Transcription
Volume 34Issue 3Article 16-29-2021Undertaking the surgical count: An observational studyVictoria Ruth Warwick DrFiona Stanley and Fremantle Hospital Group, vicky.warwick@health.wa.gov.auBrigid M. Gillespie ProfessorGriffith University - Australia, b.gillespie@griffith.edu.auAnne McMurray ProfessorGriffith University, School of Nursing, a.mcmurray@griffith.edu.auKaren G. Clark-Burg ProfessorThe University of Notre Dame Australia, karen.clark-burg@nd.edu.auFollow this and additional works at: https://www.journal.acorn.org.au/jpnPart of the Health Services Administration Commons, Health Services Research Commons,Perioperative, Operating Room and Surgical Nursing Commons, and the Surgery CommonsThis work is licensed under a Creative Commons Attribution 4.0 License.Recommended CitationWarwick, Victoria Ruth Dr; Gillespie, Brigid M. Professor; McMurray, Anne Professor; and Clark-Burg, KarenG. Professor (2021) "Undertaking the surgical count: An observational study," Journal of PerioperativeNursing: Vol. 34 : Iss. 3 , Article 1.Available at: .journal.acorn.org.au/jpn/vol34/iss3/1This Article is brought to you for free and open access by Journal of Perioperative Nursing. It has been acceptedfor inclusion in Journal of Perioperative Nursing by an authorized editor of Journal of Perioperative Nursing.
Peer-reviewed articleAuthorsDr Victoria Ruth WarwickDrN, RNPerioperative Nurse Unit Manager, FionaStanley Hospital and Fremantle HospitalGroup, Perth, Western AustraliaProfessor Brigid M GillespiePhD, RN, FACORNProfessor of Patient Safety, School ofNursing and Midwifery, Griffith Universityand Gold Coast University Hospital, GoldCoast Health, Nursing and MidwiferyEducation and Research UnitProfessor Anne McMurrayAM, PhD, RN, FACNEmeritus Professor, School of Nursing andMidwiferyPrinciple Research Fellow, IntegratedCare Program, Centre for Applied HealthEconomics, Menzies Health InstituteQueensland, Griffith University, Gold CoastCampusProfessor Karen G Clark-BurgPhD, MBA (Exec), RNDean School of Nursing and Midwifery,The University of Notre Dame AustraliaCorresponding authorDr Victoria Ruth WarwickDrN, RNPerioperative Nurse Unit Manager, FionaStanley Hospital and Fremantle HospitalGroup, Perth, Western AustraliaVicky.warwick@health.wa.gov.auUndertaking the surgical count:An observational studyAbstractObjectiveTo systematically measure and describe perioperative nurses’ surgical countpractices using the Surgical Count Observational Tool, to measure conformitywith standardised processes and identify barriers and enablers influencingnurses’ practices.Sample and settingA large public tertiary hospital in Western Australia.MethodsThe Surgical Count Observational Tool (SCOT) was developed using the ContentValidity Index over two Delphi panel rounds and then pilot tested. Individualobservations were analysed according to 14 criteria based on the 2016Australian College of Perioperative Nurses (ACORN) standard ‘Managementof accountable items used during surgery and procedures’1. Count processeswere observed over two consecutive weeks across six specialist perioperativeteams including nurses, surgeons, anaesthetists and technicians to measurecompliance with the ACORN standard. The SCOT and a field diary were thenused in an observational study of 83 nursing staff, including 54 circulatingnurses and 29 instrument nurses, over a period of 57 hours. Interrater reliabilitywas calculated using Cohen’s kappa. Descriptive statistics were used to analyseobservational data.ResultsOf the 1268 count practices observed, 759 were compliant with the ACORNstandard, representing a 60 per cent compliance rate.ConclusionConsistency and compliance rates were lower than expected. Patient,case, environmental factors and expectations of surgeons and co-workerswere observed to act as barriers to best practice in perioperative nursesundertaking a surgical count, while nurse’s knowledge was observed to act asan enabler.Keywords: surgical count, perioperative, structured observations, best practice,patient safety, standardJournal of Perioperative Nursing Volume 34 Number 2 Spring 2021 acorn.org.aue-3
Table 1: Components of observational tool (based on the 2016 ACORN accountable items standard1)ComponentnumberComponentNumber ofbehaviouralindicatorsDescriptor1Count processThe recommended steps or actions required to undertake a count.252No count requiredNo accountable items used during procedure as the proceduredoes not involve opening a body cavity or making an incision.23Accountable itemsremoved from ORItems that are part of the count process remain in the OR for theduration of the procedure.54Absorbable gauzeswabs, wool balls,pharyngeal packsutilisedAccountable items that may not have an x-ray identifiable stripbut are used intra-operatively. These items are sometimes dividedand must be recorded on the count sheet.135Incorrect number ofitems in packageAccountable items come in a standardised number (for example,1, 5 and 10). When opening a package the right number of itemsshould be as stated on the package.76Count reliefA relieving nurse that undertakes a component of the count whenthe original staff member is not available, for example, during atea break.97SimultaneousproceduresTwo different procedures on the same patient that occur atthe same time. May be the same surgical team or two differentsurgical teams.58Sequentialprocedure. ORcleared/not clearedbetween proceduresDifferent procedures that occur on the same patient but atdifferent times. Same original sterile set up may or may not beused.149Intentionallyretained itemsAccountable items are left in or on the patient at the end of aprocedure, for example, packing of a cavity to be removed later.710Removal ofintentionallyretained itemsWhen a patient returns to OR to have accountable items removedthat were left in situ by necessity and were documented on theoriginal count sheet as being retained.211Tray listsPaper lists of instruments that accompany individual surgicaltrays.1512Progressive countingaway techniqueThe process followed to account for all accountable items, forexample, handing off packs from the sterile field and placing in acontainer in groups of five.913Emergency situationThe patient enters the OR and there is no time to undertake asurgical count due to a medical or surgical emergency.314Incorrect countThe original count tally for the procedure is not congruent withthe final count tally on completion of the procedure.8Total number of itemse-4124Journal of Perioperative Nursing Volume 34 Number 2 Spring 2021 acorn.org.au
BackgroundIn 2006, the Australian Commissionon Safety and Quality in HealthCare (ACSQHC) was establishedas part of an Australian initiativeto improve safety and quality inhealth care. The ACSQHC is jointlyfunded by each Australian state andterritory and one of its roles is toadvise on best practice and providerecommendations for nationallyagreed safety and quality standards.In 2002, health ministers endorsed atable of eight descriptors of sentinelevents that became reportable to theACSQHC. These were related to harm,serious harm or death that a patientsustained while under the care ofa health care facility (HCF)2. One ofthese sentinel events was retaineditems in surgery.In Western Australia during 2015and 2016, there were 434 reportableevents within HCFs, three of whichwere related to retained itemsin surgery3. The surveillance unitidentified contributing factors ascommunication, the environmentand practitioner knowledge, skill andcompetence. Failure to follow latestpolicy, procedure or guidelines wasseen as an important contributingfactor, an issue that has also beenidentified in the USA. The AmericanJoint Commission Sentinel EventAlert4 published a 10–15 per centerror rate in surgical count practices,which was attributed to failure tofollow policy and procedure. This isa significant issue, as it can increasethe likelihood of an unintentionallyretained item (URI).Rowlands and Steeves5 reviewof studies on incorrect surgicalprocesses found a significant riskof URIs in surgery due to failure tofollow current surgical count processand procedure. Their review includedstudies of possible causes of URIsin surgery but failed to identifycurrent barriers to and enablers ofperioperative nurses following bestpractice when undertaking a surgicalcount.The surgical count is a structured,standardised process developedby the Australian College ofPerioperative Nurses (ACORN) toassist nurses in maintaining bestpractice standards and ensuringpatients receive safe, high qualitynursing care6. Despite endorsementby peak national and internationalperioperative bodies, variations inclinical practice continue to occur.This study aimed to systematicallyexamine perioperative nurses’surgical count practices in one majorAustralian hospital.ObjectiveThe aim of this prospectiveobservational study was todescribe current surgical countpractices of perioperative teamsand calculate overall compliancewith the relevant ACORN practicestandard using a specially developedobservational tool – the SurgicalCount Observational Tool (SCOT).This tool was developed usingbehavioural performance markersthat reflected the count process asrecommended in the 2016 version ofthe ACORN standard ‘Managementof accountable items used duringsurgery and procedures’ (theACORN accountable items standard).Subsumed under the overarching aimwere the following two objectives:1. to develop a tool based onthe ACORN accountable itemsstandardTable 2: Feedback from Delphi participantsRound 1 feedbackRound 2 feedbackDescriptorsLack of clarityAdd a word to increase clarityUnclear sentence structureItems listed may vary acrosssitesParticular item may not be the same at any givensite, for example, surgeon signing the count sheetIrrelevant itemThe relevance of the item listed was unclearDefinition of some wordsunclearLack of understanding about what was being askedRepetition of itemsAmbiguous because the itemis very similar to another itemRepetition of itemsSomewhat unclear aboutwhat is being askedUnsure of what the category is forDid not respond to itemGiving a mark of 1 or 2 but provided no feedback asto reason whyJournal of Perioperative Nursing Volume 34 Number 2 Spring 2021 acorn.org.aue-5
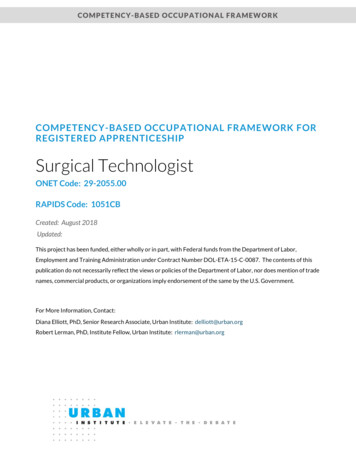
The study also aimed to identifybarriers and enablers influencingnurses’ practices.Literature reviewEthicsEthics approval was granted throughthe university and participatinghospital’s ethics approval processes.Information about the study wasgiven to participants who providedtheir informed consent. Researchintegrity was maintained throughjoint planning and discussions bythe research team. Feedback aboutthe data analysis was providedto participants during in-servicesessions at the participating hospitalprior to writing the final report andthis provided opportunities to clarifyor modify findings prior to the finalreport being written.Observational tooldevelopmentThe observational tool contained 14components of the count process(see Table 1), each consisting ofe-68089%85%64%64%36%36%604015%20The literature reviewed for thisstudy provided information aboutthe surgical count process andconcluded that the perioperativenurse’s ability to undertake a surgicalcount was influenced by patientfactors, case factors, environmentalfactors including distraction andnoise within the operating room,and individual factors includingknowledge of policy development. Noempirical studies on the barriers andenablers in undertaking a surgicalcount were found.Methods100Percentage2. to systematically observeperioperative nurses’ compliancewith surgical count practicesrecommended in the ACORNaccountable items standard usingthe tool.0111%411Component numberAgreement12DisagreementFigure 1: Disagreement between raters following pilot studybehavioural indicators. These werebased on the standard ‘Managementof accountable items used duringsurgery procedures’1 which outlinesthe recommended actions thatshould be taken by the circulatingand instrument nurses whileundertaking a surgical count.Each behavioural indicator wasformatted with ‘Yes’, ‘No’ and ’N/A’(not applicable) tick boxes for easeof recording observed behaviours. Ininstances where the behaviour wasrequired as part of the count process‘yes’ was ticked if the behaviour hadbeen observed and ‘no’ if it was notobserved or undertaken as part ofthe process. The ‘N/A’ tick box wasused for any of the behaviours thatwere not required during the countprocess. For example, if there wereno intentionally retained items forthe case observed ‘N/A’ was tickedfor all the behaviours within thatcomponent.Content validationA Delphi study was undertakento test content validity using thecontent validity index (CVI)7. Tworounds of the Delphi panel occurredwith four out of the ten perioperativenurses who were invited to reviewthe observational tool respondingto the request and then providingfurther feedback on the revisedobservational tool. All respondershad at least 20 years perioperativeexperience, were aged 36 years orover and held a hospital certificate,diploma or a bachelor’s degree inhealth scienceIn the first round, responderswere requested to review theobservational tool by rating eachitem according to its relevance, with‘1’ being not at all relevant throughto ‘4’ being very relevant. Feedbackwas also encouraged about clarityof wording and flow of items as wellas the structure and layout of thedocument. The level of agreementfor the total CVI was 0.75 and 0.66in rounds one and two respectively,both considered acceptable levels7.Minor edits were made to theobservational tool in response toresponders’ comments (Table 2). Tomaintain the alignment with theACORN accountable items standard,individual items that may have variedacross hospital sites were maintainedJournal of Perioperative Nursing Volume 34 Number 2 Spring 2021 acorn.org.au
Table 3: Surgical case altimenumber of(minutes)nursesTotalnumberof teammembersSurgical specialtyOperative procedure2OrthopaedicsFractured clavicle753923OrthopaedicsTotal hemiarthroplasty653932OrthopaedicsTotal knee replacement1803641General surgeryChest abscess953752NeurosurgeryExcision tumour210376LANeurosurgeryGanglionectomy by radiofrequency502873NeurosurgeryBurr holes and insertion of shunt1553781TraumaRemoval of glass from foot603794TraumaProximal femoral nail11038102OrthopaedicsBilateral knee replacement12038112PlasticsMastectomy and axillary clearance16538123PlasticsMastectomy and axillary clearance11538133PlasticsExcision of multiple lesions1254814LAPlasticsExcision mucosal biopsy3025153General surgeryStaging laparoscopy4548163General surgeryIvor Lewis and thoracotomy410211171PlasticsMastectomy and DIEP (deep inferiorepigastric perforator artery) flap410512182General surgeryLaparoscopic cholecystectomy7536193General 1EmergencyLaparoscopic appendicectomy6038222EmergencyLaparoscopic appendicectomy8039234PlasticsExcision of multiple lesions503624LAPlasticsExcision of cheek lesion353425LAPlasticsExcision of multiple lesions10526262OrthopaedicsRevision hip replacement8039273TraumaOpen reduction and internal fixationfractured femur19039283General surgeryGastrojejunostomy225314Note: LA local anaesthetic.Journal of Perioperative Nursing Volume 34 Number 2 Spring 2021 acorn.org.aue-7
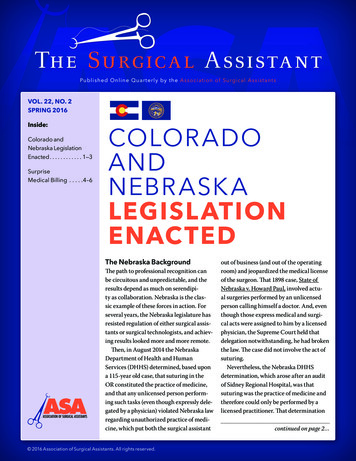
1002827282726Percentage of 0124010301062010021200 01.1011.2611.311.4011.51 11.611.70 01.8011.91 111.10 1.1176 6611 101012012171611 1120 011.12 1.13 1.14 1.15 1.16 1.17 1.18 1.19 1.20 1.21 1.22 1.23 1.24 1.25Item numberrecommended action was observedrecommended action was not observednot applicable1.1 An approved perioperative document(APD) was utilised1.11 Items remain in inner packaging forinitial count1.2 Two nurses perform the initial count1.12 Items remain as originally secured1.3 Both nurses count together1.13 Each accountable item is separated as itis being counted1.20 Instrument nurse notified surgeon1.14 Items checked for integrity1.22 Same two nurses finalise the count1.4 Both nurses count aloud1.5 Both nurses count items individually1.15 Items checked for x-ray detectablemarker1.6 Both nurses visualise all items1.7 Count recommenced if interrupted1.16 Dropped/contaminated items removedwith packaging if prior to commencementof initial count1.8 What type of interruption occurred?1.9 Only items required are opened1.18 Additional counts undertaken1.19 Surgeon notified of outcome of eachcount1.21 Circulating nurse notified surgeon1.23 APD signed appropriately by both nurses1.24 APD signed appropriately by surgeon1.25 OR cleared of all accountable items atconclusion of surgery1.17 Items added to the countintraoperatively are recorded on APD1.10 Items opened and counted as peroriginal packagingFigure 2: Compliance with recommended actions as observed for count process (component 1,behavioural indicators 1.1 to 1.25)and no items were deleted except forthose that were repetitive. Followingthe second Delphi review, the toolwas deemed ready for piloting.Pilot studySetting and sampleAt the time of the study, thepilot site had 300 beds and eightcommissioned operating rooms(ORs), performing over 460 electivesurgical cases per month acrossall specialties. Over 65 staff wereemployed in the OR facility includingregistered nurses, clinical nurses andanaesthetic technicians.Interrater reliabilityThe pilot study was conductedover three days and observationaldata collected by two perioperativee-8nurses – one was a researcher forthis study and the other a doctoralstudent. Twelve nurses wereobserved undertaking surgical countsfor six procedures over 7.7 hours (463minutes) of surgical time. Surgicaltime was recorded from when thepatient was brought into the OR,asleep or awake, to when they leftthe OR for the Post Anaesthesia CareUnit (PACU). Each procedure lasted 25to 150 minutes.Six procedures were required toachieve the minimum samplesize for interrater reliability8. Caseinformation relative to specialty,operative time, patient ASA (AmericanSociety of Anaesthesiologistsrisk grading for anaesthesia)and procedure was collected tocontextualise observations to betterexplain the results.Consistency of observersObservations included 744 individualbehavioural indicator items observedin relation to the count process forthe six surgical procedures. The tworaters used the observational toolspecifically designed for this study.ResultsThe two raters agreed on the countbehaviours that were observed andthose not observed for 726 of the744 observations. Cohen’s Kappareflected a high level of interrateragreement (K 0.85, p .0001).Figure 1 illustrates the interraterdisagreement across components 1, 4,11 and 12. All other items reflecteda 100% agreement and are notillustrated in the table.Journal of Perioperative Nursing Volume 34 Number 2 Spring 2021 acorn.org.au
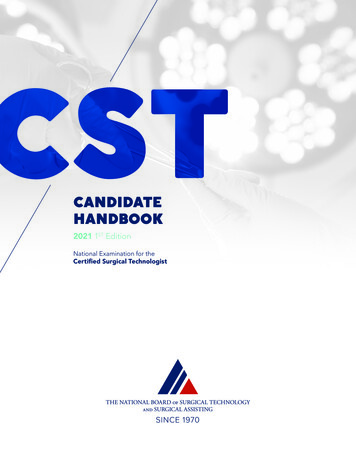
Main observationalstudySample and settingThe main study site was a largemetropolitan public tertiary hospitalwhich at the time of the study had13 commissioned operating theatreswith over 800 surgical proceduresbeing performed per month acrosselective, urgent and emergent cases.All specialties except obstetrics,neonates and paediatrics werecovered. The unit employed allcategories of perioperative staffincluding registered nurses, clinicalnurses and staff development nurses.Observations occurred over twoconsecutive weeks between 7.00am and 7.00 pm Monday to Friday.Count processes of nursing staffwere observed across six differentspecialties. Surgical time includedfrom when the patient arrived in theOR, awake or asleep, until they leftthe OR for the PACU.MethodThe observational tool was used tocollect relevant data in relation tothe count process. At the beginningof the tool there was an area todocument case information relativeto specialty, operative time, patientASA and procedure. This informationwas aimed at contextualising theobservations to better explain theobservations and determine otherfactors that may have influenced thecount process undertaken by thenurse. Information on the number ofstaff members involved in the casewas also collated as this could havean impact on the count process. Afield diary recorded notes, includingmannerisms, conversations andprocesses, to explain why items werenot observed and what may havehindered nurses’ ability to undertakethe count process. Structuredobservations allowed description ofcount behaviours.Data analysisCount processAbsolute (n) and relative (%) valueswere used to describe frequenciesof behavioural indicators observedusing the SCOT. Compliance ratesfor individual behavioural indicatorswere calculated as a percentageusing the formula 100n/d wheren is the number of cases in whichthe recommended behaviour wasobserved and d is the total numberof cases in which the recommendedbehaviour was required. Compliancerates for each of the 14 componentsof the SCOT were calculated by usingthe formula 100N/D where N is thetotal number of ‘Yes’s recorded foreach component and D is the numberof applicable behavioural indicatorsthat had been observed (i.e. the totalnumber of behavioural indicatorsobserved for a component minus thenumber of ‘N/A’s recorded for thatcomponent). The overall compliancerate for undertaking a surgicalcount as recommended by theACORN accountable items standardwas calculated in the same way bydividing the total number of ‘Yes’srecorded on the SCOT by the numberof applicable behavioural indicatorsthat had been observed (i.e. the totalnumber of behavioural indicatorsobserved minus the number of ‘N/A’srecorded on the SCOT).The first component of the SCOT iscount process. Figure 2 shows the25 behavioural indicators of thecount process and the complianceobserved for each of them. Thefollowing observations are of note:ResultsThe SCOT was used in 28 proceduresover six different specialties. In all, 83nursing staff including 54 circulatingroom nurses and 29 instrumentnurses were observed by the firstauthor over 57 hours (3450 minutes)surgical time. Table 3 shows the casedemographics that provided relevantdata to be considered when a countprocess was not clearly followed. Ofthe 14 components in the SCOT, eightwere seen to occur by the researcherand six were not seen to occur (seeTable 4). the instrument and circulatingnurse were observed countingaloud (behavioural indicator1.3, n 21/d 27, 78% compliance)and together during 17 cases(behavioural indicator 1.4, n 17/d 27, 63% compliance) in the initialcount process but in subsequentand final counts only theinstrument nurse counted aloud,indicating a lack of consistency inthis process the count process wasinterrupted on many occasions.These interruptions occurredbecause the surgeon requestedassistance or additional itemsfrom the instrument nurse.Behavioural indicator 1.7 is ‘Countrecommenced if interrupted’. Fieldnotes indicated that the countprocess often resumed from thepoint it had been interrupted,instead of starting again from theitems that were being counted atthe time. the ACORN accountable itemsstandard recommends that allaccountable items should remainin their original packaging untilthey have been accounted for(behavioural indicator 1.11);however, the researcher observedthe instrument nurses removingitems from their original packaging,e.g. loading scalpel blades ontotheir respective handles orsutures onto needle holders priorto counting. The recommendedbehaviour was observed in 17of the 28 cases (n 17/d 27, 63%compliance).Journal of Perioperative Nursing Volume 34 Number 2 Spring 2021 acorn.org.aue-9
the process to determine howmany counts were needed for agiven procedure was not clear.Additional counts were undertakenin 12 cases (behavioural indicator1.18, n 12/d 27, 44% compliance).Field notes illustrated instanceswhere the most senior nurse in theroom would make the final decisionon how many counts would beundertaken, which was rarelychallenged by the scrub team. there was inconsistency in termsof who should inform the surgeonof the count outcome. Field notesindicated that most often thecirculating nurse would notify thesurgeon of the outcome of thecount (behavioural indicator 1.21,n 20/d 27, 74% compliance) butdid not always wait for a responsebefore carrying on with theirduties. Notably, the surgeon rarelyacknowledged the count outcome;however, this was not the casewhen the instrument nurse notifiedthe surgeon of the count outcome(behavioural indicator 1.20, n 7/d 27, 26% compliance).Due to the nature of the proceduresobserved and limited knowledge ofsurgeons’ preferences for particularcases it was difficult for theresearcher observing the procedureto determine whether only requirede-10accountable items and instrumentswere opened (behavioural indicator1.9, n 27/d 27, 100% compliance)and that all appropriate packs andinstruments had been checkedfor integrity (behavioural indicator1.14, n 27/d 27, 100% compliance)and x-ray detectable markers(behavioural indicator 1.15, n 27/d 27,100% compliance).Another anomaly in the countprocess was the discarding ofaccountable items by the circulatingnurse into the waste bin immediatelyfollowing the second count, ratherthan after the final count. This wasexplained to the researcher as a‘time saver’, and these items were justre-recorded as ‘correct’ for the thirdcount.No count required‘No count required’ should onlyoccur when no accountable itemsare used for the case or there is nosurgical incision that would allowaccountable items to be retained. Ofthe 28 cases observed (see Table 3),only one was classed as ‘no countrequired’ – a ganglionectomy byradiofrequency (case #6). The patientreceived a local anaesthetic and no3012instrument nurse was allocated tothe procedure.Count reliefThe ACORN accountable itemsstandard recommends that relieftime be included in the APD(behavioural indicator 6.4, n 2/d 11, 18% compliance); this ideallyoccurs whenever the instrumentor circulating nurse is relievedfor a break during a procedure(behavioural indicator 6.1, n 2/d 14,14% compliance) and also applieswhen a nurse is being relievedpermanently (behavioural indicator6.5, n 3/d 14, 21% compliance). Thisis undertaken so that if there isan issue with the final count staffinvolved with the procedure may befollowed up appropriately.Sequential and simultaneousproceduresDuring this study the researcherobserved three sequential orsimultaneous procedures. Thesecases were described in field notesas being somewhat disorganised,with up to three circulating nurseshanding up accountable itemssimultaneously to the scrub nurse.Total compliance4211Not observedObserved2478024168Component the field notes described instanceswhere instrument nurses werenot opening suture packets toshow the circulating nurse thenumber of needles in the pack.The practice of removing the paperstrip or plastic bag from aroundswabs that secured them in theiroriginal numbers was common(behavioural indicator 1.12, n 21/d 27, 78% compliance). This practicewas performed so the swabscould be folded and placed in acorner on the instrument trolley inpreparation for the first count.5574134662410802210010100472200300Number of items observed400500Figure 3: Compliance for components of the observational tool thatwere observed by the researcherJournal of Perioperative Nursing Volume 34 Number 2 Spring 2021 acorn.org.au
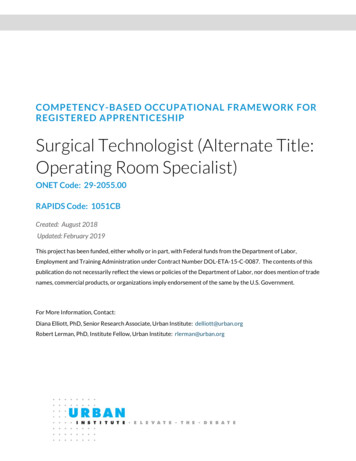
An example of the risk of suchdisorganisation was during oneprocedure the final count wasincorrect and the circulating nursejust added the extra number of itemsto the count sheet.Tray listsTray lists were attached to nearlyevery instrument tray opened bythe circulating nurse (behaviouralindicator 11.2, n 25/d 28, 89%compliance). The researcher was notalways able to see whether the listhad been signed by the sterilisationtechnician as the document wasoften discarded into the waste beforesignatures could be confirmed. Fieldobservations also confirmed thatbecause tray lists were discarded,the columns that had been providedon the tray list to count and checkoff instrumentation were not beingused by the nurses. The instrumentand circulating nurses’ details,which would assist the sterilisationdepartment in the event of anydiscrepancies in the trays returned,were also omitted from the traylist documentation. The patient’smedical record number and the dateof the procedure were also omittedas the tray list was not used in theway recommended by the ACORNaccountable items standard.Occasionally the circulating nurseswould place the tray list on thebottom of the instrument trolley, soit could be returned with the tray forreprocessing (behavioural indicator11.14, (n 21/d 28, 75% compliance).The process for countinginstrumentation was somewhatinconsistent, as some nurses countedall instruments while others countedjust a few.the worktable that did not followbest practice. When items were‘counted off’, they were not alwaysopened out fully by either theinstrument or circulating nurse(behavioural indicator 12.1, n 3/d 28, 11% compliance). Once placedin the count receptacle, they werenot recounted and the process oflabelling the bagging receptaclewith the patient’s name or numberwas not seen to occur. No countdiscrepancies were observed thatinvolved the reopening of thebagging receptacle.Observed complianceAs described, eight of the 14components of the observational toolwere seen by the researcher duringthe 28 procedures observed. Figure3 displays the compliance for eachof these eight components basedon documentation of individualbehavioural indicator items observed.The overall compliance rate forundertaking a surgical count asrecommended by the ACORNStandards was 60 per cent. Overallthere were 1268 behaviouralindicator items observed: 759complied with the ACORN Standard’srecommendations for undertakinga surgical count and 509 did notcomply. The overall compliance
Victoria Ruth Warwick Dr Fiona Stanley and Fremantle Hospital Group, vicky.warwick@health.wa.gov.au Brigid M. Gillespie Professor Griffith University - Australia, b.gillespie@griffith.edu.au Anne McMurray Professor Griffith University, School of Nursing, a.mcmurray@griffith.edu.au Karen G. Clark-Burg Professor