Transcription
JournalofDentalHygieneThe American Dental Hygienists’ AssociationJune 2013 Volume 87 Number 3 A Retrospective Comparison of Dental Hygiene Supervision Changesfrom 2001 to 2011Catalogue of Tooth Brush Head DesignsInter-Rater Reliability of the Mallampati Classification for Patients in aDental Hygiene ClinicA Survey of United States Dental Hygienists’ Knowledge, Attitudes, andPractices with Infection Control GuidelinesA Pilot Study Comparing the Outcome of Scaling/Root Planing With andWithout Perioscope TechnologyThe Attitudes of Ohio Dentists and Dental Hygienists Regarding theUse of Automated External Defibrillators in the Dental Setting - AFollow-Up StudyVol. 87 No. 3 June 2013The Journal of Dental Hygiene105
Journal of Dental HygieneVOLUME 87 NUMBER 3 JUNE 2013Statement of Purpose2010 – 2011 ADHA OFFICERSThe Journal of Dental Hygiene is the refereed, scientificpublication of the American Dental Hygienists’ Association. Itpromotes the publication of original research related to theprofession, the education, and the practice of dental hygiene.The journal supports the development and dissemination of adental hygiene body of knowledge through scientific inquiry inbasic, applied, and clinical research.presidentSusan Savage, RDH, BSDHSUBSCRIPTIONSThe Journal of Dental Hygiene is published quarterly online bythe American Dental Hygienists’ Association, 444 N. MichiganAvenue, Chicago, IL 60611. Copyright 2010 by the AmericanDental Hygienists’ Association. Reproduction in whole or partwithout written permission is prohibited. Subscription rates fornonmembers are one year, 45.SUBMISSIONSPlease submit manuscripts for possible publication in the Journalof Dental Hygiene to JoshS@adha.net.treasurerLouann M. Goodnough, RDH,BSDHpresident–electDenise Bowers, RDH, MSEdimmediate pastpresidentPamela Quinones, RDH, BSvice presidentKelli Swanson Jaecks, RDH,BSDH, MAExecutive DirectorAnn Battrell, RDH, BS, MSDHannb@adha.netEditor EmeritusMary Alice Gaston, RDH, MSEditor–in–ChiefRebecca S. Wilder, RDH, BS, MSrebeccaw@adha.netCommunicatinsdirectorRandy CraigRandyC@adha.netStaff EditorJosh Snyderjoshs@adha.netLayout/DesignJosh SnyderEditorial Review BoardCeleste M. Abraham, DDS, MSCynthia C. Amyot, BSDH, EdDJoanna Asadoorian, AAS, BScD, MScCaren M. Barnes, RDH, BS, MSPhyllis L. Beemsterboer, RDH, MS, EdDStephanie Bossenberger, RDH, MSLinda D. Boyd, RDH, RD, LS, EdDKimberly S. Bray, RDH, MSColleen Brickle, RDH, RF, EdDLorraine Brockmann, RDH, MSPatricia Regener Campbell, RDH, MSDan Caplan, DDS, PhDMarie Collins, RDH, EdDBarbara H. Connolly, PT, EdD, FAPTAValerie J. Cooke, RDH, MS, EdDMaryAnn Cugini, RDH, MHPSusan J. Daniel, AAS, BS, MSMichele Darby, BSDH, MSJanice DeWald, BSDH, DDS, MSSusan Duley, BS, MS, EdS, EdD, LPC, CEDSJacquelyn M. Dylla, DPT, PTKathy Eklund, RDH, BS, MHPDeborah E. Fleming, RDH, MSJane L. Forrest, BSDH, MS, EdDJacquelyn L. Fried, RDH, BA, MSMary George, RDH, BSDH, MEdKathy Geurink, RDH, BS, MAJoan Gluch, RDH, PhDMaria Perno Goldie, RDH, BA, MSEllen Grimes, RDH, MA, MPA, EdDJoAnn R. Gurenlian, RDH, PhDLinda L. Hanlon, RDH, BS, MEd, PhDKitty Harkleroad, RDH, MSLisa F. Harper Mallonee, BSDH, MPH, RD/LDHarold A. Henson, RDH, MEdAlice M. Horowitz, PhDLaura Jansen Howerton, RDH, MSOlga A.C. Ibsen, RDH, MSMary Jacks, MS, RDHWendy Kerschbaum, RDH, MA, MPHSalme Lavigne, RDH, BA, MSDHJessica Y. Lee, DDS, MPH, PhDMadeleine Lloyd, MS, FNP–BC, MHNP–BCDeborah Lyle, RDH, BS, MSAnn L. McCann, RDH, BS, MS, PhDStacy McCauley, RDH, MSGayle McCombs, RDH, MSTanya Villalpando Mitchell, RDH, MSTricia Moore, RDH, BSDH, MA, EdDChristine Nathe, RDH, MSKathleen J. Newell, RDH, MA, PhDJohanna Odrich, RDH, MS, DrPhPamela Overman, BSDH, MS, EdDVickie Overman, RDH, BS, MEdFotinos S. Panagakos, DMD, PhD, MEdM. Elaine Parker, RDH, MS, PhDCeib Phillips, MPH, PhDMarjorie Reveal, RDH, MS, MBAKathi R. Shepherd, RDH, MSDeanne Shuman, BSDH, MS PhDJudith Skeleton, RDH, BS, MEd, PhDAnn Eshenaur Spolarich, RDH, PhDRebecca Stolberg, RDH, BS, MSDHSheryl L. Ernest Syme, RDH, MSTerri Tilliss, RDH, BS, MS, MA, PhDLynn Tolle, BSDH, MSMargaret Walsh, RDH, MS, MA, EdDDonna Warren–Morris, RDH, MS, MEdCheryl Westphal, RDH, MSKaren B. Williams, RDH, PhDCharlotte J. Wyche, RDH, MSPamela Zarkowski, BSDH, MPH, JDPatricia A. Frese, RDH, BS, MEdJoan Gibson–Howell, RDH, MSEd, EdDAnne Gwozdek, RDH, BA, MACassandra Holder–Ballard, RDH, MPALynne Carol Hunt, RDH, MSShannon Mitchell, RDH, MSKip Rowland, RDH, MSLisa K. Shaw, RDH, MSMargaret Six, RDH, BS, MSDHRuth Fearing Tornwall, RDH, BS, MSSandra Tuttle, RDH, BSDHJean Tyner, RDH, BSbOOK REVIEW BOARDSandra Boucher–Bessent, RDH, BSJacqueline R. Carpenter, RDHMary Cooper, RDH, MSEdHeidi Emmerling, RDH, PhDMargaret J. Fehrenbach, RDH, MSCathryn L. Frere, BSDH, MSEd106The Journal of Dental HygieneVol. 87 No. 3 June 2013
InsideJournal of Dental HygieneVol. 87 No. 3 June 2013FeaturesResearch110 A Retrospective Comparison of Dental Hygiene SupervisionChanges from 2001 to 2011April V. Catlett, RDH, BHSA, MDH; Robert Greenlee, PhD118Catalogue of Tooth Brush Head DesignsMarsha A. Voelker, CDA, RDH, MS; Stephen C. Bayne, MS, PhD, FADM;Ying Liu, PhD; Mary P. Walker, DDS, PhD134Inter-Rater Reliability of the Mallampati Classification forPatients in a Dental Hygiene ClinicDiane P. Kandray, RDH, MEd; Debbie Juruaz, DDS; Mary Yacovone, MEd,RRT; G. Andy Chang, PhD140 A Survey of United States Dental Hygienists’ Knowledge,Attitudes, and Practices with Infection Control GuidelinesKandis V. Garland , RDH, MS152 A Pilot Study Comparing the Outcome of Scaling/Root PlaningWith and Without Perioscope TechnologyChristine M. Blue, BSDH, MS; Patricia Lenton, RDH, MA; Scott Lunos,MS; Kjersta Poppe, RDH, MS; Joy Osborn, RDH, MA158 The Attitudes of Ohio Dentists and Dental Hygienists Regardingthe Use of Automated External Defibrillators in the DentalSetting - A Follow-Up StudyJennifer A. Pieren, RDH, MS; Cindy C. Gadbury–Amyot, MSDH, EdD;Diane P. Kandray, RDH, MEd; Christopher J. Van Ness, PhD;Tanya Villalpando Mitchell, RDH, MSEditorials108 Dental Hygienists and Interprofessional Collaboration:Thoughts from 1927Vol. 87 No. 3 June 2013The Journal of Dental Hygiene107
EditorialRebecca S. Wilder, RDH, BS, MSDental Hygienists and InterprofessionalCollaboration: Thoughts from 1927The 2000 Surgeon General’s Report on OralHealth in American nationally recognized the importance of the connection between good oralhealth and good overall health.1 Since that time,professional groups have been conversing aboutthe need for increased collaboration and education among the various health professional groups.Interprofessional education, including dentistryand dental hygiene, has been a frequent topic atnational conferences and written about in professional publications.But the idea of different health care professionals working together is not a 21st century idea.In 1927, Ethel Covington, the first dental hygieneauthor of a paper in the Journal of the AmericanDental Hygienists’ Association (now the Journal ofDental Hygiene), wrote about the risk of specialization and how dental hygienists need to know moreabout other professions.2 Below are excerpts fromthat article:“As an auxiliary branch of dentistry, having limited field of service, we may be compared to anyspecialized group with the same grave danger ofknowing too little about the things to which ourwork is related.”“While we know the value of specialization, andthe dental hygienist is a specialist in that her field islimited to oral hygiene, it should be one of the mostimportant aims of our Journal and our AmericanDental Hygienists’ Association to keep us broadlyinformed with the greater field of which we are apart, dentistry in its relationship to better health.”On the limitations of specialization she wrote:“The Tuberculosis Associations have accomplished a noticeable reduction of tuberculosis inthe United States. Psychiatrists and the NationalCommittee for Mental Hygiene have given muchinformation on child training to parents and teachers which is manifest in the attitude of progressive mothers and teachers toward children. StateDepartments of Health, the Visiting Nurses Association, and other agencies have greatly improvedsanitary conditions and reduced the danger of epi108demics. The Red Cross, the groups of physiciansand dentists interested in health, each has a special part of the great health program to perform.Yet how little we know of the scope and the work ofthe separate groups.”“The most rapid progress and the most far reaching good will be accomplished only when there iscoordination of effort among all of these relatedhealth groups. It should be the aim and the ideal of our American Dental Hygienists’ Associationto promote high stands of service through an understanding and appreciate on the value of dentalhealth in its relationship to general health.”In 2008, a study was published on Periodontalsystemic disease education in United States dentalhygiene programs.3 One of the survey questionsasked dental hygiene program directors about interprofessional education regarding oral-systemicdisease. Only 4% indicated that they teach periodontal oral-systemic content to interdisciplinarystudent groups. When interdisciplinary teachingdid occur, it was usually with nursing or other alliedhealth students. Two program directors reportedthat their students conduct a project or patient education related to oral-systemic disease with otherhealth professions students. Hopefully the numberof dental hygiene programs who are incorporatinginterprofessional education and collaboration withdental schools or health sciences/allied/nursingprograms has increased since that time.In May, 2013, Dr. Rick Valachovic (President andCEO of the American Dental Education Association)wrote an interesting article in Charting Progresstitled, Interprofessional Education (IPE) is Here toStay.4 In it he reports that IPE is maturing. A number of dental schools now have IPE initiatives underway. One of the most interesting collaborationsis at New York University (NYU). In 2005, the NYUCollege of Nursing moved into the NYU College ofDentistry. Since that time the College of Nursinghas established a nurse faculty practice in the dental school. A benefit of that collaboration is thatnurse practitioners are frequently on the dentalclinic floor available for consultation. Twice a week,nursing faculty work with dental students as theyThe Journal of Dental HygieneVol. 87 No. 3 June 2013
chart medical histories, educating them about conditions that might impact dental treatment. Facultyfrom each program are teaching in the other programs. Interprofessional collaboration is happening with grant funding and presentations.Many schools of dental hygiene are located onhealth sciences campuses that also educate nurses, physical therapists, occupational therapists,pharmacists and other professional groups whoshould know about the importance of oral hygieneand its relationship to general health. As written byCovington in 1927, “The most rapid progress andthe most far reaching good will be accomplishedonly when there is coordination of effort among allof these related health groups.” Dental hygienistsare a vital part of the IPE team. IPE is here to stayand ADHA is working hard to make sure that dentalhygienists are a vital part of the team!Sincerely,Rebecca Wilder, RDH, BS, MSEditor–in–Chief, Journal of Dental HygieneReferences1. Oral Health in America: A Report of the SurgeonGeneral--Executive Summary. US Departmentof Health and Human Services, National Institute of Dental and Craniofacial Research [Internet]. Available from: eral/report/executivesummary.htm2. Covington E. The dental hygienists in the making. J Dent Hyg. 1927;1(1):3–6.Vol. 87 No. 3 June 20133. Wilder RS, Thomas KM, Jared H. Periodontal-systemic disease education in UnitedStates dental hygiene programs. J Dent Educ.2008;72(6):669-679.4. Valachovic R. IPE Is Here to Stay. ADEA [Internet]. Available from: http://www.adea.org/about adea/Pages/ChartingProgress.aspxThe Journal of Dental Hygiene109
ResearchA Retrospective Comparison of Dental HygieneSupervision Changes from 2001 to 2011April V. Catlett, RDH, BHSA, MDH; Robert Greenlee, PhDIntroductionAbstractSeveral factors contribute to thepoor dental health of low-incomepopulations in the U.S. Some of themost significant factors that contribute to this lack of access to care are ashortage of dentists, poor participation of dentists in public assistanceprograms and dental hygiene practice acts.1 The dental hygiene practice act supervision requirements,dictated by state dental boards, limit the dental workforce conditions.In 2006, the dentist-to-populationratio in the U.S. was 5.8 dentistsper 10,000 residents.1 In May 2010,there were over 25% more dentalhygienists as general dentists in theU.S.1 Some states are not utilizingdental hygienists to fill the need inproviding dental health care to theirunderserved populations. In a 2010survey, 1,824 dental hygienists representing 42 states reported frustrations related to their career growthdue to the trend of too many dentalhygiene programs, a reduction inbenefits and salaries, and a shortage of available dental hygiene positions.2 The dental hygiene workforceis available; therefore, it needs to beutilized.Purpose: The purpose of this study is to evaluate the extent ofchange in the professional practice environment for dental hygienists in the 50 states and District of Columbia by comparingthe state supervision requirements for dental hygienists during2001 to 2011 to the previous 7 year period, 1993 to 2000.Methods: A retrospective comparison evaluation was conducted using the 2 tables entitled “Tasks Permitted and Mandated Supervision of Dental Hygienists by State, 1993, 1998 and2000” and “Dental Hygiene Practice Act Overview: PermittedFunctions and Supervision Levels by State.” To score the netchange in supervision, a numerical score was assigned to eachlevel of alteration in supervision with a 1 or -1 for each levelof change.Results: With a 95% confidence level, the mean change indental hygiene supervision from 2001 to 2011 was 6.57 with astandard deviation of 5.70 (p-value 0.002). The mean changeof supervision from 1993 to 2000 was 2.61 with a standarddeviation of 4.36 (p-value 0.0002). The difference in the meanscores for the periods 1993 to 2000 and 2001 to 2011 was 3.96(p-value 0.06).Conclusion: This study shows that the majority of the statesare moving toward a decrease in dental hygiene supervision.Study results suggest that the movement appears to be accelerating with more states adopting fewer supervision regulationsat a faster rate. Therefore, direction is moving toward more access to dental health care for underserved populations.Keywords: dental hygiene, access to dental care, supervisionlevel, community partnerships, autonomyThis study supports the NDHRA priority area, Health ServicesResearch: Identify how public policies impact the delivery, utilization, and access to oral health care services.In addition to the shortage ofdentists in the U.S. and a lack ofdental participation in public assistance programs, public policy plays a substantialbarrier to dental care. In most states the statedental boards, which are comprised mostly of dentists, oversee the regulation of dental hygienistsand in some cases have the ability to determinewhich dental hygiene procedures may be legally performed by dental hygienists and determinewhether dental hygienists are required by law tobe directly supervised. Direct supervision limits theconditions and locations in which dental hygienistsmay provide preventive dental services; direct su110pervision confines the dental hygienist to a facilitywhere the dentist is physically present. Also, thereare state differences in dental procedures that maybe performed by dental hygienists. Over the pastdecade several states have passed legislation toallow more dental procedures to be performed bydental hygienists without the direct supervision ofa dentist. Other states have not made any changesin dental hygiene legislation over the past 2 decades.The Journal of Dental HygieneVol. 87 No. 3 June 2013
According to a study conducted in 2004 by TheCenter for Health Workforce Studies at the University of Albany, along with other previous studies,the expansion of dental hygiene professional practice acts has been shown to improve the access toand utilization of oral health care services alongwith oral health outcomes.3-7 The findings of thesestudies confirm that a decrease in dental hygienesupervision requirements in the U.S. could allowan expansion in professional practice opportunitiesfor dental hygienists. By expanding dental hygienepractice regulation, access to preventive dentalcare could be made more available in underservedpopulations, including non-traditional settings suchas schools, prisons, nursing homes and privatehomes, for homebound individuals. Some states,such as Colorado, Washington, Oregon, California and New Mexico, have had more lenient scopeof practice and dental supervision laws which hasresulted in more access to dental health care fortheir underserved populations.3 By allowing dentalhygienists to serve individuals in nursing homes,public health clinics and rural areas there is a higher access to dental care with no effect on the number of patients seen in dental offices since theseindividuals are not accessing care in a private dental office. Mandating dentists’ physical presence forthe provision of dental hygiene care is unnecessarysince there is little possible danger in most dentalhygiene services provided.3 And states that haveallowed dental hygienists to provide unsupervisedservices to more medically compromised individuals in long-term facilities, dental hygiene programsand to homebound patients have determined dental hygienists should be allowed to serve patientswho are less medically compromised in all dentalsettings unsupervised.3According to the previous Surgeon General David Satcher, oral health is an integral part of general health, and in his 2000 report, Oral Health inAmerica, he stated that dental caries is a “silentepidemic.”4 Most dental conditions may not be lifethreatening and may be easily treated, but thereare some dental conditions that result in pain, lossof teeth, infection, severe disability or even death.Early diagnosis and treatment of dental conditions,such as oral cancer, are important to ensure a goodquality of life.5 Studies have shown how the prevalence of dental caries is historically higher amongthose who live in poverty and rural areas and in minority groups.4,6,7 Low-income and minority familiesexperience 80% of all dental conditions, but onlyaccount for approximately half of the total numberof dental visits in the U.S.6 In 2005, almost 3 outof 4 shortage areas of dental health professionals were in rural areas where families experiencetransportation barriers and had reduced access toVol. 87 No. 3 June 2013community water fluoridation.5 Lacking a dentalhealth care provider is a major risk factor for receiving inadequate preventive dental health care.A 2000 national survey of physicians found that38% of patients enrolled in Medicaid and 55% ofuninsured patients encountered difficulties in making a dental appointment with a dentist.6Public policy has attempted to address the shortages in access to dental health care by providingincentives to dentists who serve low-income populations (thereby increasing the supply of dentistsin rural areas), by using medical health care providers to provide dental health care services (suchas fluoride varnish treatments) and by encouragingforeign dental school graduates to become licenseddentists in the U.S.5,8-10 These attempts have resulted in little or no success in an increase in dental health care access. The National Conferenceof State Legislatures has recommended that eachstate consider dental hygiene licensing arrangements that will improve access to dental healthcare for underserved families.6 A study performedby the National Center for Health Workforce Studies suggests that there is a positive correlation between access to dental health care and the autonomy of dental hygienists.3Methods and MaterialsA retrospective comparison evaluation was conducted using the 2 tables. “Tasks Permitted andMandated Supervision of Dental Hygienists byState, 1993, 1998 and 2000,” was developed ina study funded by the National Center for HealthWorkforce Analysis Bureau of Health ProfessionsHealth Resources and Services Administration inApril 2004. “Dental Hygiene Practice Act Overview:Permitted Functions and Supervision Levels byState” was developed by the American Dental Hygienists’ Association in June 2011 (Tables I, II).3,11The scoring instruments were designed by the initial researchers to quantify particular aspects ofthe legal practice acts and board regulations fordental hygienists within each state which permitgreater access to dental hygiene services particularly for underserved populations.3,11 The comparison of these 2 tables details the net change inthe state supervision level required for 11 dentalhygiene tasks from 2001 to 2011. The 11 dentalhygiene tasks selected were intended by the initial researchers to capture characteristics of professional dental hygiene practices that enable dental hygienists to provide dental services and werebased on conditions that are perceived to affectaccess in a variety of dental hygiene settings.3,11In order to score the net change in state dentalhygiene supervision, a numerical score, which wasThe Journal of Dental Hygiene111
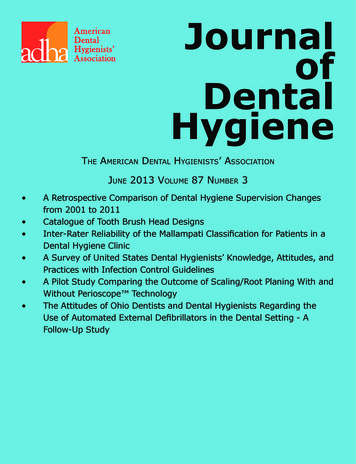
Table I: Change in Supervision Levels for Dental Hygienists by State, 1993 to erio.DressingsRemovalof SuturesMonitorN2OAdminN2OAdmin 1006StateKey:0No Change 1 to 21Degree of Decrease in Supervision Requirements-1 to -21Degree of Increase in Supervision Requirementsdeveloped by the National Center for Health Workforce Analysis Bureau of Health Professions HealthResources, was assigned to each state’s supervision level in each year as follows: 0123-Direct SupervisionIndirect SupervisionGeneral SupervisionNo SupervisionAfter each numerical value was assigned to eachsupervision level for each year, the level of supervision numbers for the 11 dental hygiene tasks inthe year 2001 were subtracted from the level ofsupervision numbers in that same dental hygiene112task for the year 2011. This occured for each of the50 states and the District of Columbia.3Each dental hygiene preventive service and extended occupational task was totaled to calculate amean change for each task, a net change for eachstate and a net change for each task. Then, a totalmean change and a total net change was calculatedfor all 50 states and the District of Columbia from2001 to 2011 to evaluate the degree of supervisionrequirement changes that has occurred during thatdecade for the entire U.S.3This review of documents provides a longitudinaldescription of the level of required supervision forThe Journal of Dental HygieneVol. 87 No. 3 June 2013
Table I: Change in Supervision Levels for Dental Hygienists by State, 1993 to 2000 alantsPerio.DressingsRemovalof SuturesMonitorN2OAdminN2OAdmin 5Key:0No Change 1 to 21Degree of Decrease in Supervision Requirements-1 to -21Degree of Increase in Supervision Requirementsthe fundamental dental hygiene preventive services and some extended occupational tasks for eachof the 50 states and the District of Columbia from2001 to 2011. In some states, negative changeoccurred, suggesting that the level of supervisionincreased. Each score can be interpreted using thefollowing method:3 0 - No Change 1 to 21 - Degree of Decrease in SupervisionRequirements -1 to -21 - Degree of Increase in SupervisionRequirementsVol. 87 No. 3 June 2013To evaluate how much change has occurred inthe level of supervision for the dental hygiene profession between the years 2001 to 2011 comparedto the years 1993 to 2000, a bivariate analysis ttest was performed utilizing the OpenEpi program.12The greatest threat to the validity of this study includes improper measurement errors which wouldaffect reliability. Therefore, data entry was verifiedtwice by the author. Using an ordinal scale of supervision level (0, 1, 2, 3) for each dental hygienetask, a mean score was given for each time frameby totaling all state ordinal scale scores and dividing them by 51.The Journal of Dental Hygiene113
Table II: Change in Supervision Levels for Dental Hygienists by State, 2001 to erio.DressingsRemovalof SuturesMonitorN2OAdminN2OAdmin 1110000-1-113StateKey:0No Change 1 to 21Degree of Decrease in Supervision Requirements-1 to -21Degree of Increase in Supervision RequirementsResultsWith a 95% confidence interval, the meanchange in dental hygiene supervision from 2001to 2011 was 6.57, with a standard deviation of5.70 (p-value 0.002). The positive value of 6.57indicates that the 11 dental hygiene tasks acrossthe 50 states saw an average movement towardless required supervision for dental hygienists. Asimilar trend toward reduced average supervisionrequirements was observed between 1993 and2000 (however, this trend was nominally smallerdue to a shorter time frame). The mean changeof dental hygiene supervision from 1993 to 2000was 2.61,with a standard deviation of 4.36 (p-value 0.0002). The difference in 2 means between114the period 1993 to 2000 and the period 2001 to2011 is 3.96 (p-value 0.06).Some states, such as Virginia, Kansas and Missouri, have made substantial change in supervision regulations in the past 10 years. Other statessuch as Alabama, Georgia, Mississippi and NorthCarolina have made little or no progression inchanging dental hygiene regulations from 1993to the present date. There has been an overallchange in more tasks permitted for dental hygienists, in regards to supervision, over the past 10years. Numerically, a change toward less supervision requirement occurred in 45 of the 51 jurisdic-The Journal of Dental HygieneVol. 87 No. 3 June 2013
Table II: Change in Supervision Levels for Dental Hygienists by State, 2001 to 2011 alantsPerio.DressingsRemovalof SuturesMonitorN2OAdminN2OAdmin Key:0No Change 1 to 21Degree of Decrease in Supervision Requirements-1 to -21Degree of Increase in Supervision Requirementstions, and a change toward more supervision requirement occurred over the past 10 years in only5 jurisdictions. There are still some states that require direct supervision in all settings: Alabama,Georgia, Mississippi and North Carolina. There arenow 35 states that allow direct access, where thedentist does not need to examine or authorizethe dental hygiene services in public health settings outside of the dental office.11 An additional3 states do not require a dentist to examine thepatient prior to dental hygiene services in publichealth settings outside of the dental office: Indiana, New York and South Carolina.11In regards to a reduction of supervision for inVol. 87 No. 3 June 2013dividual dental hygiene tasks, the largest meanchanges occurred in coronal polishing (1.12),the application of sealants (1.1), the applicationof fluoride treatments (1.08), taking radiographs(0.094) and performing scaling and root planing(0.84). The only dental hygiene task that now requires more supervision in 2011 than in 2001 isplacing an amalgam filling, with a mean score of-0.02, which is a restorative service and traditionally outside the scope of practice for dental hygienists as defined by state dental boards. With thehigher number of dental hygiene graduates overthe number of dental school graduates, it wouldseem logical to utilize these dental care providersto provide scaling and root planings, apply seal-The Journal of Dental Hygiene115
ants and fluori
asked dental hygiene program directors about in-terprofessional education regarding oral-systemic disease. Only 4% indicated that they teach peri-odontal oral-systemic content to interdisciplinary student groups. When interdisciplinary teaching did occur, it was usually with nursing or other allied health students. Two program directors reported