Transcription
Review ArticleMedial Epicondylitis: Evaluationand ManagementAbstractNirav H. Amin, MDNeil S. Kumar, MD, MBAMark S. Schickendantz, MDFrom the Department of OrthopaedicSurgery, Lenox Hill Hospital, NewYork, NY (Dr. Amin), the Departmentof Orthopaedic Surgery, DrexelUniversity College of Medicine,Philadelphia, PA (Dr. Kumar), and theDepartment of Orthopaedic Surgery,Cleveland Clinic, Cleveland, OH(Dr. Schickendantz).Dr. Schickendantz or an immediatefamily member serves as a paidconsultant to Arthrex; has stock orstock options held in TrazerHRA; andserves as a board member, owner,officer, or committee member of theAmerican Orthopaedic Society ofSports Medicine. Neither of thefollowing authors nor any immediatefamily member has received anythingof value from or has stock or stockoptions held in a commercial companyor institution related directly orindirectly to the subject of this article:Dr. Amin and Dr. Kumar.J Am Acad Orthop Surg 4-00145Copyright 2015 by the AmericanAcademy of Orthopaedic Surgeons.348Medial epicondylitis, often referred to as “golfer’s elbow,” is a commonpathology. Flexor-pronator tendon degeneration occurs with repetitiveforced wrist extension and forearm supination during activities involvingwrist flexion and forearm pronation. A staged process of pathologicchange in the tendon can result in structural breakdown and irreparablefibrosis or calcification. Patients typically report persistent medial-sidedelbow pain that is exacerbated by daily activities. Athletes may beparticularly symptomatic during the late cocking or early accelerationphases of the throwing motion. Nonsurgical supportive care includesactivity modification, NSAIDs, and corticosteroid injections. Once theacute symptomology is alleviated, focus is turned to flexor-pronatormass rehabilitation and injury prevention. Surgical treatment via opentechniques is typically reserved for patients with persistent symptoms.Medial epicondylitis, or “golfer’selbow,” is a pathology commonly encountered by orthopaedicsurgeons. Despite an overall prevalence of ,1%, medial epicondylitismay affect as many as 3.8% to 8.2%of patients in occupational settings.1-3Medial-sided pathology can be foundin as many as 10% to 20% of patientswith epicondylitis.4 A result of common flexor tendon (CFT) microtrauma and degeneration, medialepicondylitis typically occurs in thefourth through sixth decades of life,the peak working years, and equallyaffects men and women.1-3Although nonsurgical therapy andopen surgical management are mainstays of treatment, recent studies haveinvestigated the impact of nontraditional therapies such as extracorporeal shock wave therapy (ESWT)and modified surgical techniques.Anatomy and PathologyThe flexor-pronator tendon is the confluence of five muscles of the forearm:the pronator teres (PT), flexor carpiradialis, palmaris longus, flexor carpiulnaris (FCU), and flexor digitorumsuperficialis (Figure 1). This CFT isapproximately 3 cm long and, inmost elbows, crosses the ulnohumeral joint medially. The tendonattaches to the medial humeral epicondyle anteriorly and attachesproximally to the anterior bundle ofthe ulnar collateral ligament (UCL),with the fibers parallel to the UCL.5The CFT, particularly the ulnar headof the PT, also becomes confluentwith a hyperplastic section of theanteromedial joint capsule.Most authors believe the principlemechanism of injury is repetitiveeccentric loading of the muscles conducting wrist flexion and forearmpronation combined with valgusoverload at the elbow.6 Strain of themedial elbow with a valgus overloadmoment, which occurs with overheadthrowing, stimulates dynamic stabilization of the joint via eccentric contraction of the CFT. Simultaneouswrist flexion or forearm pronationJournal of the American Academy of Orthopaedic SurgeonsCopyright ª the American Academy of Orthopaedic Surgeons. Unauthorized reproduction of this article is prohibited.
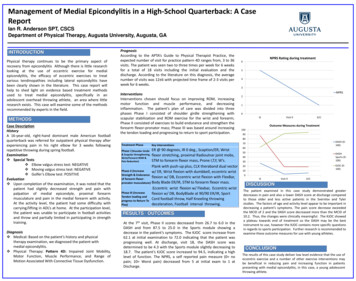
Nirav H. Amin, MD, et alFigure 1A and B, Photographs of a cadaver elbow demonstrating the ulnar nerve (UN), medial epicondyle (MEC), and the anatomyof the flexor-pronator muscles, including the pronator teres (PT), flexor carpi radialis (FCR), palmaris longus (PL), flexordigitorum superficialis (FDS), and flexor carpi ulnaris (FCU). (Reproduced with permission from Otoshi K, Kikuchi SI,Shishido H, Konno SI: The proximal origins of the flexor-pronator muscles and their role in the dynamic stabilization of theelbow joint: An anatomic study. Surg Radiol Anat 2014;36[3]:289-294.)during ball release may produce evengreater eccentric stress on the tendon.7 Historically, the PT has beenidentified as the primary dynamicstabilizer and the most likely musculotendinous unit to be injured inmedial epicondylitis. Recent cadaverstudies, however, have implicatedevery musculotendinous unit exceptthe palmaris longus.8-11Repetitive supraphysiologic stresson the tendon eventually results inmicrotrauma and degeneration. Histopathologic examination has revealed a staged process of pathologictendon change.12 Initially, repetitive trauma results in peritendinousinflammation. Continued injury results in angiofibroblastic hyperplasia,an invasion of vascular and fibroblastic elements into the tendon.Eventually, replacement of the normal tendon with angiofibroblastichyperplasia results in structuralbreakdown and irreparable fibrosisor calcification. Activity causing suchpathology to the CFT can eventuallytransfer forces deeper to the UCL,which mirrors CFT fiber orientationand histologic anatomy.5Clinical PresentationMedial-sided elbow pain encompasses a significant differential diagnosis, including ulnar neuritis,tendinopathy, ligamentous instability, intra-articular pathology, andtrauma. A thorough history andphysical examination is critical todetermine the likelihood of medialepicondylitis. In the athlete, this condition is typically associated withoverhead throwing, golf, or tennis;however, in the literature, it has beenassociated with other sports, including football, weightlifting, and bowling.13,14 Medial epicondylitis is alsocommonly found in occupationalsettings, especially those involvingrepetitive forceful grip, manual handling of loads .44 lbs (20 kg), orexposure to constant vibratory forcesat the elbow.1,2,14Patients typically present withpersistent medial-sided elbow painthat is often localized to the medialepicondyle, with radiation intothe proximal forearm. Elbow painis exacerbated by activity and isparticularly bothersome during thelate cocking phase in overheadthrowing or during early acceleration for the thrower, tennis player,or golfer.15 Patient history mayinclude an acute traumatic blow tothe elbow resulting in an avulsionof the CFT. More commonly, thepain is characterized by an insidious onset, with persistence despiterest.6Physical examination may detecttenderness 5 to 10 mm distal andanterior to the medial epicondyle thatis accompanied by soft-tissue swelling.6 Resisted wrist flexion, forearmpronation, or forceful grip may beweakened compared with that of thecontralateral side and may exacerbate elbow pain.16 Patients maypresent with elbow flexion contracture secondary to pain and guarding;however, most patients present withnormal passive and active range ofmotion (ROM) at the elbow andwrist. Peripheral neurovascular status is typically intact.Patients suspected of having medialepicondylitis should be examined forother pathologies of the ipsilateralJune 2015, Vol 23, No 6Copyright ª the American Academy of Orthopaedic Surgeons. Unauthorized reproduction of this article is prohibited.349
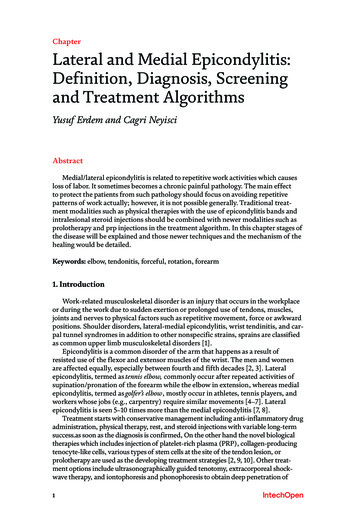
Medial Epicondylitis: Evaluation and ManagementFigure 2Axial (A) and coronal (B) T2-weighted fat-suppressed fast spin-echo magneticresonance arthrograms of the elbow. Abnormal high signal intensity withina thickened common flexor tendon (arrow) is visible on the axial view, indicatingmedial epicondylitis. On the coronal view, abnormal high signal intensity ispresent within a thickened common flexor tendon origin (arrow), and contrast isvisible at the lateral elbow injection site (arrowhead). (Reproduced withpermission from Kijowski R, De Smet AA: Magnetic resonance imaging findingsin patients with medial epicondylitis. Skeletal Radiol 2005;34[4]:196-202.)arm. Up to 84% of occupationalpatients may have concomitantwork-related disorders, such as carpal tunnel, lateral epicondylitis, orrotator cuff tendinitis.2 The overheadathlete must be examined for valgusinstability secondary to an injury tothe UCL. Evaluation of the UCL isperformed by applying valgus stressto the elbow in 30 of flexion, withthe forearm pronated and the wristflexed. Ciccotti and Ramani6 alsodescribed the use of the milking test,in which the examiner pulls on thethumb with the forearm supinatedand elbow flexed. Either maneuvermay elicit pain along the UCL, whichcan indicate an element of instabilityat elbow.Ulnar neuritis is another commonconcomitant pathology. In patientswith suspected ulnar neuropathy, theexamination should include twopoint discrimination in the ulnarsensory distribution and a comparison of the hypothenar bulk of thesymptomatic and asymptomaticextremities. A positive Tinel sign canindicate compression of the ulnarnerve. Proximally, overdevelopment350of the medial head of the triceps maycompress the nerve against the medialintermuscular septum.17,18 Distal tothe medial epicondyle, the ulnarnerve travels under the arcade ofStruthers and through the bifid FCUarcade distally, which may be inflamed and irritate the passingnerve.6 However, a positive Tinelsign may be found anywhere alongthe length of the nerve. Sensorychanges in the ulnar hand may bereproduced by applying stress to anirritated ulnar nerve via the elbowflexion test, which is performed withmaximal elbow flexion, forearmpronation, and wrist extension for30 to 60 seconds.6 The presence ofulnar nerve subluxation should alsobe noted during examination, especially in patients who report a popping sensation during daily activitiesor overhead throwing. Ulnar neuritiswith or without subluxation mayexacerbate medial-sided elbow pain;therefore, treatment modalities specifically for medial epicondylitisprovide inadequate relief. Patientswith neurologic complaints or findings should also be examined forsigns of cervical radiculopathy, particularly of the C6 and C7 roots,because these patients may be atincreased risk of developing medialepicondylitis secondary to forearmmuscle imbalance.19In addition to a thorough patienthistory and physical examination,radiologic studies can support orverify a diagnosis of medial epicondylitis. Although most radiographs demonstrate normal findings,up to 25% may show evidenceof calcification of the CFT or UCL.6Ultrasonography may be a costeffective modality for visualizingCFT tendinosis and pathologicchange. In a small series, Park et al20showed that a sonogram performedby a radiologist had sensitivity,specificity, and positive and negativepredictive values of .90% fordiagnosis of medial epicondylitis.The authors most commonly discovered hypoechoic or anechoicareas of focal tendon degenerationon ultrasonography. This modalityalso allows for dynamic examination, which may improve specificityand sensitivity.21 However, thediagnostic accuracy of ultrasonography is highly dependent on theoperator and may be less effectivewithout well-trained sonographers.MRI remains the standard of carefor radiologic detection of medialepicondylitis (Figure 2). NoncontrastMRI is effective for detecting pathologic change in the tendon, such asfrank tendinous disruption as well asother medial elbow pathology (eg,UCL or osteochondral injuries).22On T2-weighted sequences, intermediate to high signal intensity at theCFT, especially in the setting ofperitendinous edema, is indicativeof medial epicondylitis.23 Advancedimaging is typically used when concern for concomitant pathology ishigh (eg, evaluation of the UCL inthe overhead thrower) or if theclinical picture is unclear regardingthe source of medial elbow pain.Journal of the American Academy of Orthopaedic SurgeonsCopyright ª the American Academy of Orthopaedic Surgeons. Unauthorized reproduction of this article is prohibited.
Nirav H. Amin, MD, et alManagementVarious nonsurgical and surgicaltreatment modalities are used tomanage medial epicondylitis. Thegoals, however, remain similar: torelieve acute symptomatology, rehabilitate the pathologic tendon, andprevent future recurrence. As withmany chronic tendinopathies, nonsurgical therapy is the mainstay oftreatment. Surgical procedures aretypically reserved for patients withrecalcitrant or recurrent symptomsdespite nonsurgical management.Acute SymptomsThe initial focus of nonsurgical supportive care is the relief of medialsided elbow pain. Patients shouldrefrain from activities that instigateor exacerbate symptoms, especiallythose that require repetitive wristflexion, forearm pronation, and valgus stress about the elbow. Athleteswith concomitant UCL injury shouldrefrain from throwing for 6 to 12weeks, with particular care taken toavoid valgus stress during the first6 weeks of treatment. Periods of acutepain and swelling may be alleviatedwith icing, which provides both analgesic and vasoconstrictive effects.6NSAIDs may also provide effectivepain relief and may be used routinelyfor 1 to 2 weeks as tolerated bythe patient. These medications areparticularly effective in reducing thesynovitis associated with flexorpronator tendon degeneration.6,23Night splinting and supportiveorthoses may be used simultaneously,especially extension splinting inpatients with ulnar neuritis. Counterforce bracing limits the maximalcontractile force generated by theflexor-pronator musculotendinousunit.6 Chang et al24 demonstratedpain relief in baseball pitchers withmedial epicondylitis by using forearmkinesiology taping techniques asa method of counterforce bracing.However, splinting and bracingshould not involve prolonged elbowimmobilization secondary to jointstiffness. In the setting of injury to theUCL, a hinged elbow brace can beused to provide varus-valgus stabilityand prevent full elbow extension.ESWT may provide pain relief fora subset of patients. Electrical stimulation of the diseased tendon maypromote angiogenesis, tendon healing, and some degree of short-termanalgesia.25 In a study of patientswith newly diagnosed epicondylitistreated with ESWT or steroid injection, Lee et al26 reported worse clinical pain scores at 1 and 2 weeks withESWT, but better patient satisfactionat 8 weeks. However, Krischek et al27reported excellent or good clinicalresults with ESWT in only 7 of 30patients at 1-year follow-up, whichwas notably worse than the resultsachieved in patients with lateralepicondylitis who underwent similar treatment. Definitive recommendations for the use of shockwavetherapy for medial epicondylitis,including treatment duration andstimulation protocol, cannot be madeat this point.When noninvasive techniques proveinadequate, a corticosteroid injectionis often effective in reducing medialelbow discomfort. The corticosteroidis injected into the peritendinous andsynovial tissues rather than intothe tendon itself.6 Similar to oral antiinflammatory medications, the corticosteroid may reduce the surrounding synovitis and resultant pain.Historically, direct injection deep tothe flexor-pronator tendon hasbeen the delivery technique of choice,although transcutaneous methodsmay be effective, as well.28 Careshould be taken to prevent iatrogeniccomplications such as subcutaneousatrophy, tendon weakening, or nerveinjury. Local depigmentation mayoccur as well, especially in patientswith darker skin.6,29 Needle injectionalso provides the benefit of tendontrephination, which may stimulatebleeding and tendon healing.30 Ina prospective study of 60 elbowstreated with steroid injection formedial epicondylitis, Stahl andKaufman31 noted an acute improvement in pain during the 6 weeks afterinjection but no difference by 3months. Lee et al26 demonstratedeven shorter-term gains after steroidinjection, with acute improvement inpain scores over the first 2 weeksfollowed by a plateau for up to 8weeks. Suresh et al30 combined needle stimulation and injection ofautologous blood into the disruptedtendon, which resulted in decreasedvisual analog scale and Nirschl scoresat 10 months.Rehabilitation andPreventionPhysical therapy and rehabilitationremains a central aspect of recoveryfrom medial epicondylitis. Onceacute symptoms are alleviated, thefocus turns to flexor-pronator massstretching and strengthening. Eachphase of rehabilitation requires thepatient to perform targeted exerciseswith increasing repetition and speed.A return to full, painless ROM is theinitial goal. Motion of the wrist andelbow is emphasized, with open chainexercises (non-weight bearing) andself-directed passive stretching techniques. Shoulder ROM is emphasizedin the overhead thrower and in nonathletes with concomitant shoulderpathology. Elbow extension mayneed support with extension blockbracing if a baseline flexion contracture exists. Passive ROM and eccentric contraction are avoided initiallyto prevent applying unintendedexcessive stress on the tendon. Oncea painless functional motion arc isachieved, tendon strengthening begins. Concentric open and closedchain exercises are used, withincreasing weight and repetitions toincrease flexor-pronator mass power.June 2015, Vol 23, No 6Copyright ª the American Academy of Orthopaedic Surgeons. Unauthorized reproduction of this article is prohibited.351
Medial Epicondylitis: Evaluation and ManagementFinally, eccentric strengthening is implemented. All patients, particularlythrowers, benefit from strengtheningof the shoulder girdle and scapularstabilization. Core and lower bodystrengthening may also aid in throwing mechanics and activities involvingmoderate to heavy resistance. Ultimately, reconditioning of the upperlimb to maintain tendon excursionand strength during rigorous tendonstress is central to preventing unduestress about the elbow and a recurrence of symptoms.Currently, no specific guidelinesexist regarding return to sport,32although Ciccotti and Ramani6 suggested a progressive return to sportonce the patient can tolerate sprintrepetitions of concentric and eccentricresistance exercises. Sport-specificconcerns, such as equipment andtechnique, should also be addressed toreduce undue stress at the elbow.Elbow pads may alleviate symptomatic ulnar nerve subluxation duringathletic activity. In the selection of golfclubs, the length, shaft weight, clubhead weight, and club head strikezone must be considered. Propertechnique is particularly important,especially in the amateur athlete.Medial epicondylitis is often found inthe trail arm of the swing, secondaryto greater valgus stress than that in thelead arm.9 Stress on the PT of the trailarm is more likely in amateur golfersthan in professionals, who use thelead arm in a protective manner toobtain optimum swing speed andpower without excessive stress.In tennis, racquet size, weight, headweight, strike zone, and string tension can impact stress at the elbow.Amateurs may benefit from vibrationdampeners directly attached to thestrings. Ilfeld33 described poor forehand stroke mechanics as a cause ofmedial elbow stress. Late ball strike,with the racquet head behind theelbow at contact, was a significantcontributor to medial epicondylitis.It can be exacerbated with an open-352stance technique, particularly witha topspin stroke, which relies onrapid angular acceleration to thedisadvantageous strike point.Surgical OptionsSurgical débridement for medial epicondylitis is typically reserved for patients with persistent symptomsdespite an aggressive regimen ofnonsurgical therapy for 4 to 6 months.The exception to this guideline is theelite athlete with definitive tendondisruption appreciable on MRI.6 Forthese patients, surgical repair of thetendon may allow return to sport atpreinjury performance levels earlierthan nonsurgical treatment. TheMorrey classification is used to guidesurgical goals.34 Type I lesions requireepicondylar débridement. Pathologyinvolving ulnar nerve symptomsrequire decompression (type IIA) orsubmuscular transposition (type IIB).To date, there is no literature available on arthroscopic management ofmedial epicondylitis. The currenttechnique of elbow arthroscopy isbelieved to place the medial collateralligament and ulnar nerve at risk ofiatrogenic injury.6 In cadaver studiesof the medial elbow, an anteromedialportal 1 cm anterior and 1 cmproximal to the medial epicondyleand a modified “mobile” secondarymedial portal off the anterior aspectof the distal humerus were used.35,36However, the clinical efficacy of suchtechniques for medial epicondylitishas yet to be explored.Currently, surgical management ofmedial epicondylitis is performedusing an open procedure similar tothe method described by Ciccotti andRamani6 (Figure 3). An incision ismade at the medial epicondyle withcare taken to avoid injury to themedial antebrachial cutaneous nerveduring subcutaneous dissection.Pathology of the PT is common,and further exposure of diseasedmusculocutaneous tissue is accom-plished using the PT–flexor carpiradialis interval. The CFT is exposedand examined for friable tissue,which is débrided. This techniqueallows the surgeon to visualize andprotect both the ulnar nerve posterior to the medial epicondyle and theUCL deep to the CFT, particularlythe anterior band. These structuresmay require secondary proceduressuch as nerve decompression, transposition, ligament repair, or reconstruction. For focal CFT lesions,limited débridement with side-toside tendon repair may be performed. For lesions with significantdisease, more extensive débridementmay be indicated followed by CFTreattachment en mass to the medialepicondyle. The epicondyle is microfractured before tendon reattachment to provide a vascular bedfor tendon insertion. Using thistechnique, Vangsness and Jobe13reported excellent or good results in34 of 35 patients with medial epicondylitis, and only 1 patient failedto return to preinjury athletic performance at 6-year follow-up.Cho et al37 described a modifiedmethod, using a mini-open muscleresection technique in 10 patientswith epicondylitis. A 1.5-cm incisionwas made at the medial epicondyleto expose the flexor-pronator tendonpathology, which was grossly debulked. After epicondylar microfracture, the overlying fascia wasclosed over the tendon, creating anenclosed hematoma to promotehealing. The débrided tendon wasnot repaired nor was it completelyremoved and reattached to the epicondyle. All 10 patients returned totheir respective occupations within 3months and no poor results werereported. This technique, however,may limit exposure to the ulnarnerve, which may also be symptomatic and require decompression.Failure to address additional medialelbow pathologies could result infailure of surgical treatment. GabelJournal of the American Academy of Orthopaedic SurgeonsCopyright ª the American Academy of Orthopaedic Surgeons. Unauthorized reproduction of this article is prohibited.
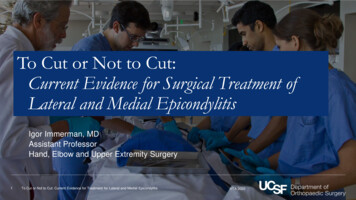
Nirav H. Amin, MD, et aland Morrey38 reviewed 30 elbowswith medial epicondylitis (16 ofwhich had concomitant ulnar neuropathy) treated with various opentechniques of tendon débridementand ulnar nerve procedures. Patientswith mild ulnar neuropathy did notpresent preoperatively with a sensoryor motor deficit and exhibited noevidence of nerve compression intraoperatively. Moderate and severeneuropathy was determined by subjective response to provocation testing via sustained elbow flexion, Tinelsign, and direct nerve compression.Of the 25 elbows with no or mildulnar neuritis, 24 had excellent orgood outcomes at a mean 7-yearfollow-up. However, three of thefive patients with elbows with moderate or severe ulnar neuropathy reported fair or poor results at finalfollow-up. The authors noted that theonly preoperative or intraoperativeparameter correlated to outcome wasthe severity of ulnar neuropathy.Kurvers and Verhaar39 reporteda similar result in their series of 38patients with medial epicondylitistreated surgically. Eleven of 16 patients treated with tendon débridement and reattachment were symptomfree by a mean 44-month follow-up.However, of 24 patients with concomitant ulnar neuritis treated withnerve decompression, only 3 weresymptom free at final follow-up.Gong et al40 described an alternativesurgical technique in 19 patients withmedial epicondylitis and ulnar neuritis. The ulnar nerve was decompressedfrom the cubital tunnel and releasedfrom the two heads of the FCU viaa Z-lengthening of the flexor-pronatormass. The proximal limb remainedattached to the medial epicondyle,while the distal limb was translateddistally and repaired, with the nerveresting upon the brachialis. At a mean38-month follow-up, all patients reported improved pain scores at restand with activity, as well as completerelief of neuropathic symptoms.Figure 3Intraoperative photographs of an elbow with medial epicondylitis showing thepathologic change of the intact common flexor tendon (A), the tendon afterdébridement of diseased tissue (B), exposure of the medial epicondyle (C), andside-to-side repair of the common flexor tendon (D).Depending on the severity of CFTdisease, postoperative care mayinvolve gentle arm use or immobilization of the limb in 90 via a splint orsling for 1 to 2 weeks postoperatively.After this period, active ROM isbegun, with return to activities ofdaily living. Strengthening exercisesare started at 6 to 8 weeks postoperatively, with eventual return tofull activity or sport at 3 to 6 months.SummaryMedial epicondylitis involves degeneration of the flexor-pronator mus-culotendinous mass of the forearm.Most patients with this condition arenot athletes; however, medial epicondylitis has been associated withthe throwing athlete, golfer, orpatient whose work requires repetitive wrist flexion. Patients typicallypresent with persistent medial elbowpain during activities of daily livingthat is unrelieved with rest. Athletesmay be particularly symptomaticduring the late cocking or earlyacceleration phases of the throwingmotion. Nonsurgical management isgenerally effective in reducing dailysymptoms and allowing return tosport at preinjury levels. Initially,June 2015, Vol 23, No 6Copyright ª the American Academy of Orthopaedic Surgeons. Unauthorized reproduction of this article is prohibited.353
Medial Epicondylitis: Evaluation and Managementefforts are focused on pain relief byreducing peritendinous synovitis andresisting tendon degeneration vianoninvasive and invasive methods.Physical therapy and sport-specificrehabilitation programs are used forstrengthening and prevention of reinjury. For elite athletes with distincttendon disruption or patients withsymptoms that are refractory to nonsurgical treatment, open débridementand simultaneous treatment of secondary pathologies can be beneficial.Such patients typically return to preinjury performance at 3 to 6 monthspostoperatively.AcknowledgementThe authors would like to thank T.Sean Lynch, MD, and Ronak Patel,MD, for their guidance and manuscript writing.References1. Shiri R, Viikari-Juntura E, Varonen H,Heliövaara M: Prevalence anddeterminants of lateral and medialepicondylitis: A population study. Am JEpidemiol 2006;164(11):1065-1074.2. Descatha A, Leclerc A, Chastang JF,Roquelaure Y; Study Group on RepetitiveWork: Medial epicondylitis in occupationalsettings: Prevalence, incidence andassociated risk factors. J Occup EnvironMed 2003;45(9):993-1001.3. Wolf JM, Mountcastle S, Burks R,Sturdivant RX, Owens BD: Epidemiology oflateral and medial epicondylitis in a militarypopulation. Mil Med 2010;175(5):336-339.4. Baumgard SH, Schwartz DR: Percutaneousrelease of the epicondylar muscles forhumeral epicondylitis. Am J Sports Med1982;10(4):233-236.5. Otoshi K, Kikuchi S, Shishido H, Konno S:The proximal origins of the flexor-pronatormuscles and their role in the dynamicstabilization of the elbow joint: An anatomicalstudy. Surg Radiol Anat 2014;36(3):289-294.6. Ciccotti MG, Ramani MN: Medialepicondylitis. Tech Hand Up Extrem Surg2003;7(4):190-196.7. Sisto DJ, Jobe FW, Moynes DR,Antonelli DJ: An electromyographicanalysis of the elbow in pitching. Am JSports Med 1987;15(3):260-263.3548. Park MC, Ahmad CS: Dynamiccontributions of the flexor-pronator massto elbow valgus stability. J Bone Joint SurgAm 2004;86(10):2268-2274.22. Walz DM, Newman JS, Konin GP, Ross G:Epicondylitis: Pathogenesis, imaging, andtreatment. Radiographics 2010;30(1):167-184.9. Farber AJ, Smith JS, Kvitne RS, Mohr KJ,Shin SS: Electromyographic analysis offorearm muscles in professional andamateur golfers. Am J Sports Med 2009;37(2):396-401.23. Kijowski R, De Smet AA: Magneticresonance imaging findings in patients withmedial epicondylitis. Skeletal Radiol 2005;34(4):196-202.10. Udall JH, Fitzpatrick MJ, McGarry MH,Leba TB, Lee TQ: Effects of flexorpronator muscle loading on valgusstability of the elbow with an intact,stretched, and resected medial ulnarcollateral ligament. J Shoulder Elbow Surg2009;18(5):773-778.11. Lin F, Kohli N, Perlmutter S, Lim D,Nuber GW, Makhsous M: Musclecontribution to elbow joint valgus stability.J Shoulder Elbow Surg 2007;16(6):795-802.12. Regan W, Wold LE, Coonrad R,Morrey BF: Microscopic histopathology ofchronic refractory lateral epicondylitis. AmJ Sports Med 1992;20(6):746-749.13. Vangsness CT Jr, Jobe FW: Surgicaltreatment of medial epicondylitis: Results in35 elbows. J Bone Joint Surg Br 1991;73(3):409-411.14. Galloway M, DeMaio M, Mangine R:Rehabilitative techniques in the treatmentof medial and lateral epicondylitis.Orthopedics 1992;15(9):1089-1096.15. Cain EL Jr, Dugas JR, Wolf RS,Andrews JR: Elbow injuries in throwingathletes: A current concepts review. Am JSports Med 2003;31(4):621-635.24. Chang HY, Wang CH, Chou KY,Cheng SC: Could forearm kinesio tapingimprove stren
treatment modalities are used to manage medial epicondylitis. The goals, however, remain similar: to relieve acute symptomatology, reha-bilitate the pathologic tendon, and prevent future recurrence. As with many chronic tendinopathies, non-surgical therapy is the mainstay of treatment. Surgical procedures are typically reserved for patients with