Transcription
ADDICTION AND RECOVERY TREATMENTSERVICES (ARTS) MANUAL UPDATESMARCH 2022Ashley Harrell, LCSWARTS Senior Program AdvisorKe’Shawn Harper, MIS, QMHP-AARTS Senior Policy SpecialistJessica Johnson, MA, Resident in CounselingARTS Service CoordinatorSonya Reyes-McDonald, MAARTS Program AnalystOketa Winn, LPCBehavioral Health Program SupervisorVirginia Department of MedicalAssistance Services
Closed Captioning Service Automated CC is available for this event with realtimecaptions that will run simultaneously with thepresentation. The streaming text is available through:https://www.streamtext.net/player?event HamiltonRelayRCC-0309-VA3365 We recommend opening a second window with the linkprovided and resizing it in such a fashion that it appearsbelow the webinar screen. This allows the viewer to seeboth the webinar and its associated text/graphics whilealso being able to comfortably view the realtimecaptions. 2If you have any questions about this service please send an emailto CivilRightsCoordinator@DMAS.Virginia.Gov
Townhall PostingChapters that were reviewed 3Chapter 2Chapter 4Chapter 5Chapter 6
Public commentsScope of practice for CSAC and CSAC-Supervisees The manual clarifies the scope of practice based on the regulation andauthority given by the Board of Counseling. Allows CSACs and CSAC-Supervisees to complete: The multidimensional assessment for all ASAM levels except ASAM Level1.0 and 4.0; The comprehensive ISP Under the supervision of a CATP who must sign off on the assessment andISP within three business days. CSACs and CSAC-Supervisees are not included in the definition of aCATP, but within individual services are able to provide care tomembers.4
Public commentsARTS Provider Qualification inia.gov/wps/portal/ProviderManual5
Public commentsISP Requirements/Reviews The initial and Comprehensive ISP can be developed by the CSAC orCSAC-Supervisees in all ASAM levels with the exception of 1.0 and 4.0. Reviews of the ISP can be done by CSAC or CSAC-Supervisees if theCATP signs off within one business day. Comment: Not require physician/psychiatrist consult for ISPs or ServiceAuthorizations DMAS Response: Higher medically/clinically focused settings requireconsultation per ASAM.6
Public commentsPeers Registration Comment: Delete requirementfor Peers certification andregistration with the Board.Allow peers to gain theseexpertise over a 15 monthperiod, similar to the time framegiven for STEP-VA peers tobecome certified before billingMedicaid.7 DBHDS requires all PeerRecovery Specialists (PRS) to becertified The General Assemblyauthorized the Board ofCounseling in 2017 to registerPRS. DMAS requires the certificationand registration with the Boardof Counseling to submit forreimbursement
Public commentsTelehealth 8Comment: Licensed physicians or physicianextenders under supervision of a physician shallperform physical examinations for allindividuals who are admitted ” Could this bedone with a licensed provider over telehealthwhen a nurse (or other medical staff) isphysically present with a patient in thetreatment program? DMAS Response: Telehealth is defined inchapter 4 and the Telehealth Supplement.Comment: Page 23 contains the definition ofTelemedicine which exclusively includes “the useof audio and video equipment.” Can astipulation be added to this that in the event ofa technical emergency (utility failure, internetoutage, etc.) audio-only services will beaccepted? DMAS Response: Audio only was anallowed flexibility during the Federal PublicHealth Emergency, but is not allowed in theTelehealth Supplement
Public commentsSubstance Use Care Coordination Comment: Care Coordinationshould absolutely includeassisting patientswith Medicaid transportation because the service is horrible.Patients are stranded for hoursand unable to get anyone to helpthem despite repeated calls fromthe patient and our staff. DMAS Response: Schedulingtransportation cannot be the soleactivity to support monthly billing.9
Transportation ConcernsSteps for Members Having Transportation Concerns1. Ensure the Member is calling the NEMT Ride Assist telephone numberand file a complaint or tell the CSR the provider hasn't returned forthe transport.2. Ensure the Member gets a complaint number3. If the issue continues, send the following information Name of MemberMember Medicaid ID not MCO ID numberMember Telephone numberMCO they are enrolled with if knownAddress of the clinic and what days they goComplaint numbers and any info given Member from their NEMTprogram Ride AssistGive a brief description of the issue.
Preferred Office-Based Opioid Treatment (OBOT) Services As of February 24, 2022, there are 193 OBOTproviders in the Commonwealth. 60 in Southwest VA & Tennessee region 30 in Northern VA region 29 in Tidewater region 26 in Central VA region Per the Opioid Treatment Services manualsupplement, the foundation of the PreferredOBOT model is to provide the medical andbehavioral health services within the samelocation, have in-person interactions with themember and care coordination to support themember in their recovery. Preferred OBOT services may be provided viatelehealth based on the individualized needs ofthe member and must have supportingdocumentation detailing the exception oftelehealth (transportation, childcare,employment, co-morbidities) that impede theiraccess to treatment.11
Preferred Office-Based Opioid Treatment (OBOT) ServicesProvider RequirementsBuprenorphine-Waivered Practitioner Must have complete one of the continuingmedical education courses approved by theCenter for Substance Abuse Treatment andobtained the waiver to prescribe ordispense buprenorphine for opioid usedisorder required under the Drug AddictionTreatment Act of 2000 and have a DrugEnforcement Agency (DEA)-X numberissued and included on all buprenorphineprescriptions for treatment of opioid usedisorder. Nurse Practitioners and PhysicianAssistants prescribing buprenorphine,who have obtained a SAMHSA waiverand the appropriate DEA registrationshall prescribe under a practiceagreement with a waivered doctor ofmedicine or doctor of osteopathicmedicine.12
Preferred Office-Based Opioid Treatment (OBOT) ServicesProvider RequirementsBuprenorphine-Waivered Practitioner A nurse practitioner to whom alicense is issued by endorsementmay practice without a practiceagreement with a patient careteam physician if suchapplication provides anattestation to the Boards thatthe applicant has completed theequivalent of at least two yearsof full-time clinical experience,as determined by the Boards, inaccordance with the laws of thestate in which the nursepractitioner was licensed(defined in §54.1-2957).13
Preferred Office-Based Opioid Treatment (OBOT) ServicesProvider RequirementsLicensed Behavioral Health Practitioner an addiction-credentialed physicianor physician with experience ortraining in addiction medicine; physician extenders withexperience or training in addictionmedicine; a licensed psychiatrist; a licensed clinical psychologist; a licensed clinical social worker; a licensed professional counselor; a registered psychiatric clinicalnurse specialist; a licensed psychiatric nursepractitioner;14
Preferred Office-Based Opioid Treatment (OBOT) ServicesProvider RequirementsLicensed Behavioral Health Practitioner licensed marriage and family therapist; licensed substance abuse treatmentpractitioner residents under supervision of a licensedprofessional counselor (18VAC115-20-10),licensed marriage and family therapist(18VAC115-50-10), or licensed substanceabuse treatment practitioner (18VAC11560-10) and registered with the VirginiaBoard of Counseling; residents in psychology under supervisionof a licensed clinical psychologist andregistered with the Virginia Board ofPsychology (18VAC125-20-10); supervisees in social work under thesupervision of a licensed clinical socialworker and registered with the VirginiaBoard of Social Work (18VAC140-20-10).15
Preferred Office-Based Opioid Treatment (OBOT) ServicesProvider RequirementsCare Coordinator Must be under the general supervision of a buprenorphine waivered practitioner orCredentialed Addiction Treatment Professional by employment or a contractualrelationship with either the buprenorphine waivered practitioner, LicensedCredentialed Treatment Professional, or the organization employing thebuprenorphine waivered practitioner or Credentialed Addiction TreatmentProfessional: At least a bachelor's degree in one of the following fields (social work, psychology,psychiatric rehabilitation, sociology, counseling, vocational rehabilitation, human servicescounseling) and have one of the following qualifications (i) substance use related directexperience providing services to individuals with a diagnosis substance abuse use disorderor (ii) clinical experience working with individuals with co-occurring diagnoses of substanceuse disorder and mental illness; or Licensure by the Commonwealth as a registered nurse with (i) substance use related directexperience providing services to individuals with a diagnosis of substance use disorder or(ii) clinical experience working with individuals with co-occurring diagnoses of substanceuse disorder and mental illness; or Board of Counseling CSAC, CSAC-Supervisee or CSAC Assistant under supervision asdefined in 18VAC115-30-10 et seq.16
Primary Evaluation Aims for ARTS:Virginia Commonwealth University Access to treatment services for Medicaid members withsubstance use disorders Quality of treatment services Outcomes of treatment (Under waiver extension) Assess cumulative impact of ARTSand Medicaid expansion on Virginia population17
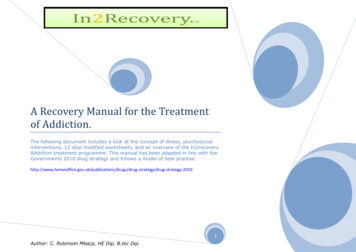
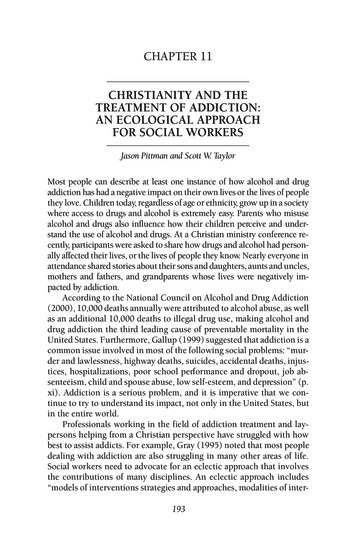
Prevalence of Substance Use Disorder (SUD) AmongMedicaid 48,94152,88758,94940,00020,00001820162017 (ARTS)20182019 (Expansion)2020
Changes in Treatment Rates for Base Medicaid 9202020.0%10.0%0.0%20172018SUD19OUDAUD
Addiction Treatment Providers Serving MedicaidMembers*Provider TypeInpatient Detox (ASAM 4)N/A55NEW41393175%Partial Hospitalization Programs (ASAM 2.5)N/A47NEWIntensive Outpatient Programs (ASAM 2.1)49284480%Opioid Treatment Programs643617%N/A193NEW1,0875,089368%Residential Treatment (ASAM 3)Preferred Office-Based Opioid TreatmentProvidersOutpatient practitioners billing for ARTS services(ASAM 1)*Magellan of Virginia – BHSA Network July 202120%# of# of ProvidersProviders IncreaseBeforeinin ARTSARTSYear 4 Providers
Preferred Office-Based Opioid Treatment (OBOT) ProviderAligning Evidence-Based Practices for Treatment of Opioid Use Disorder Specific requirements for being approved as a Preferred OBOT Increased rates for these enhanced servicesSetting Primary care clinics, outpatient health system clinics, psychiatry clinics, Federally-QualifiedHealth Centers (FQHC), Community Services Boards (CSB), Health Departments, and physicianofficesStaffing Buprenorphine-waivered practitioner (physician, NP or PA) Licensed credentialed addiction treatment professionals (e.g., LCSW, LPC, licensed clinicalpsychologist, etc.) NurseSupport Systems Care Coordination Access to emergency medical and psychiatric care and connections for referrals to higherlevels of care21
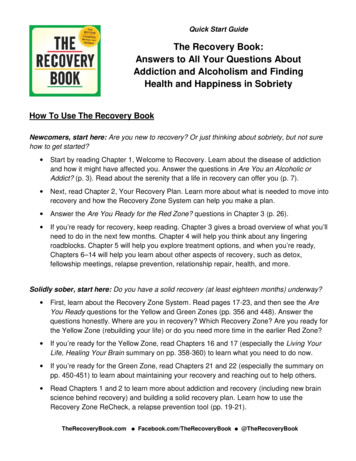
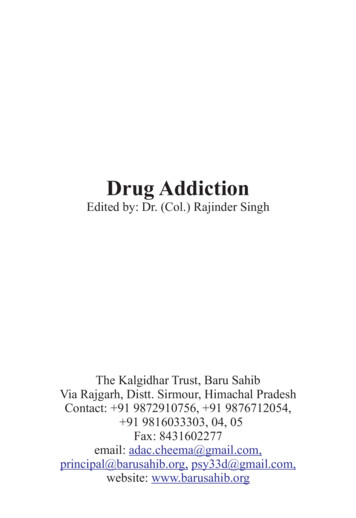
Leveraging the Evidence-Based model for OUD Care coordination services provided byPreferred Office-Based Opioid Treatment(OBOT) and Opioid Treatment Programsfacilitate integration of addictiontreatment services with physical healthand social service needs. Rates of MOUD use were higher duringepisodes of treatment at Preferred OBOTproviders (81%), compared to otheroutpatient providers (56%). Co-prescribing of opioid pain medicationand benzodiazepines declined formembers receiving treatment for OUDthrough Preferred OBOTs.193 OBOT sitesand 43 OTPs!Number of Medicaid Members ReceivedMOUD35,000 18,30711,7765,00002016222017201820192020
Expanding the Preferred OBOT model to allow for otherprimary SUD – MARCH 1, 2022 DMAS just posted the updated Preferred Office-BasedAddiction Treatment (OBAT) and Opioid Treatment ProgramSupplemental manual on March 3, 2022, effective March 1,2022. Allows for reimbursement within the OBAT model for treatingother primary SUD. Training coming soon!23
COVID-19 Accelerated Overdose Deaths Nationally"As we continue toaddress both theCOVID-19 pandemicand the opioid crisis,we must prioritizemaking treatmentoptions more widelyavailable to peoplewith substance usedisorders."CDC Data: Fatal -overdose-deaths-2020/index.htmlrates increase by 30% in 2020Estimated 100,306 people died in 12 month period ending April 202124https://www.cdc.gov/nchs/pressroom/nchs press releases/2021/20211117.htm
And in VirginiaFatal Drug Overdose Trends in Virginia –3rd Quarter 2021 orensic-epidemiology/25
WHY do we continue to see an historicrise in overdose deaths in spite ofbetter access to providers andtreatment?26
An Evolving Strategy to Address the Epidemic High quality / EvidenceBased Care Pregnant andparenting individualsJustice-involvedPriority Populations andTheir FamiliesTransitions of Care 27Needs assessmentBrightspot/Strengthsbased AssessmentUtilizing Data MOUDASAMPeer RecoverySupportsAcute CareEmergency RoomInstitutional Stays
High Quality / Evidence-Based Care Expanding the Preferred Office-Based Opioid Treatment (OBOT) model Allowing reimbursement for serving members with other primarySubstance Use Disorders as well as Opioid Use Disorder – March 1, 2022 Added allowance of Preferred OBOT services provided in a mobile unit Fostering collaboration with Health Systems for ED Bridge Clinics Expanding access to Peer Recovery Support Services (PRSS) Streamlined and standardized the registration process across all MCOs Facilitated workgroups and implemented recommendations to removebarriers for service delivery In collaboration with the Department of Behavioral Health andDevelopmental Services (DBHDS) created one-pagers to promote PRSSand a guidance document for treatment planning documentation thatproviders requested28
High Quality / Evidence-Based Care The 2020 General Assembly directed the Department of BehavioralHealth and Developmental Services (DBHDS) to utilize emergencyauthority to promulgate licensing regulations that align with theAmerican Society of Addiction Medicine (ASAM) Levels of Care Criteria“to ensure the provision of outcome-oriented and strengths-based carein the treatment of addiction.” Following the issuance of the conditional license, a representative of OLwill conduct a thorough review of each provider’s compliance with theemergency regulations as part of the annual inspection. Once compliance with all the applicable regulations within each serviceis demonstrated, including the new DBHDS regulations incorporatingthe ASAM Criteria for the corresponding service, then an annual licensewill be granted.29
SUPPORT Act Section 1003Virginia applied and was awarded 4.9M in September 2019 from theCenters for Medicare and Medicaid Services (CMS) to increase Substance UseDisorder provider capacity Building Providers’ substance use disorder (SUD)Knowledge/Skills/Abilities: Total of 150 free SUD provider trainingwebinars and technical assistance sessions with a total of over 9,000attendees. Including 3 buprenorphine waiver trainings for prescribers. Conducting surveys to understand the experiences of ARTS membersand SUD providers. Statewide Needs Assessment and identifying Brightspot communitiesusing data visualization through HealthLandscape30
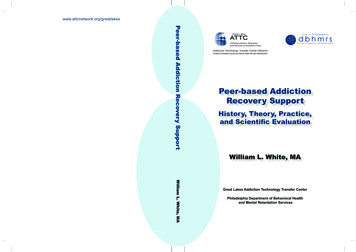
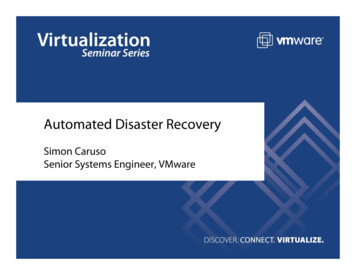
HealthLandscape - 2019Opioid Overdose Deaths per 100KBuprenorphine WaiveredPractitioners per 100KWorkforce aligns with where deaths used to be and not where they are now.31
SUPPORT Act Grant Activities, cont. Bi-monthly Stakeholder meetings to report out on grant activities Recommendations for leveraging Managed Care Organizations toincrease access to care Created Hepatitis C Treatment Provider map to promote screeningand treatment access Expanding new types of SUD treatment and connections to care modelssuch as the Emergency Department Bridge Clinics, telehealth,increasing access to PRSS and enhancing collaboration with PublicSafety and Medicaid to improve access to services for those involved inthe carceral system32
Utilizing Data Leveraging Medicaid Managed Care Organizations and External QualityReview Organization Development of performance measures and specifications Concurrent Prescribing of Naloxone and High Dose Opioids Naloxone Use for High Risk of Overdose Treatment of Hepatitis C for those with Hepatitis C and Substance UseDisorder (SUD) Treatment of Human Immunodeficiency Virus (HIV) for those with HIV andSUD Preferred Office-Based Opioid Treatment (OBOT) Compliance Cascade of Care for Members with Opioid Use Disorder (OUD) Cascade of Care for Members with Hepatitis C Cascade of Care for Members with HIV33
Winter 2022 Webinar Schedule FREE webinars for anyone who serves Medicaid Member Registration is now open. Use links in schedule to register andaccess the webinars.New Topic: Substance Use DisorderTreatment for AdolescentsPresented on: March 22nd and March 24thRevisiting Topics:- Opioids, Stimulants & Cannabis- ASAM Criteria Assessment Dimensions 1 - 6( Four part series)**- Urine Drug Screenings: Purpose & Practice- Suicide Assessment- SUD & Trauma- Co-Occurring Disorders (Two parts series)Webinar Schedule and Slide Decks are available on the SUPPORT grant website: nt/34
Additional Questions?Call the ARTS Helpline at (804) 593-2453Email: SUD@dmas.virginia.govARTS /addiction-and-recovery-treatmentservices/35
registered with the Virginia Board of Psychology (18VAC125-20-10); supervisees in social work under the supervision of a licensed clinical social worker and registered with the Virginia Board of Social Work (18VAC140- 20-10). Licensed Behavioral Health Practitioner. 15. Preferred Office-Based Opioid Treatment (OBOT) Services