Transcription
Hospice of Southern IllinoisNursingProceduresManual
Table of ContentsI.Catheterization of Bladder (Includes Female and Male)II.Gastrostomy and Jejunostomy TubesIII.IV Skills (Includes IV Catheter Gauge Selection)a. Subcutaneous (SQ) Infusionb. Peripheral Infusionc. Central Venous Access Devices (CVAD)d. VenipunctureIV. Nasogastric (NG) Intubation (Includes Insertion, Irrigation, andRemoval)V.Ostomy Care (Includes Ostomy Reference Guide)VI. PleurX Drainage Procedure (Includes Aspira Drainage SystemQuick Reference)VII. Tracheostomy Suctioning and CareVIII. Wound Care Management (Includes Venous and ArterialInsufficiency Reference Guides)a. Pressure Injuriesb. Venous Ulcersc. Arterial Ulcersd. Malignant Woundse. Measuring and Dressing Guidelines
Hospice of Southern IllinoisCatheterization of BladderREASONS TO INSERT:1. Bladder distension (pain)2. Incontinence (care giver unable or unwilling to keep patient clean and dry)3. Decubitus or skin issue irritated by urine4. Enlarged prostate glandALLERGIES:Check patient for any allergies, especially any allergies to providine-iodine (betadine), tape, adhesives,latex, lubricant, and shellfish.SUPPLIES:1. Insertion kit with extra gloves (sterile and non-sterile) in your size2. Water proof pads3. Drainage bag or leg bag with leg strap4. Irrigation kit5. Normal Saline or Sterile Water for irrigation6. Towel and wash cloths7. Catheter—Female size 14-16 Male size 16-18 (or specific size ordered by MD), may want toconsider Coude Catheter on male patients with prostate issues. Coude means bend or elbow and isdesigned for patients with enlarged prostate glands.8. A trash receptacle for used supplies and a clean bedside table or a clean place for supplies to bearranged.IMPLEMENTATION:FEMALE PATIENT PROCEDURE:1. Identify patient.2. Gather supplies. Perform hand hygiene.3. Explain procedure to patient and/or family.4. Allow for privacy.5. Raise bed to appropriate working height.6. If right handed, approach from the patient’s right side (or opposite if left handed).7. Position patient by assisting her to supine position with knees flexed. Ask patient to relax thighs, soshe can externally rotate the hip joint. Patient may require to be positioned in side lying (Sims)position with upper leg flexed at knee and hip if unable or unwilling to be in supine position. If thisposition is used, take extra precautions to cover rectal area with drape during procedure to reducechance of cross contamination.8. Prepare for procedure. Drape patient with bath blanket or sheet. Apply disposable gloves and wash perineal area with soap and water as needed; dry area anddispose of gloves. Position lamp or flashlight to illuminate area (if using a flashlight, someone should hold it.) Perform hand hygiene. Before inserting an indwelling catheter, open the package containing drainage bag (unless itcomes pre-attached to catheter) and place drainage bag in easily accessible location. Makesure drainage port is closed.Effective 3/2018, Reviewed 1/2019Page 1 of 6
Hospice of Southern Illinois Open catheterization kit. Place catheterization kit tray on clean, accessible surface such as abedside table or, if possible, between patient’s open legs. Patient size, level of cooperationand positioning will dictate exact placement. Perform hand hygiene. Apply sterile gloves. Organize supplies on sterile field. Drape perineum keeping gloves sterile. Open lubricant packet. Remove inner cover from Foley catheter and apply lubricant 1-2inches up catheter. At this time also open your betadine swabs. NOTE: It is no longer recommended to pretest a balloon by injecting fluid from prefilledsterile water syringe. Testing balloon may stretch it out and lead to increased trauma oninsertion.9. Clean Urethral Meatus Separate labia with fingers of non-dominant hand (now contaminated) to fully exposeurethral meatus. Maintain position of non-dominant hand throughout procedure. Holding betadine swab, clean labia and urinary meatus from clitoris toward anus. Use a newswab for each area that you clean. Clean by wiping far labial fold, near labial fold, anddirectly over center of urethral meatus. Pick up catheter 3-4 inches from tip. If catheter is not attached to drainage bag, make sure toposition urine tray so the end of the catheter can be placed there once insertion is completedand urine flow begins.10. Insert Catheter Ask patient to bear down gently and slowly. Insert catheter through urethral meatus. Advance catheter 2-3 inches or until urine flows out of catheter. Once urine appears, advancecatheter another 1-2 inches. Do not use force to insert catheter. NOTE: If no urine appears, catheter may be in vagina. If misplaced, leave catheter in vaginaas a landmark indicating where not to insert and then insert another sterile catheter. Release labia and hold catheter securely with non-dominant hand. Inflate catheter balloon with amount of fluid designated by manufacturer. Slowly inject totalamount of fluid. NOTE: It is recommended to fill a 3 cc balloon with 5 cc of sterile water and a 30 cc balloonwith 35 cc of sterile water. Improperly inflated balloons may cause drainage and deflationdifficulties. Using fluids other than sterile water may cause the balloon not to emptyproperly, especially after long dwell times. After inflating the catheter balloon, release the catheter from non-dominant hand. Gently pullcatheter until resistance is felt. Then advance catheter slightly. Connect drainage tubing to catheter if not already pre-connected. Secure indwelling catheter with a catheter strap or other securement device. Leave enoughslack to allow for leg movement. Attach securement device at tubing just above catheterbifurcation (inflation and deflation port.) Clip drainage tubing to edge of mattress. Position drainage bag lower than the bladder byattaching to the bed frame. Do not attach to bedrail. Provide hygiene as needed for the patient. Help patient to a comfortable position. Dispose ofsoiled supplies in appropriate receptacles. Measure urine and record. Remove gloves andperform hand hygiene. It is essential that you document the size of catheter inserted and theamount of water used to inflate the balloon in patient’s electronic medical record.Effective 3/2018, Reviewed 1/2019Page 2 of 6
Hospice of Southern IllinoisMALE PATIENT PROCEDURE:1. Identify patient.2. Gather Supplies. Perform hand hygiene.3. Explain procedure to patient and family.4. Allow for privacy.5. Raise bed to appropriate working height.6. If right handed, approach from the patient’s right side (or opposite if left handed).7. Position patient by assisting him to supine position with thighs slightly abducted.8. Prepare for procedure. Drape patient with bath blanket or sheet. Apply disposable gloves and wash perineal area with soap and water as needed; dry area anddispose of gloves. Position lamp or flashlight to illuminate area (if using a flashlight, someone should hold it.) Perform hand hygiene. Before inserting an indwelling catheter, open the package containing drainage bag (unless itcomes pre-attached to catheter) and place drainage bag in easily accessible location. Makesure drainage port is closed. Open catheterization kit. Place catheterization kit tray on clean, accessible surface such as abedside table or, if possible, between patient’s open legs. Patient size, level of cooperationand positioning will dictate exact placement. Perform hand hygiene. Apply sterile gloves. Organize supplies on sterile field. Drape perineum keeping gloves sterile. You may also use a fenestrated drape instead. Open lubricant packet. Remove inner cover from Foley catheter and apply lubricant 5-7inches up catheter. At this time also open your betadine swabs. NOTE: It is no longer recommended to pretest a balloon by injecting fluid from prefilledsterile water syringe. Testing balloon may stretch it out and lead to increased trauma oninsertion.9. Clean urethral meatus With non-dominant hand (now contaminated) retract foreskin (if uncircumcised) and gentlygrasp penis at shaft below glans. Hold shaft of penis at right angle to body. This handremains in this position for the remainder of the procedure. Using uncontaminated dominant hand, clean meatus with betadine swabs, using circularstrokes, beginning at meatus working outward in spiral motion. Repeat 3 times using clean swab each time. Pick up catheter 3-4 inches from tip. If catheter is not attached to drainage bag, make sure toposition urine tray so the end of the catheter can be placed there once insertion is completedand urine flow begins.10. Insert Catheter Lift penis to position perpendicular (90 degree angle) to body and apply gentle upwardtraction. Ask patient to bear down as if to void and slowly insert catheter through urethral meatus. Advance catheter 7-9 inches or until urine flows out of the end of the catheter. When urine appears in an indwelling catheter, advance it to the bifurcation. This ensures thatthe balloon portion of the catheter is not still in the prostatic urethra.Effective 3/2018, Reviewed 1/2019Page 3 of 6
Hospice of Southern Illinois Inflate the catheter balloon with amount of fluid designated by manufacturer. Slowly injecttotal amount of fluid.NOTE: It is recommended to fill a 3 cc balloon with 5 cc of sterile water and a 30 cc balloonwith 35 cc of sterile water. Improperly inflated balloons may cause drainage and deflationdifficulties. Using fluids other than sterile water may cause the balloon not to emptyproperly, especially after long dwell times.After inflating catheter balloon, release catheter from non-dominant hand. Gently pullcatheter until resistance is felt. Then advance catheter slightly.Connect drainage tubing to catheter if not already pre-connected.Secure indwelling catheter with catheter strap or other securement device. Leave enoughslack to allow leg movement. Attach securement device at tubing just above catheterbifurcation.Clip drainage tubing to edge of mattress. Position drainage bag lower than the bladder byattaching to the bed frame. Do not attach to bedrail.Provide hygiene as needed for the patient. Help patient to a comfortable position. Dispose ofsoiled supplies in appropriate receptacles. Measure urine and record. Remove gloves andperform hand hygiene. It is essential that you document the size of catheter inserted and theamount of water used to inflate the balloon in patient’s electronic medical record.IRRIGATION OF INDWELLING CATHETER:1. Identify patient.2. Gather supplies. Perform hand hygiene.3. Explain procedure to patient and/or family.4. Allow for privacy.5. Raise bed to appropriate working height.6. Apply gloves.7. Open irrigation tray. Pour approximately 60ml of the normal saline or sterile water into the solutioncontainer. The inside of the solution container and the tip of the piston syringe must remainsterile.8. Place the sterile piston syringe into the container and aspirate 30ml of the irrigation solution, leavingthe syringe in the container until ready to use.9. Position the drape under the catheter.10. Wipe the connection point between the catheter and drainage tubing with an alcohol pad beforedisconnecting.11. Disconnect the catheter from the drainage tubing, preventing the drainage tubing from becomingcontaminated.12. Insert the tip of the syringe into the lumen of the catheter and gently push the plunger to instill thesolution. **Never force the plunger or use suction**13. Remove the syringe while keeping the open end of the catheter pinched closed.14. Place the catheter into the collection basin and allow solution to drain. Amount of drainage solution should be equal to or greater than the amount instilled.15. After irrigation is complete, clean the end of the drainage tubing with an alcohol wipe and reinsertinto the lumen of the catheter.16. Dispose of soiled supplies in appropriate receptacles. Remove gloves and perform hand hygiene.Effective 3/2018, Reviewed 1/2019Page 4 of 6
Hospice of Southern IllinoisCARE AND REMOVAL OF AN INDWELLING CATHETER:Providing regular perineal hygiene, preventing catheter-related trauma, and removing indwelling cathetersas soon as possible are important interventions to reduce the risk of catheter-associated urinary tractinfections.When removing an indwelling catheter, it is important to ensure that the catheter balloon is fully deflated tominimize trauma to the urethra.PROCEDURE FOR REMOVAL:1. Gather Supplies as follows: Clean gloves Water proof pads Bath blanket Soap Wash cloth Towel Basin filled with warm water 10 mL or larger syringe without needle (Information on balloon size is printed directly on theballoon inflation valve.)2. Explain procedure to the patient and/or family.3. Place water proof pad under patient and drape for privacy. Gently insert the syringe into the ballooninflation port. Allow the pressure within the balloon to force the plunger back and fill the syringewith water. If the balloon does not deflate, reposition the patient. Ensure that urine flows freely.Attempt to deflate the balloon by using very gentle and slow aspiration. Aspiration that is too rapidor forceful may cause the inflation lumen within the Foley catheter to collapse. If all previousinterventions fail to deflate the balloon, the inflation port may be severed with scissors.4. Remove and discard old catheter and used supplies.5. Cleanse patient meatus and reinsert if indicated as directed above.6. Catheter changes are done PRN and according to facility protocol if patient resides in a facility.DOCUMENTATION CONSIDERATIONS**A Physician’s order is required to insert, irrigate, and discontinue a catheter** Insertion Type and size of catheter inserted Amount of fluid used to inflate balloon Characteristics of urine (color, odor, consistency, amount) Patient’s response to procedure Education provided to patient and/or family Irrigation Amount and type of solution used to irrigate Characteristics of drainage (color, odor, consistency, amount) Patient’s response to procedure Education provided to patient and/or family Removal Appearance of the catheter tip and balloon Appearance of perineal area Patient’s response to procedure Education provided to patient and/or familyEffective 3/2018, Reviewed 1/2019Page 5 of 6
Hospice of Southern IllinoisReferencesHeuristic. (n.d.) In Bard Medical Division’s online Bard foley catheter inflation/deflation guidelines.Retrieved oley%20Catheter%20Inflation Deflation%20Guidelines.pdfHeuristic. (2003) In University of Ottawa’s urinary catheter insertion guidance. Retrieved ristic. (n.d.) In University of Colorado Denver’s Sample policy and procedure inserting, removal, andcare of an indwelling foley catheter. Retrieved ts/Sample%20Policy%20and%20Procedures.pdfPerry, A. G., Potter, P. A., & Ostendorf, W. R. (2014). Urinary elimination. Clinical nursing skill andtechniques (8th edition). (pp 809-839). St Louis, MO: Elsevier Mosby.Effective 3/2018, Reviewed 1/2019Page 6 of 6
Hospice of Southern IllinoisGastrostomy and Jejunostomy TubesFeeding tubes can be placed directly into the gastrointestinal (GI) tract through the abdominalwall in patients who cannot tolerate nasogastric feeding tubes or require long-term enteralnutrition. The most common sites for long-term feeding tubes are the stomach (for gastrostomytubes) and the jejunum (for jejunostomy tubes). Initial insertion of long-term tubes requiresendoscopic, radiologic, or surgical placement.Feedings delivered via a gastrostomy tube are relatively safe to administer, provided the patienthas normal gastric emptying. Gastrostomy tubes are often called G tubes, but they are alsocommonly referred to as percutaneous endoscopic gastrostomy (PEG) tubes, a term used todescribe tubes placed endoscopically. Gastrostomy tubes range in size from 16 Fr to 28 Fr andexit through an incision in the abdomen, where an internal bumper or balloon and an externalbumper or disk holds the tube in place.Jejunostomy tubes are indicated when the risk of regurgitation and aspiration is especially high,as in cases of severely delayed gastric emptying or conditions such as pancreatitis that limit theuse of the stomach for feeding. Jejunostomy tubes can be placed directly into the small intestinein a surgical procedure or threaded through the stomach into the jejunum under fluoroscopy.Enteral nutrition, or tube feeding, is a method for providing nutrients to patients who are not ableto meet their nutritional requirements orally. As a rule, candidates for enteral nutrition must havea sufficiently functional GI tract to absorb nutrients. Examples of indications for enteral feedinginclude the following: Situations in which normal eating is not safe because of high risk for aspiration: Alteredmental status, swallowing disorders, impaired gag reflux, dependence on mechanicalventilation, certain esophageal conditions (strictures, or dysmotility), and delayed gastricemptying.Effective 3/2019Page 1 of 13
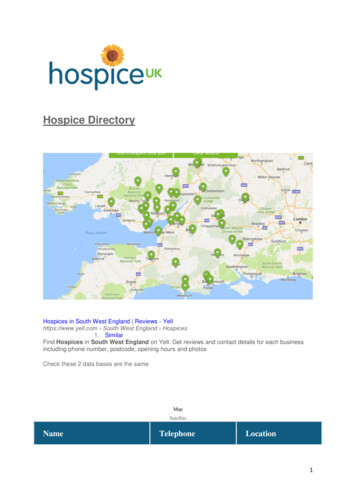
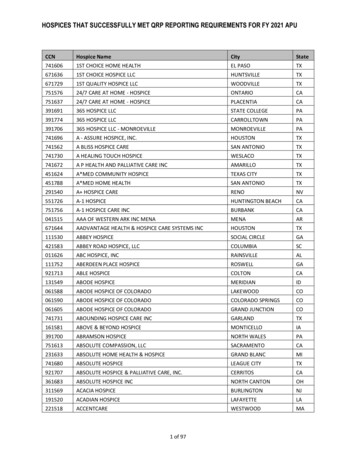
Hospice of Southern Illinois Clinical conditions that interfere with normal ingestion or absorption of nutrients orcreate hypermetabolic states: Surgical resection of oropharynx, proximal intestinalobstruction or fistula, pancreatitis, burns, and severe pressure ulcers.Conditions in which disease or treatment-related symptoms reduce oral intake: Anorexia,nausea, pain, fatigue, shortness of breath, or depression.Gastric feedings are the most common type of enteral nutrition, allowing tube-feeding formulasto enter the stomach and then pass gradually through the intestinal tract to ensure absorption. Incontrast, small bowel feeding occurs beyond the pyloric sphincter of the stomach, whichtheoretically reduces the risk for pulmonary aspiration, provided that feedings do not reflux backinto the stomach.The methods of administering enteral feedings include continuous, bolus, or a combination ofboth. The safest and most appropriate method is selected following an individual assessment ofthe patient. Continuous enteral feedings allow a slow hourly rate which may aid in feedtolerance, is less labor-intensive, and allows overnight feeding. However, this method requiresthe patient to be attached to a pump for long periods of time which may restrict mobility/activityand quality of life and requires some technical ability. Bolus enteral feedings mimic a normalpattern of eating, allows for greater mobility/activity as the patient is not attached to a pump forlong periods of time, allows greater flexibility for the patient with regards to when the feeding isadministered, and requires less equipment. However, with this method, patients may not toleratelarge bolus sizes and patients/caregivers with poor grip strength may struggle to push down theplunger or hold the syringe for the time required to administer the feeding.Gastrostomy tube with internalbumperGastrostomy tube with internalballoonEffective 3/2019Page 2 of 13
Hospice of Southern IllinoisCARE OF TUBE EXIT SITE:**The determination of whether the exit site is left open to air or a dressing is to be used isbased on the assessment of the site and the patient’s wishes**1. Gather supplies: Disposable gloves (3-4 pair) Disposable bag 4x4 gauze Protective skin barrier, if ordered. Antimicrobial agent, if ordered. Cotton-tipped applicator, if needed. Drain-gauze dressing Tape2. Perform hand hygiene.3. Explain procedure to patient and apply disposable gloves.4. If applicable, remove old dressing. Fold dressing with drainage contained inside; removegloves inside out over dressing. Discard dressing in disposable bag.5. Perform hand hygiene and apply disposable gloves. Clean skin around site with warmwater and mild soap or saline, using 4x4 gauze.6. Dry site completely with clean, dry 4x4 gauze.7. Remove gloves and perform hand hygiene.8. Apply disposable gloves.9. Apply protective skin barrier or antimicrobial agent, if ordered, using a cotton-tippedapplicator.10. If dressing is ordered, place a drain-gauze dressing over external bar or disc.NOTE: Do not place dressing under external bar or disc; this can cause gastric tissueerosion or internal abdominal wall pressure.11. Secure dressing with tape.12. Remove gloves and dispose of supplies in appropriate receptacle. Perform hand hygiene.DOCUMENTATION CONSIDERATIONS:**A Physician’s order must be obtained for a treatment to a tube exit site** Appearance of site (signs of infection, excoriation, drainage, bleeding)Dressing and/or ointments appliedPatient’s tolerance to procedureEducation provided to patient and/or familyEffective 3/2019Page 3 of 13
Hospice of Southern IllinoisADMINISTERING MEDICATIONS, VERIFYING PLACEMENT, AND IRRIGATING AFEEDING TUBE:Preferably medications administered by enteral tubes should be in liquid form. If a medication isnot available in liquid form, you will need to prepare an oral medication tablet or capsule bycrushing or dissolving it. However, you cannot crush sublingual, sustained-release, chewable,long-acting, or enteric-coated medications. Consult with a pharmacist about whether you cancrush or dissolve (including gel capsules) a medication and to determine if any medicationsinteract with the enteral feeding. If interaction occurs, hold tube feeding 30 minutes before andafter medication administration.Irrigate tube routinely before, between, and after final medication and before and after anintermittent feeding is administered.1. Gather supplies: Disposable gloves 60ml catheter-tipped syringe (or Luer-Lok tip, if applicable) Graduated container Tap water Medication to be administered Tongue blade or straw to stir dissolved medications (if needed) Towel Stethoscope2. Perform hand hygiene.3. Prepare medications for instillation into feeding tube: Tablets: Crush each tablet into a fine powder, using a pill-crushing device or twospoons. Dissolve each tablet in a separate cup of 30ml of warm water. Capsules: Open capsule or pierce gel cap with a sterile needle and empty contentsinto 30ml of warm water. Gel caps do dissolve in warm water, but this may take15 to 20 minutes. Liquids: Always prepare liquids by placing the medication cup on a flat surfaceand fill to desired level, confirm accurate fluid amount by looking at the cup ateye level.4. Explain procedure to patient/caregiver.5. Elevate head of bed to minimum of 30 degrees, preferably 45 degrees (unlesscontraindicated) or sit patient up in a chair.6. If continuous enteral tube feeding is infusing, adjust infusion pump to hold tube feeding.7. Apply disposable gloves.8. Verify tube placement:a) Attach the 60ml syringe to end of tube. Aspirate gently back on the syringe toobtain gastric contents, observing color. Gastric contents are usually green, clear,Effective 3/2019Page 4 of 13
Hospice of Southern Illinoisand odorless. For small intestine tube placement, gastric contents appear yellow,yellow-brown, or greenish brown. Return aspirated contents into stomach unlessthe volume (Gastric Residual Volume) exceeds 500ml. When GRV is excessive,hold medications and tube feeding, then contact the physician or nursepractitioner. Large residuals indicate delayed gastric emptying and put the patientat increased risk for aspiration.AND/ORb) For Gastrostomy tubes, inject 30ml of air into the stomach and listen with thestethoscope for the “whoosh” of air into the stomach. The smaller diameter ofsome tubes makes it difficult to hear air entering the stomach.9. To irrigate tube: Draw up 30ml of water into the 60ml catheter-tipped syringe.10. Kink feeding tube while disconnecting it from the administration tubing or whileremoving plug at end of tube.11. Insert tip of syringe into the end of feeding tube. Release kink and slowly instill water.12. If unable to instill water, reposition patient on left side and try again.13. When water has been instilled, kink feeding tubing again, and remove syringe.*Some enteral tubes are connected to the continuous-feeding tubing with a stopcockapparatus that contains a medication port. Attach tip of syringe to the medication port onthe stopcock; turn “off” setting of stopcock away from the patient and toward infusiontubing. Flush tube and set stopcock “off’ again to medication port and remove syringe.*14. To administer medications: Remove plunger of syringe and reinsert syringe into tip offeeding tube.15. Administer first dose of liquid or dissolved medication by pouring into syringe. Allow toflow to gravity. If giving only one dose of medication, flush with 30ml of water afteradministration. To administer more than one medication, give each separately and flushbetween medications with 15 to 30ml of water. Follow last dose of medication with 30ml of water.16. Kink feeding tube, remove syringe, then reinsert administration tubing or if tube feedingis not being administered, insert cap to end of tube.17. Resume tube feeding (if applicable).18. Help patient to a comfortable position and encourage to keep head of bed elevated forone hour.19. Remove and discard gloves; dispose of soiled supplies in appropriate receptacle. Rinsegraduated container and syringe with tap water.20. Perform hand hygiene.Effective 3/2019Page 5 of 13
Hospice of Southern IllinoisDOCUMENTATION CONSIDERATIONS:**All medication orders must indicate the route as “per tube”** Method used to check placement of tube. If applicable, document residual amount.Medications and time of medications administered.Record time of irrigation and amount of fluid instilled.Patency of tube.Patient’s response to procedure.Education provided to patient and/or caregiver.Effective 3/2019Page 6 of 13
Hospice of Southern IllinoisREPLACING A GASTROSTOMY TUBE:When a gastrostomy tube is inadvertently displaced, prompt replacement will help reduce thepotential for the tract to close. When reinserting a gastrostomy tube, it is very important to knowif the tract is adequately established. At least 4 to 6 weeks is necessary for a tract to becomeestablished. Until the tract has been established, it is recommended that a physician change thetube. In some cases, if possible, the physician who inserted the tube may be the one who willchange the tube initially. Prior to any G-tube change, collaborate with Hospice of SouthernIllinois’ Medical Director to decide whether the nurse will be replacing the tube. A physician’sorder to replace the tube must be obtained. NOTE: Replacing a gastrostomy tube may beperformed only by an RN.1. Gather supplies: Appropriate size and type of replacement tube Disposable gloves (2 pair) Towel 4x4 gauze pads Water soluble lubricant 10cc luer lock syringe 10cc luer lock syringe filled with 10cc water/saline 60 ml catheter-tipped syringe Graduated container Tape or G Tube anchor device2. Perform hand hygiene.3. Explain procedure to patient.4. Apply disposable gloves.5. Assist the patient to lie down in a comfortable position. Drape a towel over patient’sabdomen, exposing only the tube site.6. NOTE: Some tubes have a bumper type device to internally secure and do not requireStep 7. Be certain of the type of tube before performing Step 7. There are different typesof bumpers-internal and external. Some internal bumpers are collapsible/deflatable,others are hard and fixed. Some devices can be removed at bedside, but others mayrequire the physician to remove.7. If applicable, remove the balloon type tube: Deflate the balloon by inserting a Luer-lock syringe into the balloon port of theexisting tube. Once the fluid is removed from the balloon. Gently twist and rotate the tube toassess if it will come out. Remove the existing tube.Effective 3/2019Page 7 of 13
Hospice of Southern Illinois8. Once the tube has been removed, clean the peristomal area with soap and water, using aspiral pattern beginning at the stoma and moving outward. Rinse and pat dry.9. Remove disposable gloves, perform hand hygiene, and then apply clean disposablegloves.10. Make sure the balloon is intact to the new tube by instilling 2-3 ml of water or air into theballoon. Check the balloon for leaks, and then remove the water or air.11. Lubricate the end of the gastrostomy tube with a water soluble lubricant. DO NOT USEpetroleum-based lubricant.12. Insert the deflated balloon end of the gastrostomy tube into the ostomy site using a slighttwisting motion about 2-3 inches and stop. Minimal bleeding during a tube change isinsignificant.13. Inflate the balloon with 10cc’s (or physician specified amount) of water/saline and detachthe syringe. NEVER use air to inflate the balloon.14. Slowly and gently pull the gastrostomy tube until resistance is met.15. Aspirate stomach contents with a 60ml catheter-tipped syringe to assess placement. Reinstill the aspirate to prevent electrolyte imbalance.16. Flush the gastrostomy tube with 30-50ml of tap water.17. Clamp or plug the gastrostomy tube before it is completely empty to prevent air fromentering the stomach.18. Secure the tube to patient’s abdomen.19. Remove gloves and perform hand hygiene. Discard soiled supplies in appropriatereceptacle.DOCUMENTATION CONSIDERATIONS:**A Physician’s order must be obtained to replace a gastrostomy tube** If applicable, the condition of the tube removedType and size of replacement tube, as well as the amount of water instilled into balloonVerification of placementThe amount of water flushedCondition of skin at tube siteThe patient’s tolerance to the procedureEducation provided to patient and/or caregiverEffective 3/2019Page 8 of 13
Hospice of Southern IllinoisADMINISTERING ENTERAL NUTRITION:1. Gather supplies: Disposable gloves 60ml catheter-tipped syringe Towel Prescribed type and amount of feeding Tap water for flushing Graduated container Bolus administ
Pick up catheter 3-4 inches from tip. If catheter is not attached to drainage bag, make sure to position urine tray so the end of the catheter can be placed there once insertion is completed and urine flow begins. 10. Insert Catheter Ask patient to bear down gently and slowly. Insert catheter through urethral meatus.