicine (JABSOM):A Unique Opportunity To Compare PBL to Traditional Medical Training.JABSOM is uniquely situated for the comparison of medical malpractice rates between traditionally trained and PBL trained physicians. Between 1975 and 1992 JABSOM followed a traditionallecture based format. However, in 1989. JABSOM adopted a PBLformat and graduated its first PBL trained class in 1993. Additionally. JABSOM s graduates have predominately moved into thefields of primary care (61%- 75% between 1988-2001) (Table I).Because of these facts the authors assert that it is fair to compare theoccurrence of malpractice between the two groups. Thus, in aproximally associated time frame (within 25 yeart) there exist twogroups ot physicians 4raduating m LssLntiall\ thL s imc ticld thatma he compared.A.d.di.tionailv, Hawai.i is a favorah].e. place to assess the rates ofmedical malpractice brought against known physicians. Since 1975the Hawaii law has required that all medical malpractice claimsproceed through the Medical Claims Conciliation Panel (MCCP)before a claim may he filed in court. For strategic reasons(which arebeyond the scope of this project), this MCCP filing requirement hasresulted in many medical malpractice claims being formall instituted (and thus recorded) at the MCCP that would normally have‘been settled by the defendant ordropped by the plaintiff befhre therewas an official record of claim. Thus giving a clearer picture as tothe true numbers of medical malpractice rates than is demonstratedby formal court filings.Research and Design MethodsAs of the writing of this paper JABSOM has graduated 1469physicians since the inception of its four-year program in 1971. Ofthese there have been 1 8 traditionally trained graduating classes and9 PBL graduating classes. The numherofJA BSOM graduates in thetwo groups total 1084 and 489 respectively. However, at the timeof data collection from the MCCP in December of 2000, there wasonly complete data of medical malpractice filings for the years of1974-1999. Thus, the last two JABSOM PBL graduating classes of2000 and 2001 were excluded from statistical analysis, In the finalanalysis the two populations assessed numbered 1084 traditionaland 385 PBL graduates.The rates of malpractice were assessed on the basis of postgraduate year (“PGY”), i.e. first year after graduation, second year aftergraduation, etc. The number of graduates involved in law suits fora given PGY was considered a positive event without any significance given to the number of suits an individual graduate wasinvolved in for a given year. Statistical analysis of the collected databy means of the Continuity Adjusted chi-square and the FishersExact test of the data was then performed.ResultsTable 3 shows the chi-square and Fishers Exact Test values forstatistical analysis of the data collected .As demonstrated in Table3, the population size of the PBL graduates diminishes every PGYby the class size of the graduating class that has not yet reached thatyear of practice.Discussion1. Data:As shown in Table 3, chi-square and Fishers Exact Test analysis failto demonstrate any statistically significant difference in the rate ofmalpractice suit filings for the two study populations. Given therelatively rare event of malpractice filings in a given PGY the PBLpopulation is too small at this time to demonstrate a statisticaldifference.Conclusions and RecommendationsThe data failed to show a statistical difference between the rates ofmedical malpractice filings for traditional vs. PBL graduates. Thisfailure is due primarily to the small size of the PBL population incomparison with the traditional graduates. The problem is compounded by the relatively rare occurrence of malpractice suits on anannual basis in any PGY and the fact that for every PGY thepopulation size of the PBL group decreases. Both of these confounding factors will he overcome with time. The small size anddecreasing nature of the P131, population is a direct result of thenewness of the program and will increase in size and remain stablefor adequate statistical analysis as the program continues andgraduates are added to the population. Furthermore, the rareness ofmalptaLtas. suits in ans gisn PG’ can hi, osi.icorne hs gioupingPGY stogcthi.rina supi.i PG’ group asiththePGY9 inTihlcr.1E[)sDAL. JOURNAL, LOLL LO, APRIL 200274
Now is Ibe limelo cboose TAZOHACFaster, more powerful and as clinically tolerable as Differin cream 01%.31% median reduction at week 4 vs 7% for Differin (P .001)155% median reduction at week 8 vs 25% for Differin (P .001)68% median reduction at week 12 vs 36% for Differin (P .001)1Ak as effective as Dif :rIn cream in inflammatory acne:62% median reduction in papules and pustules at week 12vs 50% with Differin’Ciinica Ny coni arabic tcierabIiiy to Differr cream:Trace levels of burning, dryness, erythema, and peeling withTAZORAC Cream and Differin cream1---TAZORAC Cream is indmted for anne vu oarie The most frequent adverse events reoorted dudno utnea!TZOPC CaCQ 1% f e treatmen arne vu Od’ e e seer r Co SC 3d ’ oauen acoo mcuiei e aescen no order Jesuamat’on Or skm ermn no ourine enact on E e aocjrrmu nit to 50oa vms iv ed urn ma moon 5ac n andALL RCAN
TAZO RAC(lazarotene) Cream! 0.1%SqIEF SUMFt1ARYJ’DIGATIONS AND USAGECDJT A II DICAP 1) NSorPregnaung. Terairigonic Etfrrts PregnaacV Canqnrv XNursing mothers.NiNGSnsr’dacg CciIesrir AirPii1InUsoAI!flflçGoU’;ERSE REACTID’:S‘FADDSAGE,toriirieIsC ILLERGflN—‘i--:,jc—ipsirqrli.FIt;
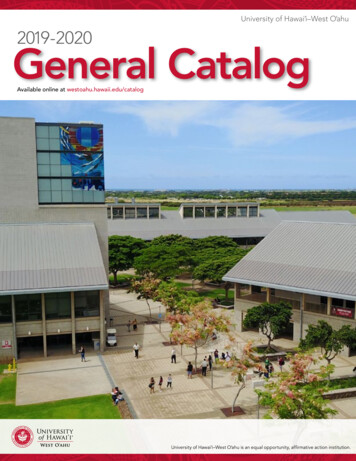
Table 1University of Hawaii JABSOM Residency Matching Summaries. Between 1 9882OOO, 61 75% of JABSOM graduates enteredprimary care fields. The top soecialhes chosen have been Internal Medicine and Family Prachce.*s.ccc-sFac7ii. PracticeFav Prac5ce OosGyri-Famiiy PracticePsychiatryi:1718I-—--ccc-19211l4-.s- IrnS1—.-—.—.II,III-0i Iit77i,j.I‘1((10ott11r
Table 2.Number of UH JABSOM gr duate named in MCCP malpractice claims by post graduate year (PGYI.Ye CPGYass szeGada:orPGYPGY 6PGYPGY 4PGY 3PGY 2IPGY 9-PGY AL. VO78.APV.
TaPe 3.Comeauson: Tractiona is. PBL Graduates notved in MCCP malpracticeTRAPBLIId11it \ ii11[3’tU\lPHI eu’aI;’‘tkh 11010 1’,ttiflfl’,‘1,IIlitOCtIi1,1IidIl\in’ P131t—no3itup11111t 091iia0Iiiino’c’flUsed by over 10,000Physicians in Japanaot‘‘CiltOh11010th*Available in HawaiiSince 1994*Learn From Our ExperienceAt Your OfficeAt Our Seminars.\t Our OfficetulReferences3 in whtc.h there are I 44 posit cc. events, Projected power analy si.demonstrates that once. th.e.re are 18 graduating. c.t.asses t.if PBLtrained physic ans, a 5% difldrence in malprac.tice suit filingsbetween the two populations i.nPGY super grouping wouldmrmstrate a rtatisticallv sicuilicant dilference in the euro ofmalpractice at the 505 ic\ei of erLuui\Iu1eresttnct ulteritnal aui\ isaud cooiparis000! the per-capita01 malpractice I iltnc it ippears thut lucre ma\ currenth he a000-uaitsncall\ ognhticant trend or lower filing rates acatnst P131.grad notes c.ornpared to traditional graduates. Time and. futurest iwtic d in 3 sw u ill tJ it thircnd is si nil i tntiIntroducingCHITIN PRODUCTSs IittiHelping DoctorsHelp Their Patients1Ie uOticd ohntt PHIut aIittotin ittheciiiilii hata\1t’hiitI1itutII toIIi1An r\pproach ToComplementrv Medicine‘ii*Call today for MoreInformation.y%%.12179\Bt)11\ ICenter Street Ste. 22(1Honolulu, HI 968168O8738-O9938O8553 25551’
Mdial elf usion ss oh a small amount ot ascites m the abdomen andpelvis. The t’enal ultrasound revealed calculus in the left kidner withminimal grade I hydronephrosis. There was an 8 mm calculus in theleft ureter at the ui’eteropelx ic junction. -\ bone scan was normal,Bone ma rrosv aspiration md hiopsr re ealed no abnormalitiesI m ph node biopsy revealed scattered secondars toll icu I ar cellswith actis e cerminal centei’ The intert oIl icular tissue ss as coniI vmphr cvres and plasmaposed of a poli ntorphous popu I ati muResidents’ Case SeriesA 76 Year-Old Man with Anemia,Lymphadenopathy and Pericarditis.Paranee Auethavekiat MD, Baron Wong MD,and Jeffrey Fong MDcells, There was background vascular proliferation. Very rarepolvkarr ocytes svere seen, No metastatic tumor. granulomas, oratypical Ir mphoid population.Floss cr tometrrc inmmunophenotvpic mt the is mph node shosvc—ipi’edoni i nant I peripheral T cells and a snial cr popu Lit m ofpotvcltmnal B cell.Case Report76 ear—o1d Chine’e man prcented to hi’ priniar\ eai’e Isicianwjth a two-sear history 01 prosressis e scieht loss ot’SO pounds andfatigue. The pat cut was referred fur psychiatric evaluation, diag—nosed with depression. and started on t’luoxetine. He did not take anyother medication or herbal remedies. F-fe was then seen h\ anotherphysician and found to has c diffuse l\ mphadenopathv on physicalexanilnation. The patient s as then scheduled br a right axillarlymph node hiopss On the da of the procedure. he developed chestdiscomfort, and an ERG showed diffuse ST segment elevationsconsistent with pericarditi’. Echocardiograni s as performed andshowed minimal pericardial effusion and ihuprofen was initiated.The patient then developed epistaxis and an ENT specialist performed a right- sided nasal packinu. The patient was stabilited andunderss cut axillarv lsmph node biopsy. During the procedure hedeveloped recurrent epitaxis and had nasal packing done again. Inthe recovery room, he was noted to he more anemic with decreasein his hemoglobin by 2 grams. He received packed red blood celltransfusion, and it was noted that his blood was difficult to type andcrossmatch.On phr sical examination alter the lr mph node biops the patientwas al ebrile and normoteusi e. Skin examination revealed no malarrash. periuncual telangiectasia. discoid lupus or alopecia areata. Hehad no obvious cutaneous asculitis. synox ins or arthritis. Thepatient had scattered cervical and minimal axiliar lymphadenopa—thy. There were no oral ulcers. Cardiac examination revealed nomurmurs, rubs or gallop, and there was no hepatosplenomegaly.\eui’olo’’ical exantinatton was normal.l)iagnostic data revealed: \VBC of 4. 10(1/ce 4.3(i0— I 0.500/ccwith II’ i h niphoc\ tes and 7’ monoc tes. Hemoglobin was 10.1g/dL t 13—IS g/dL following transfusion with relativelx normalmdtccs Platclet count ss is 3 000/cc (I 31) 000 40(1 000 c F-SRwas 122 mm/hr (0-20 mm/hr). BUN was 16 mg/dL (10-2) )mg/dLand creatinine was 1 .0 mg!dL 0.8- I .2 iug/dfu. Calcium ss as 8,5 mc.’dL . PT and PiT were m ‘rmal. .-\lbumn sva 1 -1 cni/7dl. 0— 1(1,5 my’dl. 0.5—5.5 cm”dl. and globulin sas 6 crn”dI 2.0—3.1 eni’dL.s as I :25(0 ss ith homogenous pattern. ( omplemcni C 3 ss asless than 25 mg/dl (55-120 mg/dL) and C4 was less than It) mg/dL(20-50 mg/dL). Anti —double stranded DNA was positive at titer ofI :20.Anti-Smith!RNP was negative. ANCA ss as negatis e. DirectCoonibs test ss as posuis c. F- rmalysis showed liii) ine-’dl. of’proteinwith no cells. si enty-four-h mr urine protein ss as 46o irie24hr tJ5)) mg;24hu. The tuberculin skm test was negative.A Head CT scan shoss cr1 fusiforin aneurysm of the basilar arter\with noothersignificantahuormalities. Chest, abdominal and pelvicCT scan showed bilateral pleural effucions and a moderate pericarHospital CoursePatient 55 as diagnosed with sr stemic lupus erythe inatosus and wasstarted on intravenous methvlprednisone 24mg es cry 12 hours. Hisclinical status was markedlr i mpros ed. The patient was then dis—charge w ith oral pi’cdnisone 6(1 mg,’dar DiscussionThis is 76 v-ear—old man who initially presented with generalizedIymphadenopathv and then developed pericarditis. He fulfilled 4criteria of the 1052 ievised ci’iteria for SLfu with serositis, ahematolugical disorder, high ANA titer, and positis e anti—dsDNAantibodies. Hich AN.-\ titei’s are found niore often in SEE than otherautoimmune diseases. The homogenons ANA pattern. svhich svaspresent ni this case. is common in patients svith Sl.E hut is not very’specific. It can he seen in all the connective tissue disorders as svellas in drug-induced FE, This patient had been on only fluoxetine.There has been no report of’ fluoxetine and drug—induced FE. Thelow C3 and C4 les els also sLipport the diagnosis ol’SLF since severeRA. nephritis of non-SEE etiology, and liverdisease were abscnt. Inthis patient. a positis e AN,\ ss ith depressed complement les els, inthe absence of the above mentioned situations, are almost certain tohe associated with SLE,Lymphadenopathr has been reported to occur m 36 to (ml) U ofcases ol SI.E. Hosses er. Ir mphadenopathv as the first clniicalmanifestation, as in this case, is uncommon. in one series of 520patients ss oh SI E enlargement of cci’s ical lymph nodes was thcfirst clinical manifestation in 2 U of the patients. and generalizedlvmphadenopathy had occurred at the time of diagnosis in only I%‘. Therefore svhen this patient initially presented with lyniphad—enopathr . the other possible diagnoses had to he ruled out hr eitherlymph node hiopsr or fine needle aspiration The nodes in SI Fusual Ir are m mntendei’ and discrete, and t her s air m ‘a ic tim ‘m tessmilirnicterc to tm-I centimeters in diameter. Fr inphadenopathr ismore common in children than in adults and most marked amongblack patients. Patients with Ivmphadenopathv have more constitutional sy niptoms including fatigue. fes er and sr eight loss. morecutaneous sOns and symptoms, a hich rate of hepatomeualr andspleiioiimegalr . increased anti—dsDNA antibodies and decreasedcompleniemit Ieyel, There Is no dif[erence in renal mr centralnervous sr stem insmmls ement bcmsc ecu patmcnts ss oh Ir mphadcnopathy and those without Ivmphadenopathr - .A meta-analysis showedthat lymphadenopathy prevalence with late-onset 8FF was lower,-80
than in patients with early-onset SLE’’, The histological findings oflupus lvmphadenopathy are variable, ranging from fllIicuIarhyper—plasia. edema and sinus histiocytos is in the early stages to confluentnecrosis at late stages The characteristic flndmg in the l mph nodesof patients with SLE is a diffuse, reactive h perpIaa. There areh perplastic germinal centers with plasmac\ tosis and ariable numher of immunoblasts in the interfollicular areas. In thc necrotic areasand s dim the sinuses are occasional extracellular amorphousbodies. 5 to 12 microns in diameter. that stain intcnsel\ \ ithhemato\vlin, These “hematox\ liii bodies” sserc first described h(dntlcr and Fox in 194(1 It contains ggrcgate5 01 D\-\, imnmunoclohulins. and polvsaccharides. and ss hen present. thc\ arc considered to he characteristmc of lnpns K mphadcnmpathr Althoughhcmatoxylin hodies can also occur mu other disease-, such as progiessis e s stenuc sclerosis and rareR in patients ss mth h\ pcrlohulinemia. when clinical data is unavailable, the hemalox\ in bodiesCells resembling Rced—Sternhergare pathoenona nc of SEEmorpholo\ also have been described in patients ss nh SLL \entroIhese micro—phiL. eosi nophi Is. and ranulomata are sparsescopic leatures serve to distinenish lupus l inphadenitms from otherinfictiouc. immunologic, and vasculitis conditions- The inolecular genetic finding of olicoc lonal TcR rearrangements ma\ be aleature oh Si .E. or a concurrent but distinct disorder, such as the earlyphase of a lvmphoid ncoplasmThe age and mzender also have e fleets in clinical presentat i on andcourse m SI .E. Most m vest i eators report that female t male rat i Osss oh SLE aflcr age 50 were decreased slightl\ toX: I from 1(1 to IS: IPatients ss ith drug—induced lupus arc distiuctl older and usuall\male, likely because commonR used drugs such as procamnamideand hydralazine are widely used fur conditions in people os er ac 50years. SLE has no predilection for males who are older. but relativeto voungerpatients (less than 50 years old I. the numbers of men withSLE increase with age. One group found that the older SI.E patientpresents clinically more like the patient with drug-induced SEE thanone with idiopathicThis is because these patients have alow incidence of renal disease and, more prominent pleuropericardialand museuloskeletal symptoms’. Such older patients rarely havelow complement levels and native DNA antibodies. v. hich areopposite to the findings in this patient. The meta—aualysis of olderSLE patients revealed that serositis, interstitial pulmonary disease,anti La antibodies, and Sjogren’s syndrome symptoms (secondarysicca) were commonly associated with the disease of the older agegroup. Alopecia. Raynaud’s phenomenon, fever. K mphadenopathy, hypocomplernenternia. and neuropsychiatric disease were uncommon in this group. However, the analysis shoss ed no differences
HAWAII MEDICAL JOURNAL (USPS 237-640) Published monthly hr the Hasu an Medica.i Assoctation licorporeted in S56 under the Ninirelis 101 South Beretauj. Suite (1 Hr dulu. [Lusait ms 1—1-- Ph ne '101 CeO-iC:Eju ytb 5.7 Editors \rnian Goldstein MD