Transcription
IVUS Findings in DESRestenosisGary S. Mintz, MDCardiovascular Research FoundationNew York, NY
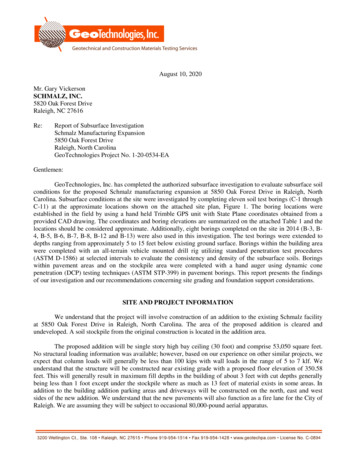
Stent Underexpansion
The 90% predictive value for underexpansion as a cause ofCypher stent restenosis in SIRIUS suggested that mostcauses of Cypher stent failure will be “mechanical”Bare Metal StentsCypher6.5*Minimum stent area 30201008.08.510090807060504030201007.07.5F/U MLA 4.0mm2 (%)3.54.04.55.05.56.0F/U MLA 4.0mm2 (%)sensitivityspecificity5.0**Minimum stent area (mm2)*predictive value 56%(Sonoda et al. J Am Coll Cardiol 2004;43:1959-63)**predictive value 90%
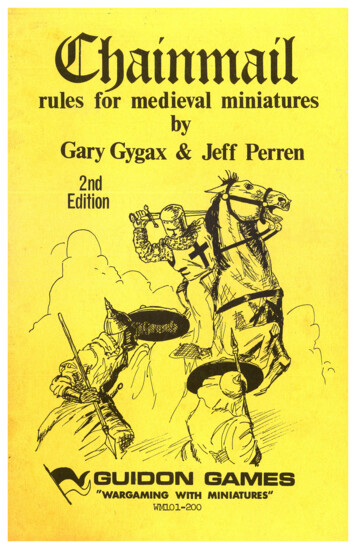
Predictors of angiographic restenosis in 550patients with 670 native artery lesionstreated with Cypher stentsAngiographic restenosis (%)Angiographic restenosis (%)1001008080606040402020003.5 4.0 4.5 5.0 5.5 6.0 6.5 7.0 7.510 15 20 25 30 35 40 45 55 60 65 70 75IVUS MSA (mm2)IVUS total stent length (mm)(Hong et al. Eur Heart J 2006;27:1305-10) 5.5mm2 5.5mm2 40mm2.4%0.4% 40mm17.7%8.6%
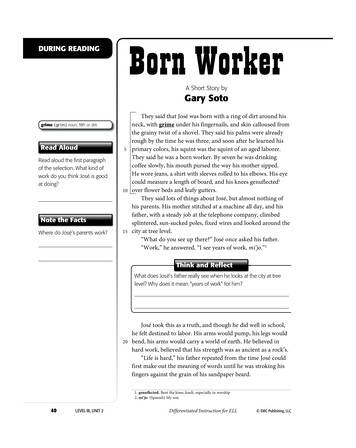
Post-Procedure MSA and Binary Restenosisat 9-Months: TAXUS IV, V, and VI100Sensitivity (%)806040Specificity (%)2000246810121416Minimum Stent Area (MSA, mm2)MSA 5.5 mm294% Neg. Predictive Value
While each of these studies reported asingle MSA that best discriminatedrestenosis from no restenosis, therewas still a stepwise relationshipbetween a larger MSA and a lower rateof DES restenosis.
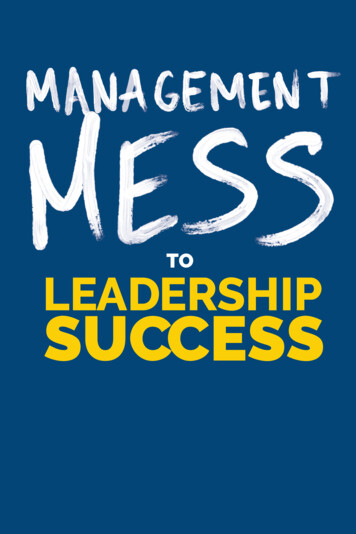
IVUS Measured MSD (mm)IVUS Measured MSA (mm2)Comparison of IVUS-measured minimum stent diameter(MSD) and minimum stent area (MSA) with the predictedmeasurements from Cordis (Cypher in yellow, n 133) andBSC (Taxus in red, n 67). DES achieve an average of only75% of the predicted MSD (66% of MSA)1412108642054321002468101214Predicted MSA (mm2)(de Rebamar Costa et al, Am Heart J 2007;153:297-303)01234Predicted MSD (mm)5
Failure of Cypher Stent Treatment ofIn-stent Restenosis @ CRF Recurrence in 10 of 41 patients with in-stent restenosis treated with Cypher stents Stent underexpansion (MSA 5.0mm2) in 8/10 recurrence instent restenosis lesions (80% vs 12/38 [38%] of non-recurrentlesions, p 0.02) and 6/10 (60%) recurrent lesions had a MSA 4.0mm2 vs 8/38 (18%) non-recurrent lesions (p 0.02) Gap between multiple Cypher stents was detected in 3/10recurrent lesions: vs 1/38 non-recurrent lesion (p 0.005). Thegap was not detectable angiographically, and it measured 1mm in length by IVUS.Therefore, complete lesion coverage and adequate stentexpansion are important in the DES treatment of ISR.(Fujii et al. Circulation 2004;109:1085-1088)
Serial IVUS Findings after CypherStent Treatment of BMS Restenosismm2252015P 0.0001P 0.000110P 0.0001P 0.000150% of lesions withMLA 4.0mm2 postPCI decreasing to 4.0mm2 at F/U(Sakurai et al. Am Heart J, in press)
“Uncovered” (Residual) EdgeStenoses
IVUS Predictors of Stent Edge Restenosis in SIRIUSBaseline ParametersPeri-stentStenosisNo PeristentStenosispReference MLA (mm2)4.7 2.36.5 2.30.06Reference Residual Plaque (%)60.5 9.049.1 11.50.03Edge SA / Reference MLA1.5 0.31.2 0.30.03Maximum Pressure (mm)15.4 3.216.9 2.7nsBalloon / Artery Ratio0.9 0.11.0 0.1ns(Sakurai et al. Am J Cardiol 2005;96:1251-3)
Plaque Prolapse
Intra-stent acute plaque prolapse in theDIABETES-I and DIABETES-II TrialsCypherTaxusNPlaqueprolapse9No plaqueprolapse60Plaqueprolapse15No plaqueprolapse65Mean 77mm21.71mm21.49mm2Restenosis03.3%6.3%7.3%Stent thrombosis0000F/UP 0.05(Futamatsu et al. J Am Coll Cardiol 2006;48:1139-45)
Acute Stent Malapposition
Acute Incomplete Cypher Apposition @ CRFPersistent ISA (n 40, 83% decreased in size)2520Baseline CSACompletely resolved ISA (n 15)(mm2)p NS2CSA (mm2)p 0.01p 0.091.515p NSp NS10p NS51p NS0.5p 0.002p NS00EEMStentLumenP&MISA The only independentpredictor of persistent ISA wasthe amount of superficiallesion calcium ISA correlated with P&M,but not with EEM-0.5 EEM Lumen P&MISAIH*Max IH-1-1.5-2p 0.006p 0.0001*at malapposition site(Kimura, et al. Am J Cardiol 2006;98:436-42)
Acute Incomplete DES Apposition @ AMC 51/705 (7.2%) lesions (7.2%) 47/705 in sirolimus-eluting stents 4/167 in paclitaxel-eluting stents. Malappostion was persistent in all 51lesions at 6-month F-U with no TLR orMACE eventsCSA (mm2) p 0.00120PostF/U15p NS10p 0.001p 0.0015p NS0EEMStent(Hong et al. Circulation 2006;113:414-9)P&MIntra-stentLumenIHISA
Strut Fracture and InhomogeneousStrut Distribution
01.56.0mm
However. . . Most suspected cases of strut fracturedid not have baseline and follow-upIVUS Most suspected or documented casesof strut fracture did not result inrestenosis or other complications Strut fracture has only been found in asmall minority of DES restenosis orthrombosis cases
When compared to either neointima-free sections in thesame stent or non-restenotic stents, the maximum IH areacorrelated with fewer stent struts and with a larger anglebetween adjacent stent struts.bacdefIndependent predictorsof IH CSA, IH thickness,and MLAabcdef EEM CSA (p 0.05) P&M CSA (p 0.05) Normalized # of struts (p 0.0001) Maximum interstrut angle (p 0.0001)(Takebayashi et al. Circulation. 2004;109:1244-9)
02.510.0mm
Conclusions The most important IVUS findings in patientswith DES restenosis continue to be stentunderexpansion and inflow/outflow stenoses Other findings include stent strut fractureand inhomogeneous stent strut distribution. All cases of DES failure deserve IVUSinterrogation.
Title: Microsoft PowerPoint - 1.Gary Mintz Author: HP_Owner Created Date: 6/14/2007 9:26:25 AM